











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkINTRODUCTION
The worldwide outbreak known as COVID-19, caused by the Severe Acute Respiratory Syndrome - CoronaVirus 2 (SARS-CoV-2), triggered a significant public health concern. In March 2020, the Director-General of the World Health Organization (WHO) declared COVID-19 a pandemic due to the high transmissibility and lethality of the disease (WHO, 2020).
Despite the social and physical distancing measures aimed at decelerating the disease's spread, WHO advocated the preparation of health facilities and health professionals to cope with the increasing number of COVID-19 patients. Health care workers (HCWs) are in the front line of the outbreak response, dealing with patients (with COVID-19 or other diseases) and their families, and therefore facing a considerably increased risk of becoming infected with COVID-19 (Bielicki et al., 2020).
Thus, the purpose of this study was to understand how HCWs' concern about contracting COVID-19 affected their emotions and consequently impacted their burnout levels. To sustain our hypotheses, we have drawn on one conservation of resources theory underlying mechanism, i.e., energy depletion (Hobfoll et al., 2018). In our study, the energy depletion mechanism may be crucial to explain the effort and resources spent by HCWs during this high-stress situation and its impacts on affectivity and burnout.
A sample of Portuguese HCWs was chosen due to the high-pitched number of patients of COVID-19 that the country registered, which demanded extra efforts from the Portuguese health care system. According to the Portuguese Directorate-General of Health and the Portuguese Ministry of Health, until the end of June 2020, the country registered 42,523 confirmed cases of COVID-19, from which a total of 1,579 deaths and 27,798 recovered cases were registered (Direção-Geral da Saúde, 2020). Adding to this, HCWs comprised a significant proportion of the people who contracted the disease. Indeed, according to recent reports, in Portugal, until the 24th of July, 8.25% of the infected were healthcare professionals (Jornal Médico, 2020).
The COVID-19 pandemic, like other pandemics that have affected the world (e.g., Ebola), has demanded additional efforts from HCWs that, unlike other professionals, were required to continue working to assist all the infected. By doing so, these professionals were much more susceptible to have contact with the COVID-19, putting their health at risk for everyone else's. Hewlett and Hewlett (2005) suggested that this constant exposure to risk may increase HCWs' levels of fear and insecurity about being infected.
In this highly stressful pandemic context, our results have significant contributions. Specifically, findings inform HCWs, health care managers, and organizations about the harmful effects of risk concern on negative affect and burnout.
THEORETICAL BACKGROUND
The impact of burnout in the healthcare context
As defined by Kristensen et al. (2005, p. 197), work-related burnout is the "degree of physical and psychological fatigue and exhaustion that the person perceives as related to his/her work." Burnout has been widely studied amongst HCWs and carries significant consequences to workers (e.g., Munyon et al., 2009), the organization (e.g., Leiter & Maslach, 2009), and patients (e.g., Dewa et al., 2017). Ehrlich et al. (2020) highlight the susceptibility of HCWs in the context of COVID-19, which is in line with Jalili et al. (2020) and Barello et al. (2020) findings on burnout prevalence among HCWs during this period.
Occupational stress, a well-established antecedent of burnout, is often experienced by HCWs and might have been intensified during the pandemic (Sultana et al., 2020). COVID-19 is responsible for an important psychological impact in this population, where anxiety and stress can be aggravated. This can be explained by the still hidden and uncontrollable nature of this disease, where there is still limited knowledge but a significant health impact (Jalili et al., 2020).
Risk concern as a predictor of burnout
As mentioned before, risk concern is expected to be related to enhanced strain among HCWs during this pandemic (Sultana et al., 2020). We draw upon the conservation of resources (COR) framework (Hobfoll et al., 2018). This framework outlines how individuals in their personal and professional lives endeavor to attain, assemble, and protect valued resources (e.g., health and well-being) to avoid strain. Employees may experience strain when their available resources are scarce, i.e., because they are threatened or lost, making them incapable of coping effectively with demands, especially in contexts where these are highly imposed (Hobfoll et al., 2018).
