











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Most people have a suitable place to sleep and rest, have set times for meals, have access to healthcare when they are ill, and can receive the necessary care. When a person finds themselves in a situation where they have no home and no financial or material resources, their basic needs are affected and access to healthcare can be difficult (Hopkins & Narasimhan, 2022; Viegas et al., 2020). Encouraging self-care among homeless people involves building participatory and co-responsible care in the face of a social, historical, global, multifaceted phenomenon with various implications experienced on the streets, such as prejudice, fear, violence in its various dimensions, and the violation of basic human rights such as access to health, education, housing, employment, income, and leisure (Silva et al., 2020).
1. Theoretical framework
Self-care is an important attitude for promoting health and reducing harm. For this reason, bringing homeless people into care planning is an important emancipatory intervention, as it places them at the forefront of self-care within their real context. With active participation, there are opportunities to enhance their individual, social, and collective capacities and to create conditions conducive to comprehensive and safe care within each person's reality (Ximenes et al., 2021). To achieve this, it is necessary to go beyond the dimension of care that occurs in behaviours and procedures, prescriptions and standardisations, in order to value the life projects of others in their individuality and subjectivity (Silva et al., 2018).
This study will analyse the concept of self-care based on Dorothea Orem's Self-Care Theory, which consists of actions that promote personal development and well-being. These actions occur at specific times and help develop individualised care strategies, identifying self-care deficits to establish, according to unique conditions, educational support systems, either partially compensatory or fully compensatory, with the aim of preserving life and improving quality of life (Orem, 1980).
Given the need for care and self-care, a moralistic, negative and prejudiced perspective on the living conditions and behaviour of homeless people compromises access to and continuity of care for these individuals, as it results in consequences such as social isolation, deterioration in their quality of life and reduced self-esteem. This stigma is often experienced by people living on the streets, and when combined with distance from health and social services, it increases their vulnerability. Alternatively, health professionals can also be impacted by this social imagery, which affects the care provided to these individuals. In other words, prejudice generates a cycle of exclusion that impacts both the person being cared for and the professionals, hindering the implementation of care and inclusion policies (Teixeira et al., 2019).
Due to precarious socioeconomic conditions and living on the streets, people are more vulnerable to infection, illness, and worse clinical outcomes, which is directly related to the lack of self-care and timely and effective treatment, resulting in the need for complex and interdisciplinary care (Silva, 2021).
It is difficult for homeless people to become aware of effective self-care without interaction between the health service, the professional and the person being cared for. Thus, the construction of self-care needs to be understood in the various ways of caring for oneself and others, in addition to the factors that influence this practice and the relationships established (Silva, 2018).
In Brazil, in large urban centres, care for homeless people is provided by the Street Clinic team, either on site with mobile units or in fixed units, on an itinerant basis. The street clinic team works in collaboration with other Primary Health Care teams, such as the Family Health Strategy, which offers continuous support to individuals, families and the community, and the Multidisciplinary team, with support from professionals from different disciplines. In addition, the street clinic team coordinates actions with the Psychosocial Care Centres, which care for people with mental disorders, with the Urgent and Emergency Care Network for situations that require immediate attention, and with the services of the Unified Social Assistance System, which provides social assistance support. These integrations also include public entities and civil society organisations, forming an integrated care network (Brazil, 2017).
In municipalities without street outreach teams, homeless people need to be able to refer to the primary healthcare/family health strategy teams responsible for the areas where they live or spend time.
This study considered the daily routine of primary healthcare/family health strategy teams in two municipalities without street clinics that provide care to these individuals. Given this context, the question arises: how do primary health care/family health strategy teams develop strategies to strengthen self-care and reduce harm for homeless people? Thus, the study aims to understand the implementation of self-care and harm reduction strategies for homeless people and the experiences of primary health care professionals in caring for these individuals.
