











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkAlcohol Use Disorders (AUD) represent multi-dimen sional chronic conditions often associated with a long-term relapsing process (Lesch et al., 2011). The identification of patient's high-risk cues for alcohol or drug abuse is essential for alcohol treatment success. Collecting information about risk situations for alcohol use could be crucial to understand patient’s reasons to drink, difficulties to maintain sobriety after treatment and to generate an individually-tailored treatment program. Usually, high-risk situations that enhance the likelihood of substance use include intrapersonal events such as cognitions and emotional states, and interpersonal dimensions such as peer pressure. The pioneer and systematic work produced by Alan Marlatt and his colleagues (Marlatt & Gordon, 1985), give considerable support for an empirically-based typology of situations that present a high risk for relapse. Based on alcoholic’s interviews following discharge from treatment programs, the authors demonstrated that client descriptions of their primary relapse episodes could be classified in 8 categories: Unpleasant Emotions (UE), Physical Discomfort (PD), Pleasant Emotions (PE), Testing Personal Control (TC), Urges and Temptations to Use (UT), Conflict with Others (CO), Social Pressure to Use (SP), and Pleasant Times with Others (PO). This empirically-based typology of situations has been operationalized by Annis and their co-workers (1982; 1985). The authors developed the Inventory of Drinking Situations (Annis et al., 1982) and the Inventory of Drug-Taking Situations - IDTS (Annis & Martin, 1985) to assess the degree to which individuals are at risk for substance use in a variety of trigger situations.
In 1997, Turner et al. suggested that future lines of investigation should focus on comparisons across drug categories on the IDTS in order to increase our understanding of commonalities and differences among alcohol and other substance use (Turner et al., 1997). In that sense, several studies have been performed. The results of a previous research that examined high-risk situations in seriously mentally ill individuals who have alcohol and drug use disorders, suggest that high-risk situations are similar for dually diagnosed individuals regardless of whether they abuse drugs or alcohol. Indeed, the analyses of variance conducted to compare the primary alcohol and drug groups on the IDS/IDTS scale scores found no statistically significant differences between the groups. Among the various hypotheses to explain the absence of differences in the groups, the authors proposed that the pattern of polydrug use may have produced heterogeneity in the samples in comparison (Bradizza et al., 1998). El-Sheikh Sel and Bashir (2004) in Saudi Arabia, compare alcoholics and heroin addicts on both high-risk relapse situations and situational confidence. The results indicate that the highest high-risk relapse situations are UE, TPC, SP and UT. Heroin addicts showed statistically significant high mean IDTS scores compared with the alcoholic’s sample, namely, PD, SP, and PT. The authors explained these results by clinical observations. They mention that generally heroin patients argued that they use drugs to relieve the physical pain or some other sickness trouble. Furthermore, high scores on PT can be based on the idea that heroin addicts usually use drugs to increase sexual enjoyment and habitually depend on this skill to maintain ongoing proper sexual functioning. Due to the nature of their substance addiction, heroin addicts may have developed poor self-efficacy to resist urges when confronted with peer and social pressure. After, Waldrop et al. (2007b) compared high-risk triggers and situations among persons with alcohol or cocaine dependence, with or without posttraumatic stress disorder (PTSD). The results were consistent with the self-medication hypothesis, in which PTSD+ subjects reported significantly greater substance use in response to negative situations, as compared to PTSD− subjects. It was suggested that PTSD+ subjects experience high rates of unpleasant emotions and physical discomfort, and use substances in an attempt to minimize such symptoms. The same group, in a study about daily stressor sensitivity and cocaine use among individuals who were cocaine dependent, observed that men and women who are more sensitive to daily stressors are more likely to report using cocaine in negative situations and temptation situations. Among men, use in positive situations was associated with greater sensitivity to daily hassles (Waldrop et al., 2007a). Hartwell et al. (2012) examined motives for drug use between non-treatment seeking individuals with current prescription opioid, marijuana, or cocaine dependence. Results showed that individuals with prescription opioid dependence reported using substances more often to relieve PD than did individuals with marijuana or cocaine dependence. The prescription opioid and cocaine dependent groups were more likely to identify TC as a motive for use, as compared to the marijuana group.
In sum, addiction clinical units should train patients on relapse prevention methods in order to achieve long-term recovery. Better results will be achieved if the treatment is directed to the patient specific needs (Pombo, 2016). However, the understanding of each person's unique dynamic for relapse is complex considering that the concomitant use of multiple substances in the brain is nowadays the rule rather than the exception (Novais et al.,, 2016; World Health Organization, 2019). Indeed, different “secondary” addictions and drug use combinations in alcohol-using populations make it more difficult to understand alcohol use relapse patterns and trends. Therefore, this study will explore the differences in relapse’s risk factors between patients with only AUD and patients with a diagnosis of AUD with past history of drug addictions.
Method
Participants
A correlational and comparative study was planned to assess high-risk situations for alcohol use among two types of addiction. Study participants were recruited in the alcoholism and addiction units of the Psychiatric Service of Santa Maria University Hospital. All patients taken from the therapeutic program fulfill the criteria for alcohol dependence according to the Diagnostic and Statistical Manual version 5 (DSM-5) (American Psychiatric Association, 2013). At the time of the assessment, 74.8% of the subjects were abstinent for at least 2 weeks. The others were stabilized from their drinking habits. Psychiatric co-morbidity was measured by the Mini Neuropsychiatric Interview (Sheehan et al., 1998).
