










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkPsicologia, Saúde & Doenças
versão impressa ISSN 1645-0086
Psic., Saúde & Doenças v.11 n.2 Lisboa 2010
Parental concerns about their children's health and development:suggestions for the reorganization of well-child care
Ana Rita Goes1, Maria Cortes1,2, & Luísa Barros1
1Faculdade de Psicologia, Lisboa, Portugal.
2Alto Comissariado da Saúde, Lisboa, Portugal.
Contactar para Email: anarita.goes@gmail.com
Abstract
Developmental and behavioural disorders affect 12 to 16% of children. There are effective interventions to promote the wellbeing of both children and their families to reduce negative outcomes. The provision of appropriate developmental and behavioural services must be guided by family needs. Parental concerns are a reliable tool to evaluate children’s developmental and behavioural status and to make decisions regarding these services. This study explored parents’ concerns in a Portuguese health care setting. We used an interview, focusing on concerns about parenting and the child’s physical health, development, behaviour and interaction. When questioned in a systematic and standardized way, parents discussed concerns about their children’s development and behaviour, as well as the parental role. All parents had at least one concern about their child. Most parents expressed concerns about their child’s behaviour, particularly about discipline. We discuss implications for the provision of developmental and behavioural services within well-child care.
Keywords: Developmental and behavioural problems; parental concerns; well-child care.
Preocupações parentais sobre a saúde e o desenvolvimento: sugestões para a reorganização dos cuidados de saúde pediátricos
Resumo
As perturbações de desenvolvimento e comportamento afectam 12 a 16% das crianças. Existem intervenções efectivas para promover o bem-estar das crianças e famílias e para reduzir o impacte negativo dessas perturbações. Os serviços orientados para responder aos problemas de desenvolvimento e comportamento das crianças devem ter em conta as necessidades das famílias. As preocupações parentais são um instrumento fiável para avaliar o desenvolvimento e comportamento das crianças e para tomar decisões sobre estes serviços. Este estudo explorou as preocupações parentais em consulta de cuidados primários. Utilizámos uma entrevista sobre as preocupações relacionadas com o papel parental, saúde física, desenvolvimento e comportamento dos filhos. Quando questionados de forma sistemática, os pais discutiram preocupações sobre desenvolvimento, comportamento e papel parental. Todos tinham pelo menos uma preocupação com o filho. A maioria dos pais expressou preocupações sobre o comportamento da criança, particularmente sobre disciplina. São discutidas implicações para a prestação de serviços direccionados para o desenvolvimento e comportamento no contexto da vigilância de saúde infantil.
Palavra-chave: Problemas de desenvolvimento e comportamento; preocupações parentais; vigilância de saúde infantil
Over the last decades, scientific progress has lead to the achievement of unprecedented child health indicators. Children’s physical health is better today than it has ever been. However, there is a rising prevalence of the so-called “new morbidities” such as obesity, as well as behavioural and developmental disorders (Kelleher, McInerny, Gardner, Childs, & Wasserman, 2000). According to international estimates, 12 to 16% of children have developmental or behavioural disorders (e.g. Boyle, Decoufle, & Yeargin-Allsoop, 1994).
Research suggests that the period from conception to age six is the most influential in the life cycle of brain development and this period is equally influential in subsequent learning, behaviour and health (McCain & Mustard, 1999). The quality of early experiences, namely parent-child relationships, has a strong impact on brain development and has long-term effects on the person’s wellbeing (Shonkoff & Phillips, 2000; Richter, 2004).
The rising incidence of developmental and behavioural problems among children attests to the inability of some children and their families to cope appropriately with the increasing stresses in their lives, resulting in their need for assistance (American Academy of Pediatrics [AAP], 2003). International surveys indicate that many parents feel unprepared and unsupported in their parental role and that they acknowledge the need for advice about raising their children (Desforges & Abouchaard, 2003; Young, Davis, Schoen, & Parker, 1998). Several interventions to improve child development and adjustment have been proved to be effective (e.g. Minkowitz et al, 2007; Olds, 2007; Puura et al., 2002) and to achieve better outcomes for children and their families (e.g. Barnett, 1995; Boocock, 1995). Therefore, providing services to families that support the healthy development of children can reduce the prevalence of developmental and behavioural disorders.
Professionals in Primary Care have substantial and continued contact with parents during childhood and parents expect them to provide information on child development and parenting, as well as on the physical aspects of health (Young et al., 1998; Schuster, Duan, Regalado, & Klein, 2000; Bethell, Peck, & Schor, 2001). There is also evidence that parents do adhere to the childrearing recommendations they receive from healthcare providers, thus improving children’s and families’ outcomes (e.g. Black & Teti, 1997; Sege et al., 1997; Needlman, Toker, Dreyer, Klass, Mendelsohn, & 2005). Well-child care constitutes an important opportunity to provide developmental and behavioural services and several organizations call for an integration of behavioural and developmental issues during well-child care visits (e.g. American Academy of Pediatrics, Bright Futures).
Contemporary protocols and guidelines for child health surveillance in primary care invariably call for attention to child development and behaviour as well as to a variety of psychosocial and family factors that may require assessment and intervention (e.g. Committee on Practice and Ambulatory Medicine and Bright Futures Steering Committee, 2007; Hagan, Shaw & Duncan, 2008;). The use of a comprehensive approach to development that includes developmental surveillance, developmental/behavioural screening, education/counseling, intervention and care coordination, is widely recommended. Portuguese guidelines on well-child care share these recommendations, and encourage health professionals to survey and respond to parents’ concerns, to assess child development, to prevent socio-emotional disorders, to identify and provide interventions for developmental and behavioural problems and to provide anticipatory guidance about developmental tasks and problems (Direcção-Geral da Saúde, 2005).