2. Methods
2.1 Type of study
Qualitative study using Grounded Theory (Strauss & Corbin, 2008) and Symbolic Interactionism (Blumer, 1969) as a theoretical framework. For greater reliability in the data presented, the recommendations of the Consolidated Criteria for Reporting Qualitative Research (COREQ) guide were followed (Souza et al., 2021).
2.2 Participants
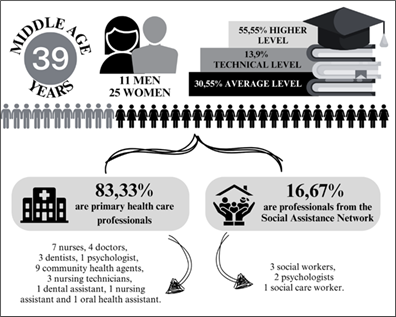
Participants were recruited conveniently, through a face-to-face approach, totalling 36, of whom 30 are primary health care professionals, distributed across six family health strategy teams, in addition to six representatives from the Social Assistance Network, from two different services, a Shelter and the Specialised Reference Centre for Homeless People. There were no negative responses to participation in the interviews.
Figure 1 illustrates the characteristics of the professionals who participated in this study. Participants were aged between 22 and 59 years old, with a predominance of females. In terms of qualifications, most had a bachelor's degree, and professional experience in the field ranged from 1 to 28 years.
2.3 Data collection
Data collection took place at the participants' workplace, in private rooms, ensuring privacy, confidentiality, and comfort for the research participants. In order to guarantee the quality of the research, the first three interviews were supervised by the supervising researcher, as part of the initial training of the researcher in charge and the student in scientific initiation.
Participants in the Social Assistance Network were invited as key informants for this study, as the Family Health Strategy professionals interviewed highlighted the collaboration of these professionals. To this end, in order to deepen understanding of the existing intersectoral relationship, interviews were conducted with professionals from the teams at the Specialised Reference Centre for Homeless People and the Shelter for Homeless People.
The inclusion criterion was that the professional had more than one year of experience in primary health care, and those who were absent due to holidays or leave during the data collection period were excluded. Data were collected using the method proposed by Strauss and Corbin (2008). The interview guide was tested beforehand and included questions related to the characterisation of participants, as well as open-ended questions addressing experiences in caring for homeless people in the context of primary health care.
The interviews took place between January and November 2022, lasted an average of 20 minutes, and were recorded digitally for transcription and subsequent analysis. The transcribed interview was sent to the interviewee for evaluation and validation of the recorded content. Microsoft Word® was used for transcription and analysis organisation.
2.4 Data analysis
Data analysis took place immediately after each interview, in accordance with the principles of Grounded Theory, considering the first stage of analysis, open coding, which was done line by line to identify meanings/concepts, searching for similarities and differences, categorising the codes in vivo or creating properties. After data collection was completed, the second stage, axial coding, proceeded. In this stage, the in vivo codes were regrouped into categories so that they re(signified) the phenomenon under investigation. In the third stage, selective coding, the categories were integrated and refined in order to name the central category. Throughout the analysis, coding for the process took place, which consists of the purposeful observation of the action/interaction of meanings, which enables the connection between categories. In the data analysis, memos were also used, consisting of notes made by the interviewer based on the operational stages of the research, observations and reflections throughout the interview process (Strauss & Corbin, 2008).
Data saturation was achieved in the 34th interview when the meanings clearly presented the definition of the categories in their properties and dimensions to describe and interpret the phenomenon under investigation (Strauss & Corbin, 2008). To confirm saturation, two more interviews were conducted, reinforcing the analytical basis and validity of the study.
2.5 Ethical issues
All participants in this study signed a Free and Informed Consent Form in duplicate. The study followed ethical guidelines for research involving human subjects in all stages. The research was approved by opinion 5.173.172 of the Human Research Ethics Committee of the Federal University of São João del-Rei - Midwest Campus.
