










Serviços Personalizados
Journal

Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
 Citado por SciELO
Citado por SciELO Links relacionados
 Similares em
SciELO
Similares em
SciELO Compartilhar

 Permalink
PermalinkPsicologia
versão impressa ISSN 0874-2049
Psicologia vol.17 no.1 Lisboa jan. 2003
https://doi.org/10.17575/rpsicol.v17i1.437
Documenting delay and disability in early development with the who - ICF
Classificação do atraso e da incapacidade no desenvolvimento precoce com a CIF -OMS
Rune J. Simeonsson1; Susana Pereira2; Anita A. Scarborough3
1-2School of Education & FPG Child Development Institute, University of North Carolina at Chapel Hill, NC USA.
3Susana Pereira, Faculdade de Psicologia e Ciências da Educação, Universidade do Porto.
ABSTRACT
While iniciatives to prevent or reduce developmental delay in young children are well established in Portugal and other European countries, inadequate documentation of childhood disability introduces significant variability in the description of children served in early intervention programs. This variability contributes to problems of standardizing eligibility criteria, uniform description of the population as well as to the derivation of incidence and prevalence estimates.
Key-Words Developmental delay, childhood disability, ICF, functional limitations, early childhood intervention.
RESUMO
As iniciativas para prevenir ou reduzir o atraso de desenvolvimento em crianças estão bem estabelecidas na UE e em Portugal, mas o uso de anadaptadas formas de classificação e registo de incapacidade na infância introduz significativa variabilidade na descrição das crianças em programas de intervenção precoce. Isso acarreta problemas na definição de critérios de elegibilidade, na descrição uniforme da população e na derivação das estimativas de incidência e prevalência. É assim necessário um método abrangente de classificação e documentação que possa abarcar as dimensões de incapacidade e limitações funcionais nos primeiros seis anos de vida. A Classificação Internacional de Funcionalidade, Incapacidade e Saúde (CIF) da OMS, 2001, fornece um referencial universal para definir a funcionalidade, actividade, participação e factores ambientais. A Classificação Internacional das Doenças (CID-10) permite atender a condições de saúde específicas que essas crianças possam acumular, fornecendo informação complementar sobre as etiologias, condições de saúde e manifestações funcionais de deficiência. Neste artigo, descreve-se um recente algoritmo que integra os códigos dessas duas classificações em 4 categorias principais correspondentes ao modelo da CIF. Esse sistema de classificação tem vindo a ser largamente aplicado nos EUA, na codificação de razões de eligibilidade (National Early Intervention Longitudinal Study) sendo, também, descrita a experiência da sua adaptação em Portugal, com sucesso, na classificação e documentação das características das crianças em intervenção precoce.
A comprehensive method of documentation is needed that can encompass the dimensions of childhood disability and functional limitations in the first six years of life. The International Classification of Functioning, Disability and Health by the World Health Organization - ICF (WHO, 2001) may meet this requerement by providing a universal framework defining functioning, activities, participation and environmental factors. Given that children with disabilities also present with specific health conditions as well as functional manifestation of disability. To this end, an algorithm is described that integrates ICF and ICD - Conditions, Body, Functions & Structures, Activitiees and Participation and Environmental Factors. This calssification approach has been applied in coding reasons for eligibility in the National Early Intervention Longitudinal Study in the US and has been successfully adapted for documenting characteristics of children in early intervention in Portugal.