The use of this theoretical framework to explain our rationale is justified by several reasons. First, Portugal has recently overcome a severe economic crisis, and it is known that employees from countries that experience this kind of crisis tend to develop higher levels of burnout and negative affect due to the persistent perception of losing important resources, such as their jobs or work stability (Ferreira et al., 2019). Second, the loss and gain of resources are central in high-stress situations, where demands tend to increase (Alarcon, 2011). Thus, the dramatic increase in labor requirements imposed by the COVID-19 pandemic and the heightened risk perceptions associated with it may have potentiated resource losses (e.g., health and well-being). In this study, we conceptualize the risk concern of contracting COVID-19 as a stressor that may increase burnout levels. Thus, we propose that:
Hypothesis 1. Risk concern is positively related to burnout.
The mediation role of affect
Risk perception comprises two components: cognitive and affective (Sjöberg, 1998). The former is related to the individual's perceived likelihood of experiencing a dangerous event, and the latter refers to how much they worry about it (Rundmo, 2000). The emotional component holds a critical role due to the level of uncertainty caused by the COVID-19 pandemic. Accordingly, Freeston et al. (2020) describe that this pandemic may contribute to uncertainty distress, "the subjective negative emotions experienced in response to the as yet unknown aspects of a given situation" (p. 1). This is in line with Son et al. (2019) work that describes emotional arousal as a consequence of risk appraisal.
Affective states hold a positive and negative nature. Positive affect expresses enthusiasm, activeness, and alertness, while negative affect expresses subjective distress (Galinha et al., 2014). Both negative and positive affect are associated with subjective health (Benyamini et al., 2000). Moreover, Little et al. (2007) findings show that negative affect is positively associated with burnout, while positive affect is negatively associated with it, which was also found in a study with HCWs (Montero-Marin et al., 2015).
From what has been described, burnout can be conceived as a product of work demands and a lack of resources (Munyon et al., 2009). Therefore, the COR theory (Hobfoll et al., 2018) may illustrate this process. Accordingly, risk concern overloads HCWs, contributing to the loss of mental resources - expressed by low levels of positive affect and high levels of negative affect - and burnout. Therefore, we posit that:
Hypothesis 2. Positive affect mediates the positive relationship between risk concern and burnout.
Hypothesis 3: Negative affect mediates the positive relationship between risk concern and burnout.
The moderator role of risk exposure
As mentioned, risk concern may increase burnout, and emotions play an essential role in this process (e.g., Montero-Marin et al., 2015). However, these effects may vary depending on the level of exposure to the risk. As humans, we are provided with mechanisms that prevent us from harmful and dangerous situations. Neuberg et al. (2011) proposed two threat-management systems (self-protection and disease avoidance) that activate affective, cognitive, and behavioral responses. Broadly, these mechanisms will operate to decrease risk, which, in most cases, means that once a threat is perceived, it will be avoided. Some findings are in line with this framework, showing how risk perception may decrease the level of risk exposure (Stewart-Taylor & Cherrie, 1998).
HCWs are frontline players in this pandemic, which may increase their levels of risk concern (Hewlett & Hewlett, 2005). However, withdrawing from their job is not a solution. Moreover, depending on the specific position, some HCWs are highly exposed to risk, regardless of concern levels. We argue that not being able to behave according to risk appraisal may provide additional strain and excessive resource consumption, resulting in higher burnout levels. Specifically, we propose that:
Hypothesis 4. The level of risk exposure will moderate all of the hypothesized relationships such that the effects will be stronger for individuals who report high levels of exposure (vs. low levels).
METHOD
Procedure and Participants
Data were collected through an online questionnaire during May and June of 2020, disseminated through the research team's networks. Informed consent was presented to participants at the beginning of the questionnaire.