In spite of existing practice guidelines to support well-child care in order to ensure the optimal health and development of young children, the provision of appropriate developmental and behavioural services is limited by a whole set of barriers. These include lack of care standards, unrealistic expectations about the content of well-child care, time constraints, inadequate training and insufficient community-based resources to address families’ needs (Regalado & Halfon, 2001; Schor, 2004; Yarnall, Pollack, Ostbye, Krause, Michener, 2003). Therefore, the use of well-child care for promoting child development and adjustment lags behind expectations. International studies show that fewer than 30% of children with developmental or behavioural problems are identified by their primary health care provider (Glascoe & Shapiro, 1999), thus limiting the acknowledged benefits of early intervention. International surveys also found that most parents reported unmet needs for parenting guidance, education or screening by primary health care providers and that almost half the parents reported not being asked about their concerns regarding the child’s learning, development or behaviour (Bethell et al., 2001; Bethell, Reuland, Halfon, & Schor, 2004; Schuster et al., 2000; Young et al., 1998).
Efforts and recommendations to improve developmental and behavioural services have two major goals: improving identification of developmental and behavioural problems and improving education, counseling and intervention within health care services constraints. In order to achieve this, an important role is attributed to the identification of parental concerns.
The identification of developmental and behavioural problems often relies on health professionals’ clinical judgment derived from observation, reviewing milestones and the administration of age appropriate tasks selected from developmental schedules and milestone checklists (Centre for Community Child Health, Royal Children’s Hospital Melbourne, 2002). However, a significant proportion of children with problems remain not identified.
Some researchers emphasize that clinical judgment is influenced by the way in which health professionals elicit, recognize and select clinical information and use appropriate judgments (Glascoe & Dworkin, 1993, 1995). Research showed that obtaining parental inputs increases the accuracy of clinical impressions and that certain clusters of parental concerns relate directly to children’s performances on screening tests for developmental and behavioural problems (Dulcan et al., 1990; Glascoe & Dworkin, 1995). For example, 72% of parents whose children failed a screening test on speech-language were concerned about this area of development; while 83% of parents whose children passed the same screening test were not concerned (Glascoe, 1991). In another study, 70% of children who failed a standardized measure of behavioural and emotional problems had parents with concerns about their behavioural and emotional status (Glascoe, MacLean & Stone, 1991). Therefore, professionals can use parental concerns to identify the risk for developmental and behavioural problems (Glascoe, 1991, 1994, 1997a, 1998).
This area of research also indicates that care should be taken in order to elicit and categorize parental concerns appropriately. Parents are more likely to share their concerns when they are worried about expressive language or health problems and some parents do not spontaneously discuss their concerns. (Glascoe, 1997b). This may indicate that parents do not always recognize that a more complete discussion about developmental or behavioural concerns is relevant to primary health care professionals. They may not realize that interventions to minimize these problems are possible.
It has been shown that parents are able to provide highly accurate indicators of childhood behavioural and developmental problems in response to structured and systematic questioning regarding their concerns, i.e., when the professional prompts them to specifically think about different developmental and behavioural domains (Glascoe, Altemeier, & MacLean, 1989).
The importance of parental concerns goes far beyond the identification and appropriate referral of children with developmental and behavioural problems. Research shows that approximately 30% of parents worry about their children, even though their children are developing and behaving within the broad range of normality (Glascoe, 1997). Part of those parents may be noticing subclinical or subtle manifestations of a problem, as children of these parents tend to have lower scores on socialization, speech-language and motor skills or exhibit a larger number of behavioural problems (Glascoe, MacLean & Stone, 1991; Glascoe, 1997). Other parents may be experiencing particular difficulties in managing normal behaviour. Explanations for other cases may include parents’ anxiety or inaccurate expectations about children’s development and behaviour. Whatever the case, parental concerns when children are developing and behaving normally also indicate that there is a need for further evaluation or clinical guidance by the health care professional. Using these concerns as a “teachable moment”1 (“ Teachable moments are effective opportunities to facilitate some sort of change and to address parents' issues, initiate discussions of common behavioural and developmental concerns and approach sensitive topics such as maternal depression or domestic violence “ (Zuckerman & Parker, 1997) for parents’ education and counseling is probably adequate in these situations (Glascoe & Dworkin, 1995). Parents appear to respond best to information focused on their specific areas of concern. Teachable moments related to these specific concerns have been identified as an effective way to provide education and counseling to parents and, therefore, to promote optimal development within the time constraints of health care settings (Glascoe, Oberklaid, Dworkin & Trimm, 1998; Bethell et al., 2004; Schor, 2004; Zuckerman, Stevens, Inkelas, & Halfon, 2004). Furthermore, it should be noted that parental concerns seem to be highly specific and very useful in guiding the health professional’s selection of different interventions (Glascoe, 1999c).
Despite the recognized importance of parental concerns for child health surveillance and the existence of Portuguese guidelines that explicitly recommend that health professionals evaluate these concerns, they have received little consideration in the Portuguese literature on child health surveillance and care. The present study intends to explore and describe the health and educational concerns of parents of children aged 2 to 6 years in a Primary Health Care setting. We aimed to answer the following research questions:
What kind of concerns do Portuguese parents of children aged 2 to 6 years have within the broad dimensions of a child’s physical health, development, behaviour, and social interaction, as well as parenting?
