











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkSevere acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes coronavirus disease 2019 (COVID-19), is currently threatening the world (WHO, 2020a). A SARS-CoV-2 outbreak was confirmed in Portugal in March 2020. On 12 March 2020, the day the World Health Organization (WHO) declared COVID-19 a pandemic (WHO, 2020b), the Portuguese government declared the highest level of alert, resulting in extraordinary public health and infection control measures. Under this state of emergency, airports were closed, civil transportation halted, national borders markedly controlled and individuals' movements greatly restricted. All Portuguese were strongly advised to maintain social distance and received non-mandatory recommendations to stay at home. The state of emergency remained until 2 May, at which point Portugal started easing restrictions (https://covid19.min-saude.pt). Data from a company that developed a mobile app to analyse the mobility of Portuguese citizens reveals that the stay-at-home rate was 29.35% on 12 March, peaked on 12 April at 79.21%, and then gradually decreased. On 2 May, the rate was 59.1%. As expected, rates of confinement are higher on weekends (https://www.pse.pt).
Although lockdown recommendations help control pandemics (Jarvis et al., 2020), they impose life changes that challenge people's mental health (Torales et al., 2020). Psychological reactions to pandemics are diverse and complex. Whereas some individuals are resilient to stress, others become highly distressed, particularly when confronted with threats such as potentially serious viral infections. Some people react with indifference or resignation while others become highly fearful or anxious. Factors such as separation from loved ones, loss of freedom, uncertainty over disease status, and boredom can generate psychological effects and occasionally even psychopathologic symptoms such as depressive mood, anxiety, irritability, anger, fear and insomnia (Ozamiz-Etxebarria et al., 2020; Yahya et al., 2020). Some individuals recover from these emotional problems once the pandemic threat passes, while others' reactions endure (Brooks et al., 2020a; Reynolds et al., 2008; Taylor, 2019).
Aiming to measure the effects of quarantine on mental health and psychological wellbeing, a recent review compiled studies conducted across ten countries that included people in areas affected with SARS, Ebola, the 2009 and 2010 H1N1 influenza, Middle East respiratory syndrome and equine influenza. The authors determined the most important stressors to be a lengthy quarantine, the fear of becoming infected or transmitting the virus to others, boredom, frustration, a sense of being isolated from the rest of the world, a lack of basic supplies and insufficient or unclear guidelines about actions to take during the quarantine. Finances and stigma were determined to be important post-quarantine stressors. Generally, the review suggests that the psychological impact of quarantine is wide-ranging, substantial, and potentially long-lasting (Brooks et al., 2020b). However, these findings should be generalised to the current pandemic with caution since most of the included studies used small samples with short quarantine times.
Research also suggests that specific groups may be more vulnerable than others to the burden of pandemics (Brooks et al., 2020b; Hao et al., 2020; Mazza et al., 2020; Wang et al., 2020). Although few studies investigate this topic, previous pandemics seem to impact the genders differently with a predominantly negative impact on the female gender (Smith, 2019; Wenham et al., 2020). Some researchers have focused on studying stigma, critical sociodemographic features and specific professions such as healthcare workers, finding, for instance, that health care staff may experience both self and social stigma (Brooks et al., 2020b; Li et al., 2020; Maunder et al., 2003; Ornell et al., 2020; Xiang et al., 2020).
Although several studies address the mental health costs of mandatory quarantine (Brooks et al., 2020b), less is known about the immediate impact of mass lockdowns on the emotional, behavioural and occupational status of individuals. For instance, despite the negative psychological effects, which the media focus on (Depoux et al., 2020b), might there be gains? Do people benefit from significantly increasing their time spent at home?
Several external factors also influence people's emotional reactions to pandemics. News broadcasts sometimes exaggerate the risk and lethality of infections by using emotionally tinged language. Social media, which enable virtual content creation and continual information sharing among users, have a propensity to spread false beliefs, rumours and misinformation (Larson, 2018; Taylor, 2019; Yammine, 2020). Such factors seem to fuel fear (Depoux et al., 2020a) and further modulate public emotional responses (Blendon et al., 2004). Previous outbreaks have shown that negative public reactions may contribute to undesirable outcomes, such as unnecessary or overwhelming demand for healthcare services or excessive precautionary behaviour, with resulting negative effects on the community and its economy (Blendon et al., 2004; Demidov, 2002; Rosling & Rosling, 2003). In a recent large online survey in Germany, with a total of 12,244 respondents during the shutdown in March 2020, Teufel et al. (2020) concluded that subjects overestimated risk compared to existing COVID-19 incidence rates.