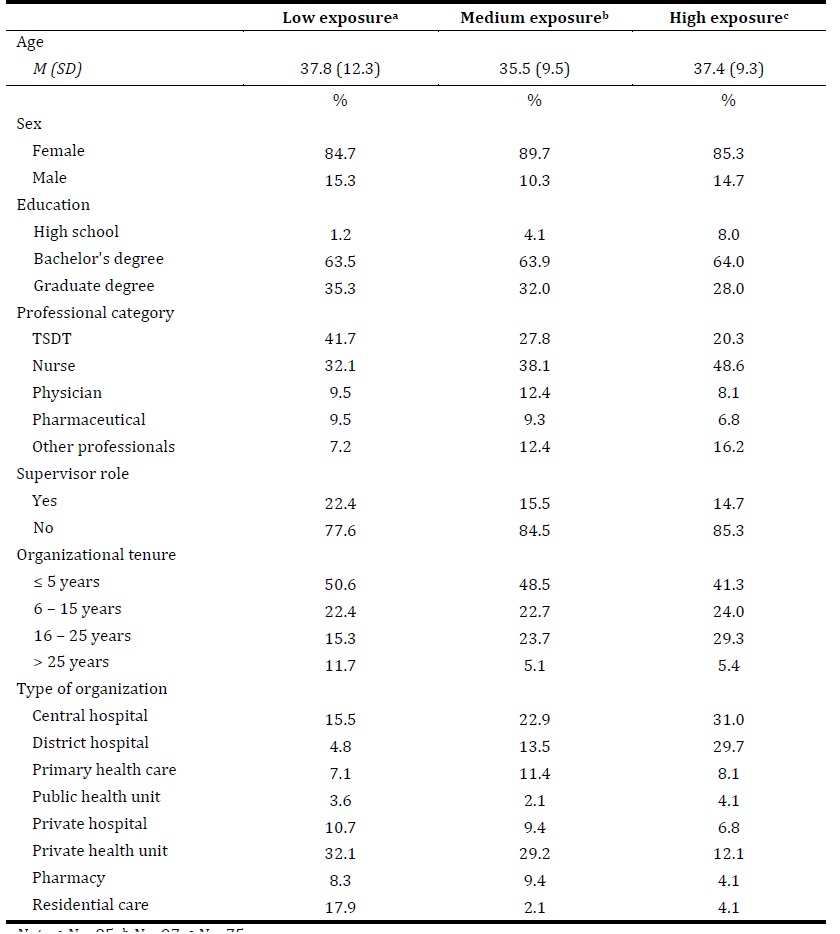
The sample consists of 257 HCWs, aged between 21 and 65 (M = 36.80, SD = 10.47). Most participants were female (86.8%), completed a bachelor's degree (63.8%), and about 70% worked in the organization for 15 years or less. Among the participants, 39.2% were nurses, 30.2% were senior diagnostic and therapeutic technicians (TSDTs), and 25.2% worked in a private health unit. Individuals were categorized into three groups according to their perceived level of exposure to COVID-19: low, medium, and high exposure. Table 1 presents the participants' characteristics by level of exposure.
Measures
All participants were fluent in Portuguese, which required the translation/back-translation procedure (Brislin, 1970; van de Vijver & Hambleton, 1996). The first stage involved translating the items from the source language (i.e., English) to the target language (i.e., Portuguese). Then a blind back-translation was performed by an independent researcher. This version was compared to the original version and reviewed by a bilingual researcher who suggested small modifications. Given that the positive and negative affect scale was already adapted and validated for Portugal (Galinha et al., 2014), it was not included in the translation process.
Risk perception. Risk perception questions were adapted from Sridhar et al. (2016) and include risk exposure and risk concern. Participants were asked to indicate their perceived level of exposure to COVID-19 on a scale from 1 - no contact to 7 - full-time contact (i.e., "Does your work involve direct contact with patients with COVID-19?"). Risk concern was measured through one question: "To what extent are you concerned that you might contract COVID-19?", answered on a scale from 1 - not at all to 7 - very much concerned.
Positive and negative affect. Positive and negative affect were assessed through the short version of PANAS (PANAS-VRP) (Galinha et al., 2014). Participants answered 10 items about how often they had experienced a specific emotion since the beginning of the pandemic situation on a scale from 1 (not at all) to 5 (extremely). The positive affect subscale included five items (e.g., enthusiastic, active), and the negative affect subscale encompassed five items (e.g., nervous, scared). Both subscales showed very good internal consistency (α = .85 for each dimension).
Burnout. Burnout was assessed using the 7-item Copenhagen Burnout Inventory (Kristensen et al., 2005). Participants answered on a 5-point scale ranging from 1 - never/almost never to 5 - always. A sample item is "Is your work emotionally exhausting?". The scale revealed excellent internal reliability (α = .90).