What is the frequency of concerns for the different domains?
How likely are Portuguese parents to engage in discussions relating to developmental and behavioural concerns when probed in a health care setting?
This work is part of a larger study on the role of Portuguese well-child care for promoting child development and adjustment. Data discussed in this paper is being used to guide the development of a program for promoting child development and adjustment through well-child care in Primary Health Care settings.
METHODS
Participants
The study was conducted in three Primary Health Care Centers from the same geographical area within the surroundings of Lisbon. Participants were parents (or other primary caregivers, such as grandparents, sisters) of children aged 2 to 6 years. They were recruited while waiting for child health appointments, using convenience sampling with the following inclusion criteria: to speak Portuguese fluently, to accept participation according to the informed consent protocol and to receive continuous well-child care at these health units. There were no exclusion criteria for children. Two families refused to participate because of time constraints or their need to pay close attention to their children at that particular time. Three parents that had agreed to participate were excluded as they were not fluent in Portuguese or lacked enough information about the child. 57 families participated. Most respondents were mothers (82.5%) and some interviews were made with both parents present (14%).
In terms of socio-demographic characteristics, the average age was 34.5 years for mothers and 32.6 for fathers. Parents’ educational levels ranged from no schooling to professional degrees. Most fathers completed nine (33.3%) or less (21.1%) years of education and most mothers completed twelve (38.6%) or less (45.6%) years of education. Most parents were married (49.1%) or lived in marital unions (35.1%).
Children had an average age of 3.68 years, 52.6% were girls, and half the children were first born. More than half attended childcare facilities (59.6%). Two children had special education needs and four children had special health needs, as reported by parents.
Most parents and children were at the health care facility for routine well-child care (70.2%) while 17.5% were there for acute care visits and 12.3% for other motives, such as immunizations.
Measures
Given the exploratory nature of this study, we chose a qualitative method using a semi-structured interview to evaluate parental concerns. This methodology allowed us to evaluate parents’ understanding of the questions and the eventual need to reformulate them, as well as their reactions to the specific questions. At the same time, the semi-structured interview allowed the researcher to further explore and clarify parents’ answers, allowing a better understanding of the meanings of their assertions and verbalizations. Contrary to what is done in most studies of parental concerns that use questionnaires including items specific for each developmental domain , such as fine motor, gross motor, receptive language, expressive language, autonomy (Glascoe, 2002), we conducted a semi-structured interview using open questions for broader dimensions. All answers were recorded.
The interview started with a broad question on parents’ concerns: “Please tell me any concerns you have about the way your child is behaving, learning and developing”. The remaining interview guide was organized into five major dimensions: physical health, development, behaviour, social interaction, and parenting. For each of these dimensions, parents were asked: “Do you have any concerns about your child’s physical health? …how is your child learning and developing? …how does your child behave? …how does your child get along with others? …and do you have any concerns about parenting?” The interview also included an open-ended question eliciting any other concerns that parents had not mentioned before. For each dimension, additional probing questions were included to guide parents with the type of concerns that could be included (e.g. for the physical health domain: “Do you have any concerns about your child sleeping and feeding?”). The development of the interview guide took into consideration recommendations concerning the wording and the structure of the questions from previous literature (Glascoe et al., 1989).
A demographic questionnaire about child and family characteristics was administered, in order to characterize the participants. In addition, parents were asked about their subjective evaluation of their child’s overall health status, using a subjective scale with three anchor points (excellent, good, and poor).
Procedures
Parents (or their substitutes) were interviewed while waiting for scheduled child health appointments. The first author informed parents about the study, invited them to participate and obtained informed consent. She also conducted all the interviews.
Parents’ verbalizations were transcribed and the content was analyzed and classified according to different broad dimensions (health, development, behaviour, parenting). Answers to the first general question were allocated into the appropriate specific dimension to receive further analysis. In the answers to the following questions, if parents mentioned concerns from different dimensions (for instance, if parents mentioned behavioural and health issues when answering the question about development) the concerns were allocated to each appropriate dimension. Categories were generated using an inductive approach. Within each dimension, answers were organized in categories based on common themes (for example, within the behavioural dimension we identified categories on discipline and anxiety). For each category, a definition was developed. Afterwards, we revisited the original data for newly emerging themes or categories and added them as necessary. Coding was then checked by two additional researchers to ensure that categories were derived from data and not imposed by personal beliefs or prejudices. These codes were analyzed statistically for the identification of frequencies of different concerns.
RESULTS
Parents’ subjective evaluation of their children’s health status
Almost all parents perceived their children’s health status as good (n=33; 57.9%) or excellent (n=23; 40.4%).