Recognition of the rights of individuals with disabilities was an important accomplishment in the latter part of the 20th century. These rights took the form of community rather than institutional based care for adults and the provision of special education for school age children. A logical consequence of these efforts was a downward extension of services to prevent or reduce the manifestation of disability in the infant and young child. The result has been that early intervention programs for infants and young children identified as experiencing developmental delays or being at risk for such delays has emerged in the last two decades as an important human service priority in many Western countries. Family members, advocates and service providers advanced the rationale for early childhood intervention on the basis of a framework of children's needs to promote their health and development and prevent disability. The rationale for early childhood intervention builds on a rights framework as elaborated in the UN Declaration of the Rights of the Child and the Standard Rules for the Equalization of Opportunity. This is in keeping with Lansdown's position (2000), emphasizing that the basis for services to the child should rest on the rights of the child and not on the good will of adults. Building on the broad statement of rights for all children, article 23 of the UN Declaration in particular provides a comprehensive framework to address specific rights applicable to children with disabilities.
Now, at the beginning of the 21th century, the field of early intervention is well established with the goal of preventing or reducing developmental delay and disabilities in young children. While the nature of early intervention services may vary from one country to another, most programs share several common elements: viewing the child and the family together as the client, the need for individualized interventions, an interdisciplinary approach to delivery of services and an acknowledgment of family preferences for services and supports (Bailey et al, 1998).
The conceptualization of the child and family as the unit of intervention is consistent with the shift from the medical model of disability to a biopsychosocial model. A fundamental premise of the biopsychosocial paradigm of disability is that the environment plays a central role influencing human functioning and participation. This assumption of a person environment interaction is reflected in a shift of focus in early intervention from treatment of impairments within the medical model, to enhancing the performance of daily activities, participation and quality of life within the biopsychosocial model (Dennis et al., 1993; Simeonsson & McDevitt, 1999). For the child, the focus is on promoting social integration and participation in life with peers. For the family, the focus is on reinforcing the larger support system with the assistance of the service providers. A central theme is recognizing the value of engaging the family in interventions for their children with disabilities. With time, the nature and focus of intervention can be expected to take the form of more personalized and more efficient ways of enhancing the functioning and development of the child with disabilities and their inclusion in family and communal life (Guralnick, 2000).
This continuing evolution of the field of early childhood intervention requires a knowledge base built on improvements in our understanding of the elements of early intervention. To optimize person-environment interactions, more specific and precise measures of the environment will need to be developed. In this context, Futterweit and Ruff (1993) have noted that it is the identification of the effective environment, not the objective environment, that is a priority for intervention efforts with young children. Further research is needed to document the developmental needs of the children and their families, the design of individualized interventions and supports, and evidence of effective interventions that can be generalized. This requires an increasing focus on the sensitivity of identification and the functional assessment of young children with disabilities. Such assessment can serve as the basis for the development of personalized interventions as well as to document the characteristics of children served in early intervention programs. In particular there is a need to improve the quality of data available to describe the population served in early childhood intervention. These are issues that are current to the implementation of early childhood intervention in Portugal and will be explored in this paper.
Early childhood intervention in Portugal
The last two decades has witnessed a significant expansion of early childhood intervention initiatives in Portugal as in other European countries. Initially these practices were not supported by specific legislative measures, but in 1999, guiding principles for early childhood intervention programs in Portugal were formalized under a joint ministerial decree (DC 891 /99) by the Education, Health, Labor and Solidarity ministries. The development of DC 891/99 was influenced by EURLYAID guidelines, representing the European Network on Early Intervention to promote common European Union policy and legislation. The EURLYAID manifesto, published in 1993, provided a comprehensive framework for member states to provide effective intervention services to young children with disabilities and their families in respective countries (De Moor, Van Waesberghe, Hosman, Jaeken, & Miedema, 1993). Early intervention continues to expand and develop as a field in the US as well as in Europe (Peterander et al., 1993).
The EURLYAID manifesto (De Moor et al, 1993) was based on the UN Convention of the Rights of the Child and inspired by the Education of the Handicapped Act Amendments of 1986 in the United States (PL 99-457). The entitlement to multidisciplinary assessment and intervention formalized in the Individualized Family Service Plan defined in PL 99-457, were also recommended by DC 891/99 for children with disabilities in Portugal.