3. Results
The data-based theory that emerged from this study was derived from five theoretical categories originating from 10 subcategories and 40 in vivo codes, named after the central category that gave the master's thesis its title: ‘Care for homeless people in municipalities without street clinics: from access to tackling inequalities’.
In this article, we will discuss the category ‘Difficulties in implementing self-care strategies for homeless people,’ presented in Figure 2, which highlights the challenges faced by these individuals in adopting self-care practices and preventing risks and health problems, from the perspective of health professionals and the social assistance network. The in vivo codes that gave rise to this category reveal aspects such as resistance to rules and guidelines, difficulties in adhering to care strategies, limitations in access to health education, and challenges in promoting self-care in the face of the adverse conditions faced by these individuals. These elements reflect structural and subjective barriers that directly impact the effectiveness of health actions aimed at homeless people, especially in municipalities without street clinics, in a context that reinforces inequalities in access to health care.
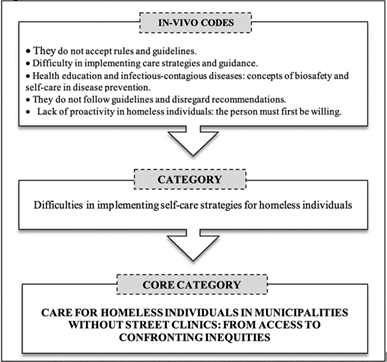
Figure 2 Category “Difficulties in implementing self-care strategies for homeless people” and in vivo codes, two municipalities in the Central-West region of Minas Gerais, Brazi
In the realities researched, the participants in this study were unanimous in their view that homeless people do not accept rules or guidance:
It's difficult, because they're homeless, they don't accept the rules, they would come here to the unit, turn on the radio, then we would ask them to turn off the radio, they didn't want to turn off the radio (E1).
They have a lot of difficulty following rules. One even said to me: ‘That's why I live on the street, because I don't like rules’ (laughs). But then I said that in order for you to receive care, there have to be rules, because otherwise it's difficult for us to control (E3).
Because they have rules at the shelter, sometimes they don't adapt to the rules; they leave and go back to the streets, and then we lose that continuity of care (E32).
Many arrive here from the streets, and on the streets there are no rules: ‘my space, my rules.’ When they arrive here, there are rules, and then they start to go crazy (E35).
According to professionals, in everyday life, people living on the streets do not follow the guidance of the health team and do not comply with care recommendations:
But they don't follow the guidelines. We advise them one thing, [...] they don't come back for a dressing change the following week (E2).
Thus, primary health care teams report that they face difficulties in implementing strategies for care and guidance for self-care, harm reduction, and health promotion:
It is difficult to carry out health promotion activities with them because it is difficult to reach them, difficult to gain their acceptance, and very difficult to keep track of this population. Today, I don't see a new way; I can't think of anything other than the traditional way (E31).
Faced with nomadism and treatment abandonment, continuity of care does not occur, and professionals' experiences are of responding to spontaneous demand:
There is no way to plan much. This population is very fluid; there is no way to link them to the health unit [...] There is no point in my wanting to register them, link them, because next week they will be on the other side of town (E33).
What happens with them is that they don't take care to return for that care. It starts and then stops. If you don't go after them, they don't come back (E5).
The biggest difficulty we have is continuity of treatment. These patients who are homeless, in general, do not remain in the city, they migrate, so it is difficult for us to get any adherence (E8).
The fragmentation of the Healthcare Network also seems to influence continuity of care due to the lack of counter-referrals:
Here, in the situation we live in, the RAS is very fragmented, extremely fragmented (E22).
The reality of health education, preventive measures against infectious diseases, and biosafety concepts is characterised by:
There was a patient there who had tuberculosis, so [...] they were desperate, afraid of catching tuberculosis, and kept calling here at the family health strategy, so I had to go there to advise them (E1).