Parents’ concerns
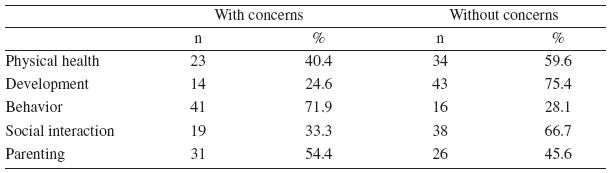
All parents had at least one concern in one of the domains approached (table 1). The majority of concerns reported were in the domains of behaviour (71.9%) and parenting (54.4%). For each domain, parents were able to raise one or more concerns. Table 1
Table 1
Parents’ concerns by major domains
Pascal Health
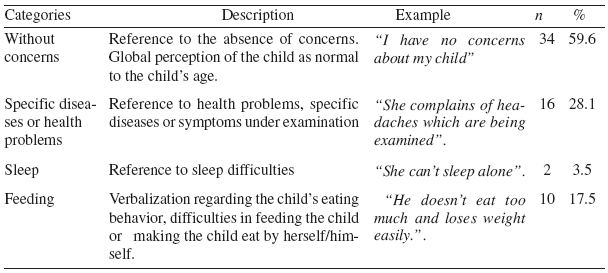
The domain of physical health included any concerns relating to child health, feeding or sleeping. Approximately 40% of parents reported concerns about their child’s physical health. Most of them were concerned about specific disease or health problems or feeding (table 2).
Table 2
Parents’ concerns about physical health
Development
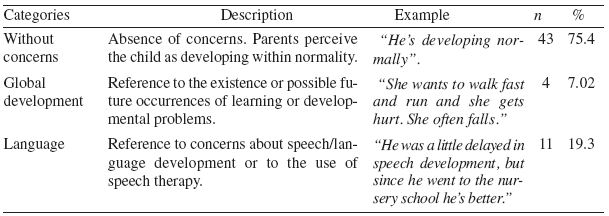
We included in the domain of development any verbalizations relating to the child’s overall developmental status or to motor, cognitive, and language development. Most parents did not report concerns about development (75.4%). Among those who reported developmental concerns, most had concerns about expressive language (table 3).
Table 3
Parents’ concerns about development
Behaviour
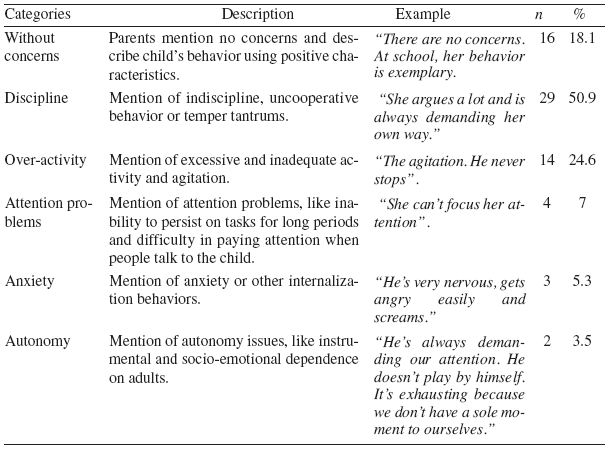
In the domain of behaviour, were included any concerns relating to the child’s overall behaviour pattern or about behavioural problems, such as discipline, attention, overactivity, anxiety, and autonomy. Forty-one parents reported one or more concerns about behaviour. Approximately 50% of parents reported concerns about discipline, and fourteen parents mentioned concerns with the over activity of the child (Table 4).
Table 4
Parents’ concerns about behavior
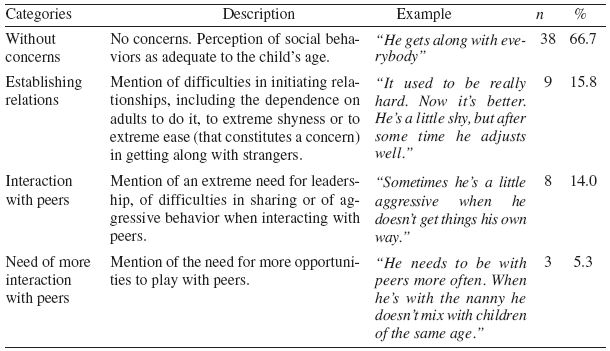
Social Interaction
Parents’ concerns about the child’s overall pattern of interaction or about specific abilities or behaviors that interfere with the establishment and maintenance of social interactions were included in the domain of social interaction. Most parents reported no concerns in this domain. Twenty parents (35.1%) reported one or more concerns about the child’s ability to establish social relations, problems during peer interactions and the need for more interaction with peers (table 5).
Table 5
Parents’ concerns about social interaction
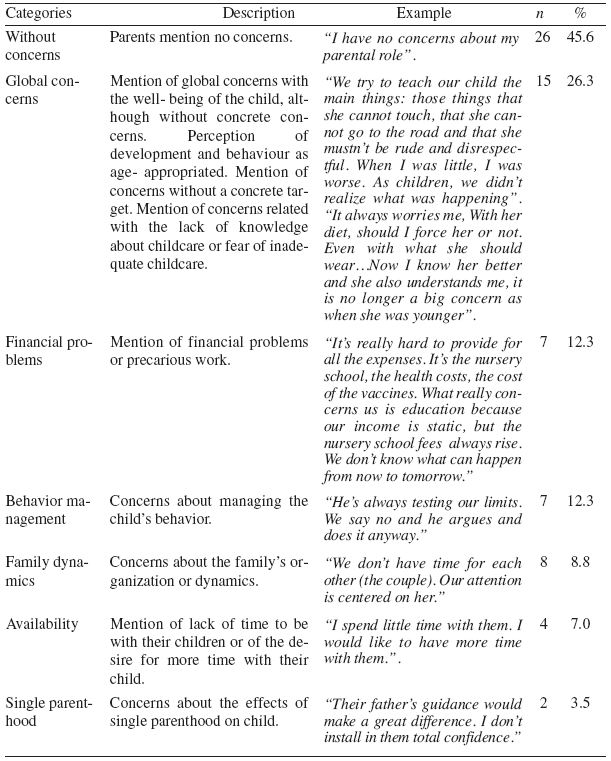
Parenting
The domain of parenting included parents’ concerns about their overall experience of parenting or about their perceived parental ability, as well as any constraints relating to their competencies in the parental role. Approximately half the parents reported one or more concerns within this domain, with a large heterogeneity of themes (table 6). Fifteen parents (26.3%) reported global and diffuse concerns around the hard job of raising a child and the major demands and efforts for providing appropriate care, protection and nurturance to the child. Concerns that were more specific included financial constraints, child behaviour management, family dynamics, family structure, and family time.