The DC 891/99 decree emphasized the involvement of both family and community throughout the process of assessment and intervention and specified that the needed procedures should be carried out in the children's natural contexts of living. In keeping with PL 99-457, the partnership of family and professionals is recognized in the development of the Individual Intervention Plan, and is managed by a case manager responsible for full implementation of the program.
While the family centered approach was spelled out in the DC 891/99 decree, in practice, the comprehensive and integrated family-centered approach has not been fully implemented. According to a recent study of early childhood intervention in Portugal by Bairrao and Almeida (2002) many practices still reflect a restricted child-centered perspective.
It is important however to recognize the growth of initiatives in this field, represented by the establishment of new programs. The Center of Studies for the Support to the Child and Family, in Lisbon, for example, has emphasized family-centered perspectives since 1985. Another example of an inclusive and integrated early intervention program is the ecological family-centered approach of the Early Intervention Integrated Project of the District of Coimbra. This program was initiated in 1989 and has generated research on early intervention (Gomes-Pedro et al, 1995).
Publication of the DC 891/99 decree represented an important step in the development toward more ecological, comprehensive and integrated family-centered early childhood intervention programs in Portugal. This legislative measure reflected emerging policies, practices and research in early intervention in the European Union and in the United States. A central aspect of DC 891/99 important for implementation is the determination of eligibility for early intervention services. The regulations of DC 891/99 specified that early childhood intervention services were intended for children from birth until six years of age, especially for those from birth to three years of age. Two conditions define eligibility for early childhood intervention: children (a) with a disability, or (b) at risk for severe developmental delay. Determination of children eligible for early childhood intervention services under the decree is made by intervention teams operating at a council level, with child assessment carried out on the basis of eligibility criteria defined by coordination teams.
In regard to the two conditions to establish eligibility, DC 891/99 provided a description of risk factors for delay but not for children eligible on the basis of disability. Risk for severe developmental delay was defined in terms of prenatal, perinatal or postnatal factors associated with an increased probability of delay or disability in one or more areas. An additional factor constituting risk was any reason that may limit the child's capacity to benefit from intervention. However, DC 891/99 regulations did not make available specific descriptions regarding the characteristics of disability in young children. In the absence of clear and detailed descriptions for defining disability under DC 891/99, the task of defining criteria was delegated to coordination teams at the district level. Based on these criteria, intervention teams, operating at a council level, identified children likely to benefit from early childhood intervention programs.
The lack of specific criteria for eligibility introduces an important source of variability in the identification of young children being served in early childhood intervention programs in Portugal. This situation is further complicated by the fact that districts vary in the role of health, education and social sectors responsible for providing services. Further there is variability in the instruments and procedures used to determine the presence of disability or defining risk factors. The lack of specific descriptors to define disability contributes to substantial variability in terms of identification and documentation of the epidemiology of the nature and prevalence of disability in the child population in Portugal.
This imprecision in the criteria to identify children eligible for early childhood intervention services, results not only in inconsistency in describing the children served across the country, but contributes to problems of uniform description of the population and in the derivation of incidence and prevalence estimates. In summary, there is presently no uniform basis for describing the population of young children with disability in Portugal.
It is important to recognize that these issues are not specific to the field of early childhood intervention but are found in other services for individuals with disabilities. The Portuguese Superior Council of Statistics has expressed similar concerns regarding the need for promoting uniformity in the documentation of disability in two Deliberations/Resolutions, D 9/99 and D 190/99. In D 9/99, the Superior Council of Statistics proposed the adoption of a standard Portuguese classification of disability in order to achieve uniformity of concepts and terminology, as well as comparability of data nationally and internationally. This classification corresponded to a translated and condensed version of the International Classification of Impairments, Disabilities, and Handicaps (ICIDH), published in 1980 by the World Health Organization (WHO) for trial purposes. This resolution was superceded by D190/99 in light of the fact that the ICIDH was being reviewed at an international level with significant revisions made in the classification.