Since verified information can effectively prevent panic (Lancet, 2020), objective measures of how the Portuguese people are feeling and coping with self-isolation due to the COVID-19 pandemic are crucial to provide reliable information on the psychological impact of lockdown in our population. Therefore, this study aims to explore the immediate emotional and occupational impact of the COVID-19 pandemic as well as any resulting changes in key health-related behaviours during the first four weeks of self-isolation.
Method
Participants
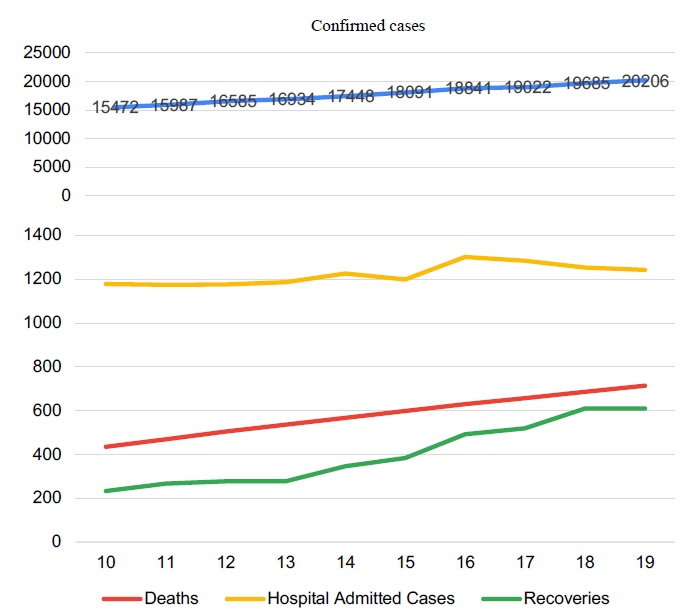
The sample collection started on 10.04.2020 and ended on 19.04.2020. We intended to capture the study information in a delimited period of roughly 1 month of lockdown so that we could assure some political and social stability and avoid other potentially psychological influences, such as mental fatigue due to social isolation. To apprehend the situation of the country during the period of data collection, we present the numbers in figure 1.
From an initial sample of 1819 respondents, 25 were removed for being under the age of 18 or for incorrect completion of the survey. Thus, 1794 cases were considered for the final sample.
All individuals included in the study participated voluntarily and gave informed consent. The study was approved by the Ethics Committee of the Centro Hospitalar Lisboa Norte (CHLN) and the Academic Medical Center of Lisbon (CAML) on April 21, 2020 (Ref. No. 167/20).
Material
The data collection process relies on a web-based survey, which was self-administered.
Taking into account the massive amount of information that individuals are exposed daily in the social media and the proliferation of on-line surveys in digital platforms, we decided to develop a brief survey that could respond appropriately to the study aims in a timely manner. For that, we followed the recommendations of Schnall et al. (2018) on questionnaire development in the context of Disaster Epidemiology. Questions were intended not to be general and targeted specifically to “need to know” information. Directed and written in the simplest language possible. The goal is to have as few questions as possible to obtain the information required to meet the objectives. Since it is helpful to use questions from existing data collection instruments, some questions were partially extracted from WHOQOL-Bref (Fleck et al., 2000).
Prior to the beginning of the survey, informed consent was obtained from the respondents. Afterward, the survey explores patients´ socio-demographic information: age, gender, residency postal code, school level, civil status, household before and during quarantine, and professional situation. Individuals were also asked if they attended psychology or psychiatry consultations currently and checked regarding COVID-19 condition, namely if they have already been infected or hospitalized.
Subsequently, participants were asked to answer questions regarding their experience and psychological adaptation to the period of social isolation, expressly comparing it to the previous month. This part of the survey was constituted by 23 questions, organized in 4 dimensions: family life (3 items); professional life (4 items); behavioral habits (12 items), and psychic state (4 items). The responses were framed in a Likert format, in which participants are asked whether or not they agree with the statements. Each item consists of a five-point scale, ranging from “totally disagree” (1) to “totally agrees” (5). We initially pilot-tested the survey with 19 individuals to ensure the question wording is appropriate and understandable by our audience. This allows us to improve unclear questions or procedures and detect errors in advance. Small changes regarding wording were made. The pilot-test sample was removed from the study sample.