Table 6
Parents’ concerns about parenting
DISCUSSION
When interviewed, Portuguese parents discussed concerns about their child’s development and behaviour as well as their parental role, confirming the pattern of responses already identified in international studies (Reijjneved, Meer, Wiefferjnck, & Crone, 2008; Ford, Sayal, Meltser, & Goodman, 2005). As in the USA and Australia, concerns about the development and behaviour of young children and about their own parenting role are prevalent amongst Portuguese parents.
In this study, a significant number of parents had no concerns across the majority of the domains explored and only mentioned singular areas of concern. In a study conducted by Glascoe (2002), 43% of parents either did not think about or worried about their child’s behaviour and development. Among these parents with no concerns about their child’s development, only 5% had children with developmental problems. In our study, the absence of multiple concerns may also indicate the absence of real behavioural and developmental problems.
With regard to global themes, parental concerns were similar to those found in classical parental studies (Glascoe, 1999a, 1999b; Kanoy & Schroeder, 1993). The prevalence of parental concerns within each domain also follows the major trends documented in the literature (Hickson, 1983 cit in Glascoe, 2002; Glascoe & Dworkin, 1995; Glascoe, 1999b; Glascoe, 2000; Reijjneved et al, 2008).
Most parents did not report concerns related to their child’s physical health, including sleeping and feeding. The fact that most parents evaluated positively their child’s overall health status and that appointments were mainly well-child consultations may partially explain these findings. In addition, the belief that mild physical health concerns would be satisfyingly addressed during the visit, thus not constituting a relevant concern, may had some effect on there results. Previous studies have found that parents report fewer concerns about physical health in healthcare settings than when interviewed in other contexts and that, in the absence of a specific disease, other themes deserve more parental attention (Glascoe, 1999a, 1999b, 1999c; Glascoe, 2003; Reijjneved et al. 2008).
Only a few parents expressed concerns about their child’s development, mostly about expressive language. Language concerns are the developmental issues most likely to be raised by parents. Parental concerns about speech-language development are also strong predictors of developmental problems (Glascoe et al., 1989; Glascoe, 1991, 1997, 2003; Tervo, 2005). Therefore, children whose parents raised concerns about expressive language in this study are likely to have a developmental problem, which will need further assessment and probable intervention (Glascoe, 2002, 2003, 2005). Additionally, some parents may express their worries about their child’s development through the verbalization of concerns related to behavioural problems (Oberklaid, Dworkin, & Levine, 1979; Glascoe, 1994). Though, the prevalence of children from this study in risk for a developmental problem may be higher, once their parents may be expressing their child’s developmental difficulties through behavioural concerns. This is another reason to pay close attention to different dimensions of parental concerns.
Most parents expressed concerns about their child’s behaviour. Previous studies confirm a prevalence of concerns related to behavioural issues (Reijjneved et al., 2008; Glascoe, 1999a). Behavioural concerns are good predictors of possible future problems in this area. For example, 87% of children with attention-deficit hyperactivity disorder had parents with concerns about impulsiveness, attention problems or over activity (Glascoe, 1999b, 2002; Mulhern, Dworkin, & Bernstein, 1993). In our study, some parents did mention concerns about their child’s over activity and short attention span. Many behaviors, which are difficult to deal with, and raise conflicts over discipline or routines, are frequent during toddlerhood and preschool years. Several studies show that parent reported social-emotional and behavioural problems are common (Gross, Sambrook, & Fogg, 1999). Parent-reported behavioural problems have been associated with higher behaviour intensity (i.e., more disturbing behaviors), greater parental stress, lower self-efficacy, and poor discipline strategies characterized by irritability, coercion, and inconsistency (Gross et al., 1999). Therefore, even if most of the children in this study seem to be functioning well, some of these parents and children may be engaged in highly stressful and coercive relationships and these parents may find an intervention to be beneficial.
In this study, the majority of parents that discussed behavioural concerns mentioned specifically problems about discipline. Hickson (1983 cit in Glascoe, 2002) also found that an important percentage of parents expressed concerns related to discipline. Although we could not find any data about the predictive value of these concerns, the high prevalence of parental concerns about discipline found in this study highlight the needs of these families in this area. Moreover, this is consistent with international guidelines about the need to provide anticipatory guidance on this topic and the call for action to this specific domain (e.g. Canadian Paediatric Society, 2004).
Most parents did not report concerns about social interaction. Those parents who did so, mentioned problems in establishing relationships and in peer interactions. According to Glascoe (2003), parental concerns about behaviour and social skills are strong predictors of mental health problems in children. Therefore, parents reporting concerns about social interaction should receive careful attention from well-child care providers. On the contrary, parents without concerns in this area have a high probability of having children with no social problems (Glascoe, 2002).