Controls. Age (in years) was used as a control variable since previous literature found that it is associated with burnout (e.g., Munyon et al., 2009). Also, supervisors' support was identified as a predictor of burnout among HCWs (e.g., Pisanti et al., 2011), and therefore it was controlled in this study.
Measurement model and common method bias
A Confirmatory Factor Analysis (CFA) for the total sample was conducted in AMOS v. 25. The measurement model showed a good fit to the data, χ 2 (111) = 217.62, p < .001, χ 2 / df = 1.961, CFI = .96, TLI = .95, RMSEA = .06, SRMR = .07 (Hair et al., 2010). As shown in Table 2, this three-factor measurement model yielded a better fit than all the alternative models.
Reliability, convergent, and discriminant validity of the measurement model were assessed and are summarized in Table 3. All constructs showed high internal consistency as Cronbach's alphas ranged between .85 and .90, and composite reliability (CR) indices exceeded .70 (Hair et al., 2010). In addition, the average variance extracted (AVE) values were equal to or above the threshold value of .50 (Hair et al., 2010). Therefore, the latent variables meet the requirements of convergent validity.
Table 2 Fit indices for measurement model comparisons
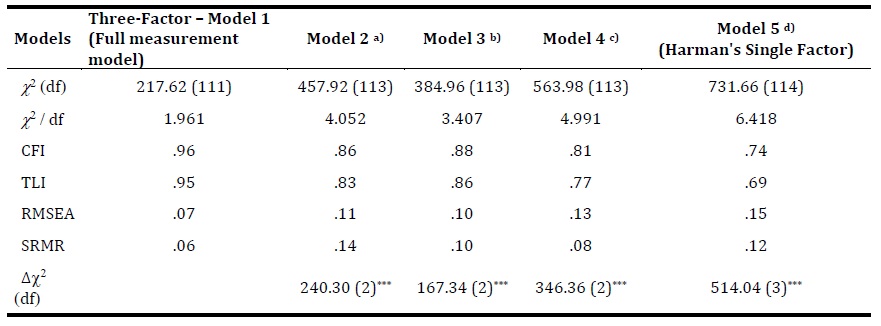
Note. N = 257; χ2 - chi-square; df - degrees of freedom; χ2/df - normed chi-square; CFI - comparative fit index; TLI - Tucker-Lewis index; RMSEA - root mean square error of approximation; SRMR - standardized root mean square residual; Δ2 - chi-square difference.
a) Positive affect and Negative affect combined into a single factor.
b) Positive affect and Burnout combined into a single factor.
c) Negative affect and Burnout combined into a single factor.
d) The three factors combined into a single factor.
*** p < .00
As shown in Table 3, the AVE of each construct's square root is greater than the inter-construct correlations, which fulfilled the Fornell-Larcker criterion (Fornell & Larcker, 1981). The AVE values were also greater than the maximum shared variance (MSV) (Hair et al., 2010). Moreover, the heterotrait-monotrait (HTMT) ratio of correlations values ranged between .35 and .68, below the threshold of .85 (Henseler et al., 2015). Thus, discriminant validity is reached in this study.

Harman's single-factor test was conducted to address common method variance concerns (Podsakoff et al., 2003). As shown in Table 2, a single-factor model showed a poor fit to the data.
Finally, to detect multicollinearity, tolerance and variance inflation factor (VIF) values were calculated using SPSS v. 26. Tolerance values ranged between .69 and .92 (>.10), whereas the VIF values ranged from 1.09 to 1.45 (<5), suggesting that there are no multicollinearity problems in the model (Hair et al., 2010).
Measurement invariance
A multi-group confirmatory factor analysis (MCFA) was then used to assess the configural, metric and scalar invariance of the three groups: low, medium, and high exposure to COVID-19 (Vandenberg & Lance, 2000). The measurement model reached a good fit, χ 2 (333) = 458.83, p < .001, χ 2 / df = 1.378, CFI = .95, TLI = .93, RMSEA = .04, SRMR = .09. Thus, configural invariance was established.