Statistical analysis
Nominal data were described by frequencies, ordinal data by medians and frequencies, and numerical data by means and standard deviations (SD). In preliminary analyses, we used χ2 analysis, t-student, and one-way between-groups analyses of variance (ANOVA) to examine baseline differences in demographics. Several one-way between-groups analyses of covariance (ANCOVA) were conducted, adjusted for age, school level, and the days of social isolation, to investigate associations between the baseline demographics variables and outcome variables. All statistical analyses were conducted using IBM SPSS Statistics version 25. The significance level for all analyses was set at p<0.05.
Results
Socio-demographic characteristics of the sample
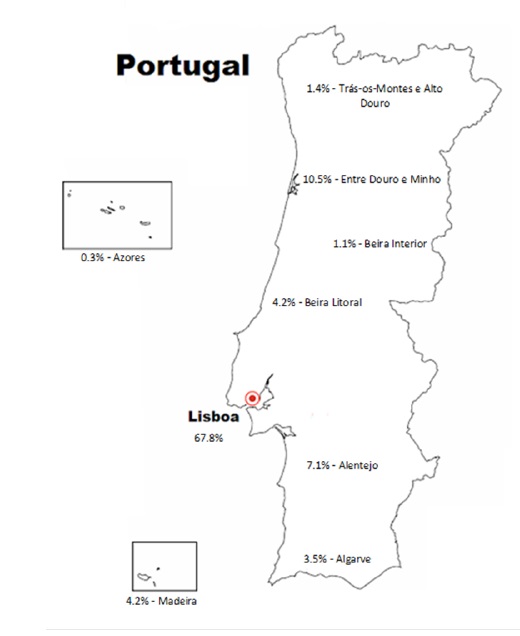
The average age was 41.8 years (SD = 12.4). The sample (N=1794) was mostly female (N=1243/69.3%), compared to males (N=551/30,7%), highly educated, married, from the Lisbon region, and employed in teleworking status. The average number of days of social isolation was 24.2 (SD=11.6). Socio-demographic characteristics are summarized in table 1. Gender comparisons revealed that there were no significant differences in age, geographic region distribution, marital and professional status, and household composition (p>0.05). However, females, when compared to males, showed a significantly higher level of education (χ2=27.0; p<0.01), as well as a higher number of days in social isolation (F=22.9; p<0.01).
Behavioral and emotional reactions
Several changes in daily habits and family and psychological life have been reported. Considering the answers in absolute values of agreement in the aspects that were evaluated in the study, it should be emphasized that this period of social isolation has served to value family life more (91.2%) and contributed to more pleasant moments in the family (77.9%). Only 31% of the cases reported that this period has increased family conflicts. People seem to feel satisfied with their capacity to work (69.4%) and from being able to do it from home (64.2%). They also report having a sleep of at least 7-8 hours a night (73%), eating a more balanced diet (62,6%), perform more leisure activities (57.2%) and physical exercise (45.3%) and have more time dedicated to doing what they like (58.4%). More than half mention that this period of confinement has increased the frequency of positive feelings, such as joy, hope, and confidence (56.3%), and is contributing to being able to better appreciate life (60%). In terms of maladaptive behaviors, 25.7% say they consume more alcohol and 12,2% illicit drugs. Almost half the smoking population reported smoking less (46.2%). 46.7% indicate that they have consumed fewer anxiolytics.
On the other hand, more than half of the sample reported difficulties in concentrating to work (57%), that their work is frequently interrupted (57%) and that their intimate/ sexual life has worsened (61.4%). About half say they feel that I now work more hours than I previously worked (48.8%). 61% said they had less care with food and weight and 46.2% less free time. The connection with technologies is clearly more present in daily life (88.5%). More negative feelings were reported, such as sadness, despair, or anxiety (65.1%), tension, and inability to relax or unwind (67.7%).