Parents reported a diverse set of concerns about parenting issues. These results confirm previous research showing that, at some point, all parents will have concerns about their children and their own parental role and will need to discuss them with people outside the family context (Reijjneved et al., 2008; Glascoe). For some, parenting represents a major challenge, and they feel insecure and unsupported (Barros & Santos, 2006; Glascoe, 1999a, 1999b; Glascoe, 2002; Glascoe 2003; Moran, Ghate, & Merwe, 2004). Providing support and imparting skills to parents constitutes an important opportunity for the promotion of child development and adjustment (Barros & Santos, 2006; Silva, Eira, Vicente, & Guerreiro, 2003).
Through this study, we were able to describe parental concerns within a sample of Portuguese parents in a well-child care setting. Parents openly discussed concerns about their child and about their own parental roles, easily expressed their main concerns and needs and valued the interview as an important task.
Research shows that parents often do not discuss their behavioural concerns with the healthcare providers. Parents may not share their concerns unless asked or when questions are not systematic and well structured (Glascoe, 1997b). This raises the question of whether Portuguese parents concerns about their children and their parental role are usually discussed during regular well-child care visits. Studies show that about one third of parents do not spontaneously discuss their concerns and that parents who do so are more likely to discuss their concerns if they are worried about health or expressive language issues, and less likely if they are worried about behavioural issues (Glascoe, 1997b). It is clear that health care providers cannot depend on parents to initiate discussions relating to their concerns. International research shows that most health professionals do not evaluate parental concerns systematically (Bethell et al., 2004), and even when parents’ concerns are discussed, health professionals may not use the information collected to identify family needs and provide appropriate services (Sices, Feudtner, McLaughlin, Drotar, & Williams, 2004). In addition, parents may worry about their children, even though they are developing and behaving within the normal range (Glascoe, 1997). These parents may need some form of support that, in the absence of disclosure, is not recognized or dealt with.
These findings may constitute the foundation for important suggestions and contributions to well-child care reorganization. However, several limitations must be considered. We used a small convenience sample, which makes it impossible to generalize our findings to the overall population, even though the sample used allowed for the collection of descriptive information until saturation of data. Another limitation of this study is the absence of validation data for parental concerns, as we did not assessed child development nor had any other sources of information about child behaviour. These issues should be considered in future studies.
Well-child care has been repeatedly recognized as an opportunity for the promotion of child development and adjustment. National and international guidelines for professional practice recognize the role of well-child care in primary care and make strong recommendations for the provision of integrated developmental and behavioural services, such as developmental assessment and anticipatory guidance. However, developmental and behavioural services face time constraints and several studies have shown that parents have unmet needs in this area. Recommendations for improving developmental and behavioural services in well-child care call for a strong investment in the identification and valuing of parental concerns.
The current study confirmed international research showing that eliciting parental concerns may provide well-child care providers with an opportunity to detect possible developmental and behavioural problems, as well as to promote a family-centered approach to parenting (Glascoe et al., 1998). According to the international research, parents desire more information and support to help their children grow and develop in healthy ways (Young et al., 1998). Knowledge of Portuguese parental concerns and awareness of their relevance may guide the identification of the kinds of services and materials that need to be made available to such families.
To ensure an effective approach to behaviour and development, health professionals need not only to elicit parental concerns systematically, but also to have appropriate answers for the concerns raised. Results show that parents had concerns about development, behaviour and social interaction, pointing the need to consider approaches to these areas during well-child care visits. Particularly, most parents had concerns on the behaviour dimension and especially about discipline issues, which focus the need to develop specific educational/counseling efforts to this area. The availability of effective parental counseling about behaviour and discipline during routine primary care would be possible through the development of partnerships between primary health care professionals and mental health professionals.
Primary care professionals have regular contact with families and could provide these interventions, while mental health professionals could support the development of interventions and its implementation through training and supervision. Psychologists may play an important role as consultants to primary healthcare providers, both in promoting the systematical assessment of parental needs and helping professional to interpret these concerns, but also in supporting the development and use of educational materials and information in a language and format appropriate to these parents.
REFERENCES
American Academy of Pediatrics. (2003). Family pediatrics: report of the Task Force on the Family. Pediatrics, 111(6), 15411571.
Barnett, S. W. (1995). Long-term effects of early childhood programs on cognitive and school outcomes. The Future of Children, 5(3), 2550.
Barros, L., & Santos, M. (2006). Significações sobre parentalidade e bons Cuidados: como pensam os pais? In: M.C. Taborda, M.T. Sousa Machado, M.L. Vale Dias & L. Nobre Lima (Eds.), Psicologia do desenvolvimento: temas de investigação. Coimbra: Almedina.
Bethell, C., Peck, C., & Schor, E. (2001). Assessing health system provision of well-child care: the Promoting Healthy Development Survey. Pediatrics, 107, 10841094.
Bethell, C., Reuland, C. P., Halfon, N., & Schor, E. L. (2004). Measuring the quality of preventive and developmental services for young children: national estimates and patterns of clinicians’ performance. Pediatrics, 113, 19731983.
Black, M. M., & Teti, L. O. (1997). Promoting mealtime communication between adolescent mothers and their infants through videotape. Pediatrics, 99(3), 432437.
Boocock, S. S. (1995). Early childhood programs in other nations: goals and outcomes. The Future of Children, 5(3), 94114.
Boyle, C. A., Decoufle, P., & Yeargin -Allsoop, M. (1994). Prevalence and health impact of developmental disabilities in US children. Pediatrics, 93(3), 399403.