Full metric invariance was assessed by comparing the unconstrained model (i.e., free estimates) with the constrained model (i.e., factor loadings constrained to be equal across groups). Results indicate that there is full metric invariance (Δχ 2 (28) = 28.98, p > .05). Finally, scalar invariance was tested by maintaining the metric invariance model's restrictions and constraining observed variables' intercepts on their latent factor. This model shows scalar invariance (Δχ 2 (62) = 65.23, p > .05). These findings establish measurement invariance, justifying the examination of differences across levels of risk exposure.
RESULTS
The descriptive statistics of variables in the study are presented in Table 4. For the three levels of exposure, the strongest correlations were found between negative affect and risk concern (r low = .44, p < .001; r med = .53, p < .001; r high = .48, p < .001), and negative affect and burnout (r low = .57, p < .001; r med = .67, p < .001; r high = .43, p < .001).
Table 4 Descriptive statistics of variables in the study
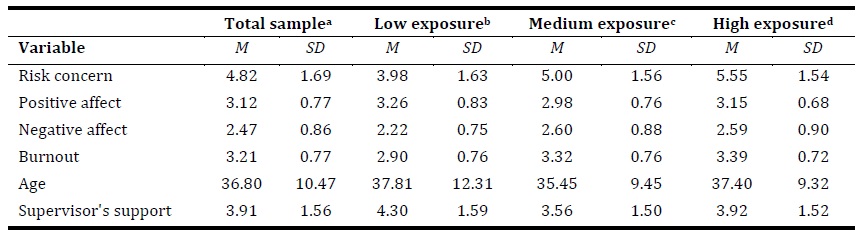
Note. a N = 257; b N=85;c N = 97; d N = 75.
Structural model
A three-group structural equation modeling (SEM) was conducted in AMOS to investigate if the level of risk exposure impacted the proposed model. The structural model showed an acceptable fit, χ 2 (468) = 707.70, p < .001, χ 2 / df = 1.512, CFI = .91, TLI = .88, RMSEA = .05, SRMR = .10. Results are illustrated in Table 5. Hypothesis 1 stated that risk concern would positively correlate with burnout, which was supported by the findings.
Table 5 Multi-group SEM results for total sample and low, medium, and high levels of risk exposure
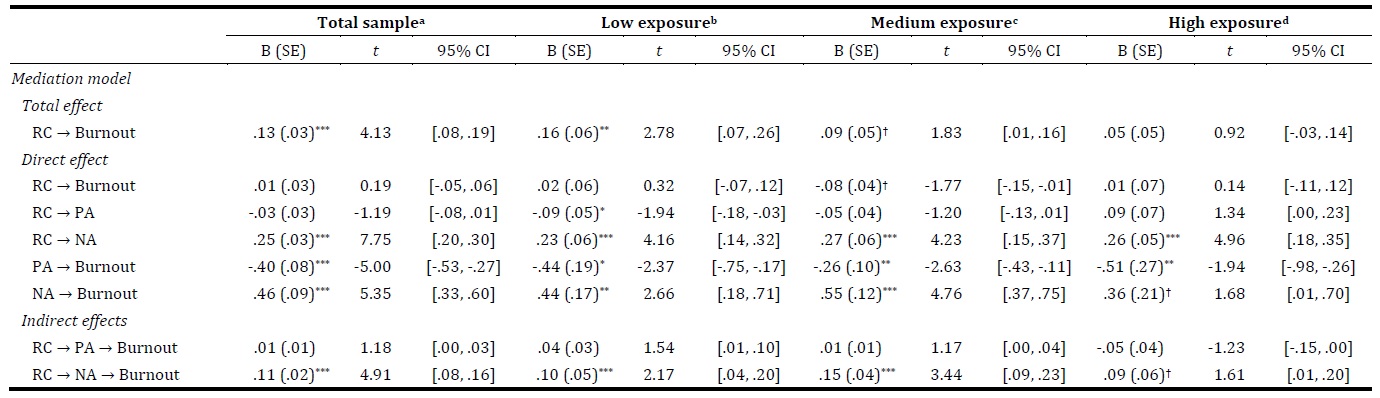
Note. a N = 257; b N = 85; c N = 97; d N = 75. Unstandardized coefficients are reported. All estimates were tested for significance using bias-corrected (BC) confidence interval from 5,000 bootstrap samples.