Gender comparisons
There were significant differences by gender concerning family, psychological, and behavioral adaptation to the period of social confinement, even after controlling for the effect of school level and the days of social isolation. Overall, females report a significantly more negative impact on their lives in this period of domestic confinement, when compared to males. ANCOVA revealed that females report more difficulties in concentrating on work (F (1, 1395)=4.9, p<0.05) and suffering more interruptions (F (1, 1311)=5.6, p<0.05) and less free time (F (1, 1570)=6,4, p<0,01). They also refer more often negative feelings (F (1, 1570)=53.4, p<0.01), such as sadness, despair, anxiety, tension, and an inability to relax (F (1, 1570)=22.7, p<0.01). In turn, males report, in general, greater satisfaction with their work performance (F (1, 1414)=13.9, p<0.01). Although they say they smoke fewer cigarettes (F (1, 508)=4.4, p<0.05), they are more involved in maladaptive behaviors such as consuming more alcohol (F (1, 1570)=15.4, p<0.01) or illicit drugs (F (1, 1508)=18.1, p<0.01).
Household structure
There were statistically significant results when assessing the structure of the household. Parents with children at home (a), compared to other forms of household (b.only with a partner, c.alone, d.other family members, friends, e.only with children), refer significantly more pleasant family moments (vs. a,c,d; F=71.6, p<0.01), more family conflicts (vs, a,c; F=18.0, p<0.01), work interruptions (vs. a,c,d,e; F=13.8, p<0.01), less free time (vs. a,c,d; F=16.7, p<0.01), and less time doing what they like (vs. a,c,d,e; F=7.1, p<0.01). Being alone is associated with a higher connection to technologies (vs. a,b; F=4.6, p<0.01), a worse intimate/sexual life (vs. a,b,d; F=22.3, p<0.01), and a higher consume of alcoholic beverages (vs. d; F=5.2, p<0.01). Who is living with other family members or friends during this pandemic period reported more family conflicts (vs, a,c; F=18.0, p<0.01), more opportunities for leisure activities (vs. b,d; F=9.3, p<0.01), a higher connection to technologies (vs. a,b; F=4.6, p<0.01), more physical exercise (vs. a,b; F=6.9, p<0.01), and a worse intimate/sexual life (vs. a,b,d; F=22.3, p<0.01).
Occupational status
Comparisons between people that were at the time: a. unemployed, b. employee in regular working functions, c. employee in lay off, d. teleworking, e. studying or f. retired, revealed significant differences.
Students reported more family conflicts (vs. a,b,c,d,f; F=7.4, p<0.01), more difficulties in concentrating on work (vs. a,b,c,d,f; F=22.6, p<0.01), more opportunities for leisure activities (vs. b,d,f; F=22.6, p<0.01), a higher connection to technologies (vs. b,d,f; F=5.4, p<0.01), a lower consume of alcoholic beverages (vs. a,c; F=4.1, p<0.01), and more physical exercise (vs. a,b,c,d,f; F=10.8, p<0.01).
As expected, individuals that were unemployed or in layoff reported poorer satisfaction with work performance (vs. b,d,f; F=22.6, p<0.01). No differences were observed between who was working on a regular basis and in teleworking. Individuals that were in teleworking reported feeling that work more hours now than previously, when in comparison with individuals that were working on a regular basis (F=9.6, p<0.01).
Health professional’s subgroup
When comparing health professionals (N=282) with other professionals (N=1096) in the most varied work regimes (Unemployed, students, household, and retired were not included in the analysis), there were statistically significant differences with regard to age and education. In our sample, health professionals respondents were younger (F=3.4; p<0.01) and more educated (χ2=51.6; p<0.01). Thus, the comparative analysis included age and education as covariates. In general, the negative impact of this period is evident. When compared with other professionals, health professionals refer that tend to valuing family life more (F (1, 1374)=7.5, p<0.01), have less pleasant family moments (F (1, 1374)=8.7, p<0.01) and fewer opportunities to perform leisure activities (F (1, 1374)=14.0, p<0.01), do not sleep at least 7-8 hours a night (F (1, 1374)=5.6, p<0.05), spend less time doing what they like (F (1, 1374)=3.9, p<0.05), less care with food and my weight (F (1, 1374)=5.4, p<0.05), and less physical exercise (F (1, 1374)=22.8, p<0.01). They also reported more often negative feelings, such as sadness, despair or anxiety (F (1, 1374)=5.8, p<0.05), less positive feelings, such as joy, hope (F (1, 1374)=8.7, p<0.05) and feeling more tense and unable to relax (F (1, 1374)=8.9, p<0.05).