Canadian Paediatric Society. (2004). Effective discipline for children – position statement (pp200401). Paediatric Child Health. 9(1) 3741.
Centre for Community Child Health, Royal Children’s Hospital Melbourne. (2002). Child health screening and surveillance: a critical-review o fthe evidence. Australia: National Health and Medical Research Council.
Committee on Practice and Ambulatory Medicine and Bright Futures Steering Committee. (2007). Policy statement: Recommendations for Preventive Pediatric Health Care. Pediatrics, 120(6), 1376.
Desforges, C., & Abouchaar, A. (2003). The impact of parental involvement, parental support and family education on pupil-achievement and adjustment: a literature review. London: Department for Education and Skills.
Direcção-Geral da Saúde (2005). Saúde Infantil e Juvenil: Programa tipo de Actuação–Orientações Técnicas. Lisboa: Direcção-Geral da Saúde.
Dulcan M. K., Costello, E. J., Costello, A. J., Edelbrock, C., Brent, D., & Janiszweski, S. (1990). The pediatrician as gatekeeper to mental health care for children: do parents’ concerns open the gate? Journal of the American Academy of Child and Adolescent Psychiatry, 29(3), 453458.
Ellingson, K. D., Briggs-Gowan, M. J., Carter, A. S. & Horwitz, S. M. (2004), Parent identification of early emerging child behaviour problems. Archives of Pediatrics & Adolescent Medicine, 158, 766772.
Ford, T., Sayal, K., Meltser, H. & Goodman, R. (2005). Parental concerns about their child’s emotions and behaviour and referral to specialist services: general populations’ survey. British Medical Joural, 331, 14351436.
Glascoe, F. P. (1991). Can clinical judgment detect children with speech-language problems? Pediatrics, 87(3), 317322.
Glascoe, F. P., & Dworkin, P. H. (1993). Obstacles to effective developmental surveillance: errors in clinical reasoning. Journal of Developmental and Behavioural Pediatrics, 14(5), 344349.
Glascoe, F. P. (1994). It’s not what it seems. The relationship between parents’ concers and children with global delays. Clinical Pediatrics, 33(5), 292296.
Glascoe, F. P. (1997a). Parents´ concerns about children’s development: pres-creening technique or screening test? Pediatrics, 99 (4), 522528.
Glascoe, F. P. (1997b). The importance of discussing parents’ concerns about development: do parents express concerns spontaneously? Ambulatory Child Health, 2, 349356.
Glascoe, F. P. (1999a). Using parents´ concerns to detect and address developmental and behavioural problems. Journal of the Society of Pediatric Nursing, 4(1), 2435.
Glascoe, F. P. (1999b). The value of parents concerns to detect and address developmental and behavioural problems. Journal of Paediatrics and Child Health, 35, 18.
Glascoe, F. P. (1999c). A method for deciding how to respond to parents´ concerns about developmental and behaviour. Ambulatory Child Health, 5, 197208.
Glascoe, F. P. (2000). Evidenced-based approach to developmental and behavioural surveillance using parent’s concerns. Child: Care, Health and Development, 26(2), 137149.
Glascoe, F.P. (2002). Collaborating with parents: using parents’ evaluation of developmental status to detect and address developmental and behavioural problems. Nashville, TN: Ellsworth & Vandermeer Press.
Glascoe, F. P. (2003). Parents´ Evaluation of Developmental Status: How well do parents´ concerns identify children with behavioural and emotional problems? Clinical Pediatrics, 42(2), 133138.
Glascoe, F. P. (2005). Screening for developmental and behavioural problems. Mental Retardation and Developmental Disabilities Research Review, 11, 173179.
Glascoe F. P. Altemeier W. A. & MacLean W. E. (1989). The importance of parents’ concerns about their child’s development. American Journal of Diseases of Children. 143 (8): 955958.
Glascoe, F. P., & Dworkin, P. H. (1993). Obstacles to effective developmental surveillance: errors in clinical reasoning. Journal of Developmental and Behavioural Pediatrics, 14(5), 344349.
Glascoe, F. P., & Dworkin, P. H. (1995). The role of parents in the detection of developmental and behavioural problems. Pediatrics, 95(6), 829.836.
Glascoe, F. P., MacLean, W. E., & Stone, W. L. (1991). The importance of parents’ concerns about their child’s behaviour. Clinical Pediatrics, 30(1), 811.
Glascoe, F. P., Oberklaid, F., Dworkin, P. H., & Trimm, F. (1998). Brief approaches to educating patients and parents in Primary Care. Pediatrics, 101(6), e10.
Glascoe, F. P., & Shapiro, H. L. (1999). Introduction to developmental and behavioural screening. Developmental and Behavioural Pediatrics Online. Available from: www.dbpeds.org/articles/detail.cfm?TextID=%205. Accessed 2010 Jan 13.
Gross, D., Sambrook, A., & Fogg, L. (1999). Behaviour problems among young children in low-income urban day-centers. Research in Nursing & Health, 22(1), 1525.
Hagan, J. F., Shaw, J. S., & Duncan, P. M. (Eds.). (2008). Bright Futures: guidelines for health supervision of infants, children and adolescents. 3rd Ed. Elk Grove Village: American Academy of Pediatrics.
Kanoy, K. W., & Schroeder, C. S. (1993). Suggestion to parents about common behaviour problems in a pediatric primary health care office. Five years of follow-up. In M. Roberts, G. Roocher, & D. Routh, Readings in Pediatric Psychology (pp. 317332). New York: Plenum.