RC = risk concern; PA = positive affect; NA = negative affect
†p< .10 * p < .05 ** p < .01 *** p < .001
The second hypothesis, proposing that positive affect would mediate the relationship between risk concern and burnout, was not supported. Hypothesis 3 claimed that negative affect would mediate the relationship between risk concern and burnout. The findings support this hypothesis, as shown in Table 5.
Finally, the fourth hypothesis proposed that previously hypothesized relationships would be moderated by the level of risk exposure, such that the effects would be stronger for individuals who perceive high risk. A pairwise parameter comparison was conducted to compare the magnitude of coefficients from the multi-group analysis. Contrary to our expectations, there were no significant differences between low and high-risk groups in the risk concern-burnout relationship (z = -.173, p > .05). Also, the indirect effect of risk concern on burnout via negative affect was not statistically different for these two groups (z = -.332, p > .05). Thus, hypothesis 4 was not supported.
DISCUSSION
This study investigated the impact of risk concern on burnout of HCWs during the COVID-19 pandemic and the mediation of positive and negative affect in this relationship. Further, this paper examined the moderation role of risk exposure in this parallel mediation model.
Hypotheses 1 and 3 were supported by the findings, consistent with previous literature on burnout (e.g., Little et al., 2007; Montero-Marin et al., 2015). These findings are of critical importance once they offer both theoretical and practical contributions. They are especially important since a second wave of COVID-19 constitutes a looming threat to health care systems (Leung et al., 2020). First, our study shows that a critical contextual stressor (i.e., risk concern) increases burnout levels among HCWs in the specific context of COVID-19 (H1). This is critical because HCWs are pivotal players in fighting the pandemic. Thus, it is not overstated to claim that HCWs' well-being may have an essential and systemic impact in society, making clear the urgency to implement strategies designed to decrease risk concern and its effect on burnout. The SARS-CoV-2 virus spreads through close contact (WHO, 2020). Therefore, we argue that risk concern can be reduced if one can use protective barriers, particularly in HCWs work settings where it is impossible to ensure physical distancing. An example of a highly valued strategy is personal protective equipment delivery and training (Carvalho et al., 2019; Wang et al., 2020).
Second, results regarding the mediation of negative affect (H3) provide empirical evidence to expand the COR theory (Hobfoll et al., 2018). Accordingly, within the pandemic context (i.e., high demanding context), HCWs' risk concern (that creates an overloaded mental state) produces negative affect (i.e., loss of resources), giving rise to burnout. Again, these results suggest that organizations should implement an integrated strategy to buffer the negative potential of risk concern on negative affect and burnout. Within this specific context, HCWs cannot decide to skip work to avoid the source of stress, and for this reason, they need to learn how to face and manage this contextual threat. Therefore, this study aims to draw organizations' attention to the relevance of considering emotion regulation and stress management training programs (e.g., Hersch et al., 2016).
Hypothesis 2 was not verified as risk concern did not influence positive affect, which means that individuals do not experience fewer positive emotions despite being concerned with becoming infected with COVID-19. The lack of support for this hypothesis can be explained by the buffering role of other work-related factors, such as the existence of a safety climate (i.e., safety policies, procedures, practices, and behaviors in the workplace), and personal factors (e.g., social support outside work) (e.g., McCaughey et al., 2013).
Hypothesis 4 was not supported as both direct and indirect (via negative affect) effects were not stronger for the high-risk group. These results can have two main explanations. First, when perceiving risky situations, workers may engage in problem-solving adaptive strategies such as wearing protective equipment (Arezes & Miguel, 2005), which may impact their vulnerability to experience burnout. Second, higher levels of risk exposure may produce habituation (Barnett & Breakwell, 2001), which may explain why those reporting higher risk exposure levels do not report more burnout due to risk concern.
In conclusion, our findings disclose the reality of HCWs in a pandemic context. Despite its contributions to understanding how COVID-19 impacts HCWs' well-being, our study is not without limitations. First, this was a cross-sectional study using self-reported measures. Also, we point to our sample size as a limitation. Hence, future research should use longitudinal designs and broader samples to enhance study findings' generalization. Second, the convenience sample of this study was collected through a snowball approach. However, we have applied this sampling method due to the population's specificities (i.e., health care sector) we intended to study (Babbie, 2014).