Mental health assistance subgroup
Current attendance in psychiatric or psychological consultations was reported in 10.8% of the cases. After controlling for the effect of days in social confinement, respondents who reported being receiving some type of mental health assistance (N=191), comparing with who did not (N=1580), reported more family conflicts (F (1, 1550)=14.5, p<0.01), a worse intimate/sexual life (F (1, 1550)=7.2, p<0.01), more often negative feelings, such as sadness, despair or anxiety (F (1, 550)=20.4, p<0.01), less positive feelings, such as joy, hope (F (1, 1550)=4.5, p<0.05), and feeling more tense and unable to relax (F (1, 1550)=12.7, p<0.01).
Table 1 Socio-demographic characteristics by gender
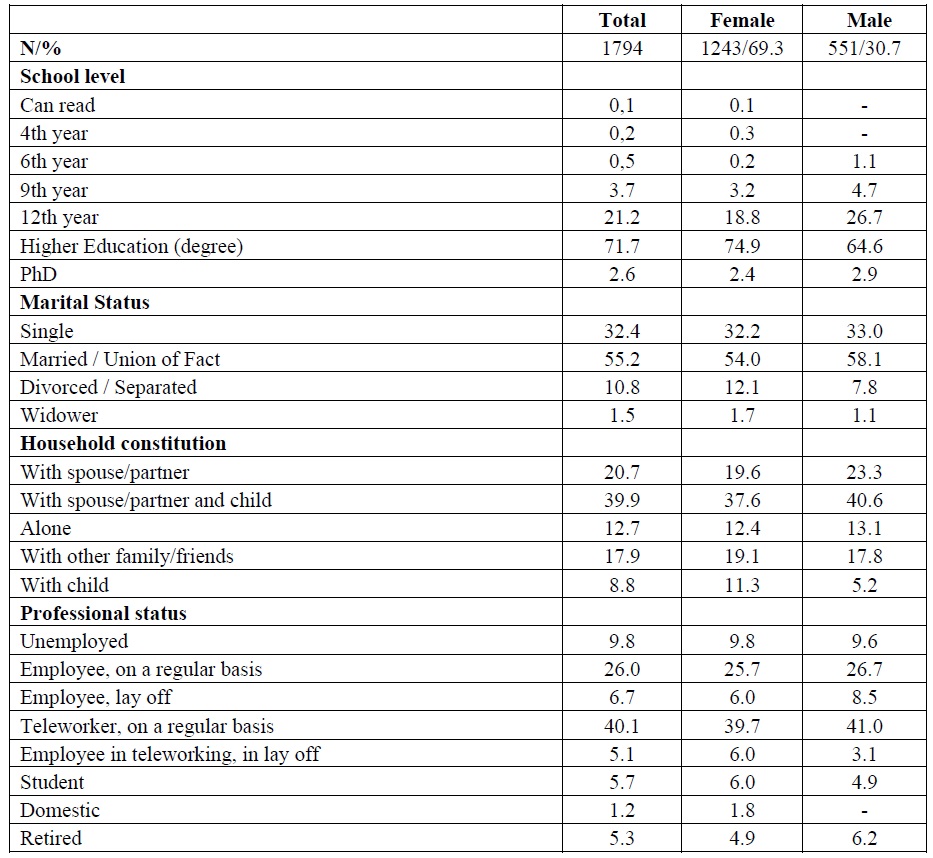
Note: Values are expressed in percentages. Groups were compared using the Qui-Square test.
Discussion
In the approximately four-week period of the state of emergency, the Portuguese people seem to have lived and adapted to the required social isolation in a way that combined both positive and negative psychological aspects. The results of this study show that some specific groups within the population were more vulnerable to the potentially negative costs of the lockdown; namely, females, parents with children who were at home, health care workers, and individuals with mental health issues.
Although studies report an increase in psychological stress, particularly as the pandemic progressed (Li et al., 2020; Ozamiz-Etxebarria et al., 2020; Wang et al., 2020), many people showed themselves to be resilient in the face of these stressors (Taylor, 2019). According to our results, as paradoxical as it seems, this phase of social confinement contributed to a series of gains in the personal and family lives of some individuals. Several factors may help to explain this apparently “benign” impact of confinement on a part of our population. One factor is that the state of emergency was announced earlier in Portugal than in many other countries, at a time when fewer people had been infected, and fewer deaths had been associated with the pandemic. Also, after the confinement began, the rate of progression of the disease slowed more than it did in many other countries (Roser et al., 2020), and this may have helped to reduce people's concerns about being infected or having a family member become infected. The Portuguese government also provided financial support to those who were required to stay at home, and many companies allowed their employees to work under flexible conditions in their homes. We hypothesize that because people locked themselves in their homes they may have found a remedy for another “pandemic”: the daily stresses marked by competition, pressure, and chronic feelings that they lacked the time to complete their tasks (Cohen et al., 2007; Epel et al., 2018). Using their time at home as opportunities for personal and family leisure seems to have been common, with activities that involved interaction with others in their homes playing an important role in combating loneliness and the psychological fatigue inherent in forced social isolation.