A commitment was made by the Superior Council of Statistics to the development of the ICIDH effort through the Working Party on Disability and Rehabilitation Statistics. With the revision of the ICIDH published by WHO in 2001 in the form of the International Classification of Functioning, Disability and Health (ICF) — and its Portuguese translation — Classificação Internacional da Funcionalidade, Incapacidade e Saúde (CIF), the Permanent Section of the Planning, Coordination and Diffusion of the Superior Council of Statistics approved the Portuguese version of the ICF for statistical use. It is expected that the translated version of the CIF will be published in the first months of 2003.
In a broader context, there is a need for a comprehensive and integrated national system to define and document the characteristics of individuals with disabilities needing support and services in Portugal. Such a system should be inclusive of children served in early childhood intervention programs and applicable to describe the characteristics of functioning and disability unique to the developing child. Specifically, it should encompass the dimensions of eligibility for early childhood intervention and be inclusive of disability and functional limitations as manifested by children in the first six years of life.
The requirement for such a classification system may be met with the International Classification of Functioning, Disability and Health by the World Health Organization - ICF (WHO, 2001). This taxonomy provides a framework of disablement including both health conditions and their consequences, as expressed in disability experience. This universal framework defines the health conditions, functioning, activities, participation and environment of an individual as a dynamic interaction of concepts. Ultimately, the ICF provides a standard language and classification to document human functioning and disability. The ICF provides a conceptual framework and an associated taxonomy with which to document the role of environmental factors on child functioning and development. The focus of the revision of the ICIDH was to develop the ICF as a classification framing disability within the dimensions of health, functioning and environmental factors. Such an approach is consistent with current conceptions of disablement as a process reflecting the ongoing interaction of the person with the environment (Verbrugge & Jette, 1994). This is in contrast to earlier classifications of disability framed within the dimensions of illness, injury and disease. In the words of WHO director Brundtland (2002), the ICD-10 (1992) provides a classification of disease and the ICF a classification of health. The value of the ICF and ICD-10 classifications are that each provides a universal language that can serve to document the needs of persons with disabilities across service systems and national boundaries.
The combined use of the ICF and the ICD-10 may be of value in addressing the need for a systematic approach to document disability and the basis for eligibility in early childhood intervention services. As two classifications in the WHO family of classifications, the ICF and the ICD-10 each can provide complementary information on the underlying etiologies, health conditions as well as the manifestation of disability and functional limitations. In that eligibility for intervention services include both diagnosed conditions of disability and risk factors for developmental delay, a classification system is needed that is inclusive of underlying conditions and environmental factors. The conditions defining eligibility can be used as a framework for using the ICF and ICD-10 classification in early childhood intervention. In the Portuguese context, two conditions for eligibility have been defined under DC 891/99; (a) presenting a disability and (b) risk of severe developmental delay. As noted earlier, in the US, a third condition is used to define eligibility, the presence of a diagnosed medical condition. On closer inspection of the risk definition under DC 891/99, risk based on biological factors may in fact overlap with the definition of established diagnosed conditions under IDEA in the US. To this end it may be useful to integrate the two Portuguese definitions with the three in the US as the basis for an organizational structure to assign codes of the ICF and ICD-10. Such an organizing framework, was developed to provide a comprehensive way to classify the reasons for eligibility of infants and toddlers served in early intervention programs in the US (Simeonsson et al., 2001).
The problems addressed were the same as those described in the situation in Portugal, namely a lack of national consistency of eligibility documentation with variability in the definitions and criteria from state to state. In that context, the three conditions were used to derive an algorithm for assignment of classification codes.