They are very afraid, as we saw several patients on the same day. They were very afraid, for example, one would enter the office, and when he left, the others would ask: "Did you clean everything? Did you sterilize everything? Because he has hepatitis. [...] I saw that in them, the care they want for themselves (E3).
According to the professionals interviewed, there is a lack of proactivity among homeless people because, first of all, the person has to want it:
I'll be honest, first the person has to want it, because if they don't want it, you can try to do whatever you want, but they won't accept help [...] the first thing a homeless person has to want is to improve their situation, because in life, everything is about wanting. If I want to improve and I have these possibilities, just like I do now, I'll go for it (E6).
So, it depends on the user too, not just the team. The team is doing its part, but they also have to want to be treated. [...] the user also has to do their part, they have to want it, and it's very difficult (E21).
The realities researched are from large municipalities in the state of Minas Gerais, Brazil, without street clinics, with different ways of organizing daily work to care for homeless people, since one of them has a Specialized Reference Center for Homeless People, while in the other, services are provided by the Social Assistance Reference Center and the Shelter. Specific actions by primary health care teams in response to spontaneous demand were highlighted. The Community Health Agent contacts the institutions in the social assistance network to refer the demands to other professionals in the team, as well as identifying people on the streets (Memorandum).
There is one that I have tried to take in several times, because his foot is very swollen, he has vein problems, but he refuses treatment. He says he can go to the emergency care unit. So I've approached him, I've tried several times to bring him here, but I think he's afraid we'll take him to some kind of permanent shelter, so he ends up rejecting it, and he stays there, whatever will be, will be (E26).
The lack of proactivity among homeless people in terms of self-care determines the experience of spontaneous demand in conditions of illness that could have been avoided through harm reduction or monitored by health services before becoming more complex (Memorandum).
And it could further increase their interest, because they themselves are not concerned about it. When their concerns arise, it is because things are already very bad. So there could be more interest on their part (E34).
4. Discussion
Self-care and harm reduction are essential measures for protecting health. However, homeless people often face difficulties in caring for themselves effectively due to the adverse conditions imposed by homelessness and the vulnerabilities inherent in this context (Viegas et al., 2021). This population group depends largely on the solidarity of third parties and institutional and intersectoral actions to enable self-care practices for harm reduction, either due to a scarcity of individual resources or insufficient public policies for these individuals (Nascimento et al., 2022).
Vulnerable conditions intensify the risks of health problems in people who are deprived of resources, which is corroborated by Orem's Theory, which states that universal self-care needs are not being met, resulting in a self-care deficit. However, it is essential to emphasise that the challenges of lack of resources can be mitigated through a strengthened educational support system (Orem, 1980). This support is understood as a set of intersectoral strategies aimed at promoting autonomy, access to rights, and improving living conditions in order to guarantee support for people so that they can develop or recover their self-care capacity (Macedo et al., 2021) or at least reduce harm.
Loss of self-esteem and lack of concern for self-care are real situations faced by homeless people, associated with poor health conditions and insufficient resources to sustain life, in the face of daily suffering and a lack of prospects for the future (Hino et al., 2018).
Self-care among homeless people is deeply related to their ways of living and the common-sense knowledge acquired through social relationships. Therefore, self-care strategies must recognize this knowledge as legitimate, as it contributes to harm reduction. Valuing these practices in care planning strengthens bonds and promotes changes in attitude, both at the individual and collective levels (Silva et al., 2020).
Caring for others is a common practice among homeless people, as social exclusion means they do not recognize health as a right. They experience solidarity within the group in terms of care and use common sense knowledge and treatments to recover their health on the streets. As such, they only resort to health services in urgent and emergency situations (Silva et al., 2018).
A study conducted in Mato Grosso, Brazil, pointed out that even though homeless people are aware of the importance of self-care and harm reduction in the consumption of psychoactive substances, they do not implement known strategies, claiming that the consumption of these substances provides an anesthetic effect on the problems they face on the streets (Nascimento et al., 2022). These results corroborate those of this study, in which professionals report difficulty in developing self-care strategies with these individuals, as they are unable to prevent conditions of vulnerability and follow the guidelines and recommendations provided.