However, our data also reveal that the quality of life among some subgroups may have deteriorated during this period. For instance, gender comparisons have demonstrated that the personal costs of this crisis were much higher among women than among men. This probably reflects historical socio-cultural gender inequalities. For example, women have traditionally adopted roles as caregivers and also tend to make self-sacrifices within their families (Cantillon & Hutton, 2020; Ussher & Sandoval, 2008; Wenham et al., 2020). In addition, as the schools closed, women were probably the first who needed to stay at home, therefore starting their confinement earlier than men. In their homes, the women might also have been more responsible than the men for caring for children, cleaning, and preparing meals for all family members, while possibly also combining this with working remotely from the home. Another hypothesis, however, is that women may be more susceptible to the effects of social isolation or more vulnerable to experiencing anxiety and trauma-related and stress-related disorders (Li & Graham, 2017).
Our data also underlines the greater resilience required by couples whose children were at home, particularly young children. Parents needed to arrange for their support while themselves struggled to fulfill their work obligations from home. This could present difficulties regarding the management of everyday life and lead to increased conflict.
With regard to health care workers, this group is particularly exposed to the negative impacts of pandemics such the recent one (Brooks et al., 2020b; Xiang et al., 2020). This is especially true of frontline health care professionals, who are remarkably vulnerable to experiencing both self and social stigma. They must cope with the psychological distress of losing patients while at the same time trying to protect their own health (Park et al., 2018; Yahya et al., 2020). In addition to their perceptions of personal danger, health care workers were exposed to uncertainty through the constant, almost daily, sometimes hourly, modifications to infection control procedures and public health recommendations. Many health care workers also expressed conflict between their roles as health care providers and as parents, feeling on the one hand a sense of altruism and professional responsibility and on the other hand the fear and guilt associated with potentially exposing their families to infection (Maunder et al., 2003). Our study showed that health professionals reported that during the pandemic they had less leisure time, less time to sleep, more negative feelings such as sadness, despair or anxiety, and fewer positive feelings such as joy or hope. They also felt tenser and more unable to relax. Our results are in line with other studies showing that this pandemic has negatively affected the mental health and psychological wellbeing of health care workers in different countries (Blake et al., 2020; Chew et al., 2020; Lai et al., 2020) and pointing out that, even in countries like Portugal where the public health response and the hospital working conditions were reasonably controlled, health care workers still suffered from the effects.
Our study also found that people who required assistance with mental health issues were a vulnerable group. As Yahya et al. (2020) posited, the current crisis demands resilience and significant adjustment. However, those with predisposing vulnerabilities and existing mental health difficulties may lack the adaptive coping mechanisms or the supportive social networks to make this transition appropriately.
Several limitations should be considered with regard to our study. Although our data derive from a substantially large sample and follows the characteristics of the Portuguese population according to data from the 2011 census (https://censos.ine.pt), we must, nonetheless, highlight that the study population is highly educated and mostly female, married, from the Lisbon region, and employed in teleworking. Also, the method selected for the timing and data collection could have had an impact on the results. Web-based surveys are less resource-intensive and can garner many participants but are more likely to introduce selection bias (i.e., only those with Internet access may participate). Another limitation is the fact that we did not control for depression or anxiety syndromes in our population, and this could have impacted our results. However, we asked for information about current psychiatric support, and that could be used as a proxy for current major psychiatric syndromes.
In conclusion, there seems to be a balance between losses and improvements in quality of family life, behavioral and emotional well-being during the first 4 weeks of lockdown due to the COVID-19 pandemic, for the majority of the population studied. Nevertheless, some subgroups seem to be particularly affected by the impact of confinement showing an important deterioration of their psychological well-being, namely, women, health care professionals, couples with children at home, and individuals with current mental health assistance. Further studies are necessary to clarify the long-term consequences of social confinement, particularly in the subgroups that seem to be the most affected.