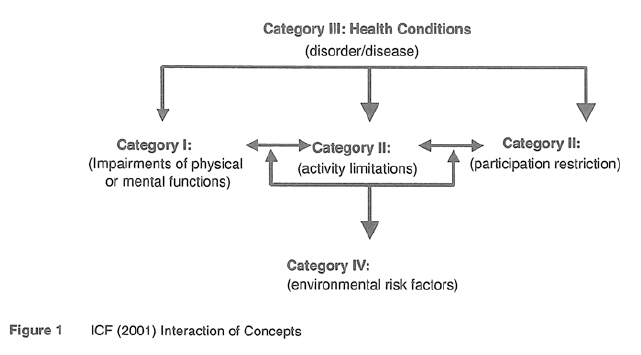
The derivation of the algorithm was based on the fact that documentation of eligibility should answer four questions regarding the developmental status of young children. These four questions were framed to encompass both dimensions of developmental delay and underlying health conditions and corresponded to the key elements of the ICF model of impairments of body functions/structure, limitations of activities/participation, environmental factors and health conditions.
1 Does the child present with significant variations in development, form or function of physical, sensory, motor, physiological, neurological or psychological systems?
2 Does the child experience limitations or delays in the performance of one or more daily life activities?
3 Is the child characterized by a specific health condition, syndrome or diagnosis associated with delayed or atypical development?
4 Are there physical, social or other environmental factors associated with risk for delayed or atypical development of the child?
In order to answer these four questions, the algorithm was set up to allow for the integration of ICF and ICD-10 codes into four major categories corresponding to the ICF model of disablement. As shown in Figure 1, the classification framework was organized around the four major categories of Health Conditions, Body Functions & Structures, Activities and Participation and Environmental Factors. To reflect a hierarchical structure, major categories were assigned Roman numerals (I-IV) and 28 subcategories were noted with capital letters (A-BB) as follows: I. Impairment of body functions or structure (A-H) II. Limitations of activity or performance (I-P). III. Health conditions (Q-X). IV. Environmental factors (Y-BB).
This classification approach has been applied in coding reasons for eligibility in US programs in the National Early Intervention Longitudinal Study- NEILS (Hebbeler et al, 2001; Scarborough et al., in press). Given the similarity of issues faced in documenting characteristics of children served in early childhood intervention programs in Portugal, the classification system has been adapted for analyzing descriptions of children provided such services. These analyses are being conducted in the context of a doctoral research project at the University of Porto (Pereira, 2003), using part of a data set collected in a national survey of early childhood intervention practices with children birth to six years of age in Portugal.
Specifically, the goal of the project was to analyze the descriptions of young children's eligibility for early childhood intervention programs in Portugal. The data for analysis were drawn from a study conducted by the Department of Basic Education of the Ministry of Education, in collaboration with the University of Porto and the Center of Studies for Support to the Child and Family of the District
Center of Solidarity and Social Affairs of Lisbon. Some of the findings of this study, which had Bairrão and Almeida as investigators, have been presented in a national meeting in Lisbon, in May, 2002 (Ministério da Educação), and in a recent publication (Bairrão & Almeida, 2002). The descriptions of the characteristics of children in early childhood intervention programs included both functional and diagnostic information. This information was gathered by special education teachers based on their own assessment taking into consideration information supplied by other providers, primarily from the health sector. As found in the analysis of the NEILS data in the US, classification of the data in Portugal was useful in documenting dimensions of health, disability and risk factors. Further, these classification studies have value in informing the current process of identifying the modification and addition of content needed to develop a version of the ICF encompassing the characteristics unique to children and youth (Simeonsson & Leonardi, 2002).
The growth of identification, assessment and intervention planning activities involving interdisciplinary teams and parents in early intervention programs around the world (Koshevinikova, 2000; Albertini & Rubino, 2000; Bjorck-Akesson, Granlund & Simeonsson, 2000) emphasize the importance of a common language of disability. In this paper, we have proposed the use of the ICF and the ICD-10 as common languages for documenting dimensions of disability in children. Beyond direct clinical applications are implications for training, policy and research. With a commitment to interdisciplinary practice with children with disabilities, it is clear that the ICF can play a key role in the training of future professionals from health, education and other disciplines. In regard to policy, the concept of "participation" in defining the lived experience of children and adults can serve as the basis for societal assurance of the rights of persons with disabilities (Lansdown, 2000). Such assurances take the form of IDEA in the US and and DC 891 /99 in Portugal and similar national laws in other countries. A central element of these laws is access to environmental support.