It is essential to recognize that there is no single ideal form of care for all people. Care must be tailored to individual needs, with harm reduction measures and a comprehensive approach, respecting the autonomy and wishes of those receiving care. Soft technologies, such as welcoming and bonding, are essential for strengthening autonomy. Rather than prescribing behaviors or encouraging self-care, professionals should consider the subjectivities and life trajectories of these individuals (Viana et al., 2020).
A study conducted in the Netherlands found that low adherence to treatment was not only related to homeless people, but also to the characteristics of the health service. It also establishes that care practices need to be rethought so that unique and longitudinal care is provided to overcome stigmatizing behaviors and prescriptive treatments that do not consider the conditions of the person being cared for (Klop et al., 2018). It is necessary to experience humanizing practices with respect for dignity in order to achieve accessibility and equity (Viegas et al., 2021).
The results of this research confirm evidence from a study in Rio de Janeiro, which identified prejudiced and stigmatizing practices against homeless people, including by health professionals and other users. In these situations, care was conducted in an authoritarian manner, limiting autonomy, especially among alcohol and other drug users who suffered double stigmatization. Their desires and choices were disregarded, subjecting them to the values and beliefs of professionals, which deepened processes of exclusion. The lack of technical and ethical preparation of professionals reveals practices based on individual conduct, disregarding the subjectivity and vulnerabilities of these people (Brito & Silva, 2022).
When considering nomadism, providing longitudinal care to homeless people becomes complex and challenging. The street clinic team makes it possible to provide care beyond homes, families, and institutions, making it available on the streets according to the rhythms of life, desires, and trajectories (Freitas & Justo, 2019). Thus, this team mitigates prejudices, overcomes barriers to access, and reduces indifference in caring for homeless people (Brito & Silva, 2022). A study with professionals from the street clinic team in the municipality of Rio de Janeiro, Brazil, shows that caring for these people on site was associated with increased self-esteem and the promotion of self-care (Teixeira et al., 2019).
A study conducted in Campina Grande, Paraíba, Brazil, showed that it is necessary to go beyond the health-disease process to provide comprehensive care to homeless people, and that it is essential to consider lifestyle habits and barriers that hinder access and effective treatment with planned and intersectoral professional action. The fragmentation of the Health Care Network is another setback in the development of self-care strategies for homeless people, since the lack of communication and weakened intersectoral action make comprehensive and individualized care, early detection, treatment, and follow-up of cases unfeasible (Queiroga et al., 2018).
Risky behaviors such as drug use, prostitution, sharing sharp objects, physical violence, unprotected sex, etc., require qualified, welcoming assistance and encouragement to take care of oneself (Patrício et al., 2020). It is imperative to abolish professional practices that contribute to discrimination and neglect. Prejudice affects various aspects of a person's life, generating feelings of shame and humiliation and distancing them from health services. These experiences impact the self-image and self-esteem of homeless people and promote neglect in care (Brito & Silva, 2022).
Despite the adversities faced by health professionals in developing shared self-care strategies, this context opens the door to reflections on the development of harm reduction actions that enable homeless people to recognize their health condition and make safe choices, without demands, with their autonomy and discernment guaranteed. Health professionals are essential actors in promoting self-care with qualified care, as educators and advisors. A welcoming attitude will favor longitudinal follow-up and closer ties with health services (Ximenes et al., 2021), enabling the person receiving care to be a co-participant and co-responsible for maintaining their health (Nascimento et al., 2022).