Kelleher, K. J., McInerny, T. K., Gardner, W. P., Childs, G. E., & Wasserman, R. C. (2000). Increasing identification of psychosocial problems: 19791996. Pediatrics, 105(6), 13131321.
McCain, M. N., & Mustard, J. F. (1999). Early years study: reversing the real-brain drain. Ontario: Publications Ontario.
Minkowitz, C. S., Strobino, D., Mistry, K. B., Scharfstein, D. O., Grason, H., Hou, W., Ialongo, N, & Guyer, B. (2007). Healthy Steps for Young Children: sustained results at 5.5 years. Pediatrics, 120(3), e658e668.
Moran, P., Ghate, D., & Merwe A., (2004). What works in parenting support? A review of the international evidence. United Kingdom: Department of Education and Skills.
Mulhern, S., Dworkin, P. H., & Bernstein, B. (1993). Do parental concerns predict a diagnosis of attention-deficit hyperactivity disorder? Journal of Developmental and Behavioral Pediatrics, 15(5), 349352.
Needlman, R., Toker, K. H., Dreyer, B. P., Klass, P., & Mendelsohn, A. L. (2005). Effectiveness of a primary care intervention to support reading aloud: a multicenter evaluation. Ambulatory Pediatrics, 5(4), 209215.
Oberklaid, F., Dworkin, P. H., & Levine, M. D. (1979). Developmental behavioural dysfunction in preschool children. Descriptive analysis of a pediatric consultative model. American Journal of Diseases of Children, 133(11), 11261131.
Olds, D. L., Sadler, L., & Kitzman, H. (2007). Programs for parents of infants and toddlers: recent evidence from randomized trials. Journal of Child Psychology and Psychiatricy, 43(3/4), 355391.
Puura, K., Davis, H., Papadopoulou, K., Tsiantis, J., Ispanovic-Radojkovic, V., Rudic, N., Tamminen, T., Turunen, M., Dragonas, T., Paradisiotou, A., Vizakou, S., Roberts, R., Cox, A., & Day, C. (2002). The European Early Promotion Project: a new Primary Health Care service to promote children’s mental health. Infant Mental Health Journal, 23(6), 606624.
Regalado, M., & Halfon, N. (2001). Primary care services promoting optimal child development from birth to age three years. Archives of Pediatric and Adolescent Medicine, 155(12), 13111322.
Reijjneved, S., Meer, G., Wiefferinck, C. H., & Crone, M. R., (2008). Parent´s concerns about children are highly prevalent but often not confirmed by child doctor and nurses. BMC Public Health, 8, 124
Richter, L. (2004). The importance of care giver child interactions for the survival and healthy development of young children: a review. Geneva: World Health organization, Department of Child and Adolescent Health and Development.
Schor, E. L. (2004). Rethinking well child care. Pediatrics, 114(1), 210216.
Shuster, M., Duan, N., Regalado, M., & Klein, D. (2000). Anticipatory guidance: what information do parents receive? What information do they want? Archives of Pediatric and Adolescent Medicine, 154(12) 11911198.
Sege, R. D., Perry, C., Stigol, L., Cohen, L., Griffith, J., Cohn, M., & Spivak, H. (1997). Short-term effectiveness of anticipatory guidance to reduce early childhood risks for subsequent violence. Archives of Pediatric and Adolescent Medicine, 151(4), 392397.
Shonkoff, J. P., & Phillips, D. A.. (2000). From neurons to neighborhoods: the science of early-childhood development. Washington D C: National Academies Press.
Schuster, M. A., Duan, N., Regalado, M., & Klein, D. (2000). Anticipatory guidance: what information do parents receive? What information do they want? Archives of Pediatric and Adolescent Medicine. 154, 11911198.
Sices, L., Feudtner, C., McLaughlin, J., Drotar, D., & Williams, M. (2004). How do primary care physicians manage children with possible developmental delays? A national survey with an experimental design. Pediatrics, 113(2), 274282.
Silva, P. C., Eira, C., Vicente, M. G., & Guerreiro, R. (2003). Promoção do desenvolvimento psicossocial das crianças através de serviços de Cuidados de Saúde Primários. Análise Psicológica, 1(XXI), 5976. [ Links ]
Tervo, R. C. (2005). Parent´s reports predict their child´s developmental problems. Clinical Pediatrics, 44, 601611.
Yarnall, K. S., Pollak, K. I., Ostbye, T., Krause, K. M., & Michener, J. L. (2003). Primary care: is there enough time for prevention? American Journal of Public Health, 93, 635641.
Young, K. T., Davis, K., Schoen, C., & Parker, S. (1998). Listening to parents: a national survey of parents with young children. Archives of Pediatric and Adolescent Medicine, 152, 255262.
Zuckerman, B., Parker, S. (1997). Teachable moments: assessment as intervention. Contemporary Pediatrics, 14(), 103118).
Zuckerman, B., Stevens, G. D., Inkelas, M., & Halfon, N. (2004). Prevalence and correlates of high quality basic pediatric preventive care. Pediatrics, 114(6), 15221529.
Acknowledgements We thank staff and parents from the participating well-child care facilities for their contributions to the study. The present study is part of a larger project supported by a doctoral grant from the Portuguese Science and Technology Foundation.
Recebido em 9 de Junho de 2010/ Aceite em 29 Novembro de 2010