Given the continuing evolution of early childhood intervention, there is a need for research to develop assessment measures specific to the dimensions of activities, participation and environmental factors. The development of version of the ICF for children and youth, can provide standard language for the development of assessment measures (Simeonsson et al, 2003). Such measures are needed to track the manifestations of disability of the developing child. They may also contribute consistency in the description of children and outcomes in the current demand for evidence-based studies of effective interventions for children (Berg, 1998; Kleinman, 1998). Surveillance of childhood disability and comparative epidemiological studies have been complicated by varying definitions and the lack of correspondence with criteria for disability in adults. The standard terminology provided by the ICF can support national monitoring of demographic trends and facilitate international comparisons of the nature and prevalence of childhood disability. To that end, the studies described in this report on the utility of the ICF for classifying disability in young children can provide important information to identify modification or addition of content needed for a version of the ICF for children and youth. The availability of a such a version of the ICF can serve as an important tool to translate the promise of the UN Convention of the Rights of the Child into practical reality.
References
Albertini, G., & Rubino, S. (2000). Interdisciplinary assessment of individuals with disabilities in Italy: A new model in Rome. In M. J. Guralnick (Ed), Interdisciplinary clinical assessment of young children with disabilities. Baltimore: Paul H. Brookes, Publishing Company. [ Links ]
Bailey, D. B., McWilliam, R. A., Darkes, L. A., Hebbeler, K., Simeonsson, R. J., Spiker, D. & Wagner, M. (1998). Family outcomes in early intervention: A framework for program evaluation and efficacy research. Exceptional Children, 64 (3) 313-328. [ Links ]
Bairrão, J., & Almeida, I. C. (2002). Contributos para o estudo das práticas de intervenção precoce etn Portugal. Lisboa: Departamento de Educação Básica. [ Links ]
Berg, A. O. (1998). Dimensions of evidence. Journal of American Board of Family Practice, 11 (3) 21-6-223. [ Links ]
Bjorck-Akesson, E., Granlund, M., & Simeonsson, R. J. (2000). Assessment philosophies and practices in Sweden. In M. J. Guralnick (Ed), Interdisciplinary clinical assessment of young children with disabilities. Baltimore: Paul H. Brookes, Publishing Company. [ Links ]
Brundtland, G. H. (2002). Address to WHO meeting on the international classification of functioning, disability and health. Trieste: Italy. [ Links ] [ Links ] [ Links ]
Deliberação n.° 9/99,159.a Deliberação do Conselho Superior de Estatística. Diário da República n.° 4, de 6 de Janeiro, II série (1999).
Deliberação n.° 190/99,169.a Deliberação do Conselho Superior de Estatística. Diário da República n.° 75, de 30 de Março, II série (1999).
De Moor, J. M. H., Van Waesberghe, B. T. M., Hosman, J. B. L., Jaeken, D., & Miedema, S. (1993). Early intervention for children with developmental disabilities: Manifesto of the EURLYAID working party. International Journal of Rehabilitation Research, 16,23-31. [ Links ]
Dennis, R. E., Williams, W., Giangreco, M. R, & Collinger, C. J. (1993). Quality of life as context for planning and evaluation of services for people with disabilities. Exceptional Children, 59 (6), 499-512 [ Links ] [ Links ]
Despacho Conjunto n.° 891/99, dos Ministérios da Educação, da Saúde e do Trabalho e da Solidariedade. Diário da República n.° 244, de 19 de Outubro, II série (1999).