Taking care of oneself on the street is a difficult reality. Intersectoral actions favor shared knowledge and action, since self-care is not only about biomedical care, but also involves safety, education, social promotion, and the guarantee of human rights, in addition to valuing culture, beliefs, knowledge, and individual values. To enhance shared self-care, autonomy and self-determination must be enabled. Care encounters must be free from prejudice, stigma, and hygienist actions. Intersectoral action should promote social reintegration, the re-establishment of bonds, the promotion of employment, income, and citizenship, and the guarantee of full participation by the actors involved (Silva et al., 2020).
The way of expressing how others should live or act can have a colonizing and imprisoning effect, using words as instruments of control and punishment, imbued with stigma and prejudice, which favor exclusion and result in obstacles to access to comprehensive healthcare and the exercise of citizenship (Moreira et al., 2024).
In light of Symbolic Interactionism (Blumer, 1969), it is understandable how complex the implementation of self-care is in the context experienced by homeless people, given that human actions are influenced by various elements, with their conduct being shaped by the interpretation of these actions. Guidelines for recurrent self-care are not followed because desires, needs, and goals are not considered. This affects self-care, since behavior is modified and can be guided by the image that the person has of themselves and others in relation. In the context of this study, self-care is influenced by the interactions between the subjects involved, and can be initiated, abandoned, postponed, confined to intention or fantasy, or even transformed and become sensitive and lived.
5. Limitations of the study
One limitation is the intentional sampling justified by the theme, which focuses on homeless people in municipalities without street outreach teams. Although the sampling was intentional, it was diversified by the inclusion of research participants from various professional categories and intrasectoral and intersectoral care networks, which led to a theoretical sampling, as proposed by the methodological framework of Grounded Theory. As this is a qualitative research study, the results can be theoretically generalized to similar situations.
This study contributes to the care of homeless people in situations where there are no specific teams, providing support for managers, health professionals, and the Social Assistance Network.
Conclusion
Self-care in health cannot be dissociated from the guarantee of fundamental rights to life, which includes people having a safe place to live, enough to eat, the means to care for themselves, and timely access to health services. More than just providing services, it is essential that primary health care professionals are trained and sensitized to adopt humanized and inclusive practices, free from stigma, ensuring care that respects the unique characteristics of homeless people.
Encouraging self-care does not mean imposing rules, but rather building a welcoming environment in which people feel proactive and jointly responsible for the therapeutic process. The adoption of intersectoral and supportive actions reduces inequalities and expands access to health care. The care that is possible is that which is appropriate to individual needs, limitations, and expectations, ensuring dignity and autonomy. In this sense, the street clinic team plays an essential role in strengthening bonds and adopting harm reduction strategies, sharing responsibilities with people living on the streets to take care of themselves, with unique support systems.
However, in municipalities that do not have street clinics, the challenges are even greater, as the absence of specialized teams limits the provision of care tailored to the needs of this population. A form of support provided by family health strategy teams can broaden this approach, making health actions more accessible and effective for homeless people. Thus, the promotion of self-care must be linked to the implementation of public policies that guarantee basic rights, associated with the continuous training of primary health care teams.
More than offering guidelines on self-care, it is essential to create real conditions for these people to be able to practice it, overcoming structural barriers and ensuring truly inclusive, dignified, and humanized care. The results of this study contribute to the health sector and other sectors of society, reinforcing the importance of working with people who experience vulnerability on the streets to develop unique and realistic self-care practices, with intersectoral and supportive actions.
Author´s contribution
Conceptualization, L.G. and S.V.; data curation, L.G., B.S. and S.V.; formal analysis, L.G., B.S. and S.V.; funding acquisition, S.V.; investigation, L.G., B.S. and S.V.; methodology, L.G. and S.V.; project administration, L.G. and S.V.; supervision, S.V.; validation, L.G., I.D., H.Q., F.L. and S.V.; visualization, L.G., B.S., I.D., H.Q., F.L. and S.V.; writing- original draft, L.G., B.S., I.D., H.Q., F.L. and S.V.; writing- review & editing, L.G., B.S., I.D., H.Q., F.L. e S.V.