Futterweit, L. R., & Ruff, H. A. (1993). Principles of development: implications for early intervention. Journal of Applied Developmental Psychology, 14,153-173. [ Links ]
Gomes-Pedro, J., Patrício, M., Carvalho, A., Goldschmit, T., Torgal-Garcia, F., & Monteiro, M. B. (1995). Early intervention with Portuguese mothers: A 2-year follow-up. Journal of Developmental and Behavioral Pediatrics, 16 (1), 21-28. [ Links ]
Guralnick, M. J. (Ed.) (2000). Interdisciplinary clinical assessment of young children with disabilities. Baltimore: Paul H. Brookes, Publishing Company. [ Links ]
Hebeler, K. M., Wagner, M., Spiker, D., Scarborough, A., Simeonson, R., & Collier, M. (2001). A first look at the characteristics of children and families entering early intervention. Menlo Park, CA: SRI International. [ Links ]
Kozhevinikova, E. (2000). Interdisciplinary assessment within early intervention in Russia. In M. J. Guralnick (Ed.), Interdisciplinary clinical assessment of young children with disabilities (pp. 367-386). Baltimore: Paul H. Brookes, Publishing Company. [ Links ]
Lansdown, G. (2000). Implementing children's rights and health. Archives of Diseases of Children, 83,286-288. [ Links ]
Kleinman, L. C. (1998). Prevention and primary care research for children: the need for evidence to precede "evidence-based". American Journal of Preventive Medicine, 14 (4), 345-351. [ Links ]
Ministério da Educação (2002, May). Pensar a intervenção precoce em Portugal: Encontro nacional. Lisboa: Departamento de Educação Básica. [ Links ]
Organização Mundial de Saúde (1989). Classificação internacional das deficiências, incapacidades e desvantagens (handicaps): Um manual de classificação das consequências das doenças. [ Links ] [Transl, from International classification of impairments, disabilities, and handicaps: A manual of classification relating to the consequences of disease (Geneva, 1980)]. Lisboa: Secretariado Nacional de Reabilitação.
Pereira, S. R. (2003). Classification of dimensions of disability in early childhood intervention programs in Portugal. Dissertação de doutoramento não publicada. Porto: Faculdade de Psicologia e de Ciências da Educação da Universidade do Porto.
Peterander, E, Opp, G., & Speck, O. (1993). Analyzing structure and content of early intervention in Bavaria, Germany: Implications for the education of young children with special needs. Special Issue: Risk and resilience in individuals with learning disabilities: an international focus on intervention approaches and research. Learning Disabilities Research & Practice. 8 (1) 52-58. [ Links ]
Simeonsson, R. J. & McDevitt, L. (1999). Issues in disability and health: The role of secondary conditions and quality of life. Chapel Hill, NC: FPG Child Development Center, University of North Carolina.
Simeonsson, R. J., & Leonardi, M. (2002, October). Adapting the ICF for child health systems: Status report. [ Links ] Meeting of Heads of WHO Collaborating Centers for the Classification of Diseases. Brisbane: World Health Organization.
Simeonsson, R. J., Leonardi, M., Bjorck-Akesson, E., Hollenweger, J., Lollar, D. J., Brown, S. C. & ICY task force (in press). International Classification of Functioning, Disability and Health: Toward a universal classification of disability in childhood. Social Science & Medicine. [ Links ]
Scarborough, A. A., Spiker, D., Mallik, S., Hebbeler, K., Bailey, D. B., & Simeonson, R. J. (in press). A national picture of children and families entering early intervention. Exceptional children. [ Links ]
Verbrugge, L . M., & Jette, A. M. (1994). The disablement process. Social Science & Medicine, 38,1-14. [ Links ]
World Health Organization (1980). International classification of impairments, disabilities, and handicaps: A manual of classification relating to the consequences of disease. Geneva: World Health Organization (reprinted in 1993 with foreword). [ Links ]
World Health Organization (2001). International Classification of Functioning, Disability and Health. Geneva: WHO. [ Links ]


{kind=link}