The study will be comparing 2 groups of patients: patients with a diagnosis of alcohol use disorder (AUD) without drug use disorder comorbidity (“pure AUD patients”) and patients with a diagnosis of AUD with past history of drug addiction (“poly-addicted AUD patients”). For that, patients were asked whether they had used different drugs, especially cocaine, heroin and cannabis. They were also assessed about addiction features of each of these substances. In order to be categorized as “poly-addicted AUD patients”, individuals must fulfill DSM-5 criteria for another substance addiction (heroin 36.7%, cannabis 49.2%, and cocaine 44.8%). Recreational and/or sporadic use of other drugs was not considered.
The study was approved by the local Ethical Board of Medical School of Lisbon (REFa DIRCLN).
Material
The following variables were measured: drinking and substance use habits and socio-demographic information were collected at patient’s hospital admission with a standardized interview. Quantity-Frequency method (QF) was used to quantify the average of alcohol consumption. Craving was measured with the Penn Alcohol Craving Scale (PACS) and high-risk situations for heavy alcohol use with the Inventory of Drug-Taking Situations (IDTS) - alcohol version.
In our analysis, we take into consideration previous findings that demonstrate the significant impact of state-dependent factors as well as the trait-related characteristics (e.g., gender, life-time history of major depression disorder) on high-risk situations measurement using IDTS (Abulseoud et al., 2013; Lau-Barraco et al., 2009; Waldrop et al., 2007b). Moreover, since research approaches have been indicating IDTS as a successfully measured of craving (Abulseoud et al., 2013; Karpyak et al., 2016; Karpyak et al., 2019), we also decided to include a psychometric craving measure in the analysis: the Penn Alcohol Craving Scale (PACS).
Statistical analysis
The normal distribution of the psychometric measures was confirmed using the Kolmogorov-Smirnov test. Thus, considering normally distributed data, parametric methods were used to calculate numerical relations among variables.
Comparisons among gender regarding baseline variables (socio-demographic and drinking data) were performed using chi-square and student t-tests. Assuming that we could observe a significant interaction between socio-demographic/drinking variables, the groups comparisons were performed with a one-way ANCOVA (analysis of covariance) in order to assess whether the subgroup differences were attributable to covariate factors.
Data were analyzed using the Statistical Package for Social Sciences (SPSS - Version 24.0). Statistical significance was defined at p <0.05.
Instruments
Semi-structured interview for alcohol dependent patients
This interview explores patients´ socio-demographic and drinking information. It has been used in several other studies (Lesch et al., 2011; Pombo et al., 2016; Pombo et al., 2008).
MINI (Mini Neuropsychiatric Interview)
The MINI is a short and rapid structured diagnostic interview, created to assess 17 psychiatric disorders. This instrument can be easily incorporated into the clinical practice routine with an administration time of approximately 15 minutes (Sheehan et al., 1998). The MINI is nowadays available in almost 30 languages, including Portuguese (Amorim et al., 2000).
Quantity-Frequency method (QF)
QF method is a fast alcohol consumption measure that quantifies the weekly average alcohol consumption per drinking day. This estimation formula was used in order to compute the average number of drinking days over a certain period (typical week) and then to estimate the average number of drinks consumed per drinking day. The QF drinking variable was then calculated as the product result of those measures (in standard drinks) - average number of drinks per week. A standard drink was defined as one beer, one glass of wine, one glass or shot of liquor. In the cases of alcohol abstinence, patients were asked about the last week of alcohol consumption before they stopped drinking.
Inventory of Drug-Taking Situations (IDTS) - alcohol version
Originally, the IDTS was generated from an equivalent instrument - the Inventory of Drinking Situations (Annis et al., 1982; Annis & Martin, 1985). Developed in the Addiction Research Foundation in Toronto by Annis and coworkers, the Inventory of Drug-Taking Situations (IDTS) is a 50-item self-report questionnaire that provides a profile of the situations in which an individual has used a substance of abuse. Each item consists of a four-point scale, ranging from “never” to “almost always”. Higher scores indicate greater frequency of drinking in that situation. The IDTS can be administered either through interactive computer software or in a paper and pencil format.
The drug-taking situations assessed on the IDTS are based on Marlatt's 8-category classification system of common antecedents to drug use. The IDTS offer for each client a split profile of the situations in which a client has used a particular drug above the past year. The individual is assessed in relation to eight categories of high-risk situations: UE, PD, PE, TC, UT, CO, SO and PT. IDTS also presents a second order factor constituted by three global categories: 1. (N) Negative situations (combining UE, PD and CO); 2. (P) Positive situations (combining PE and PT) and 3. (T) Temptation situations (combining UT, SO and TC). Clients are asked to specify their frequency of drug use or heavy drinking in the past year. The IDTS has two versions, one for illicit drugs and one for alcohol. Previous results suggest that the IDTS can be used in place of the Inventory of Drinking Situations with alcohol users (Turner et al., 1997). The alcohol version was used in this study. This instrument has demonstrated high levels of validity and reliability with a Cronbach coefficient alpha of 0.95 for the IDTS total score, ranging from 0.70 to 0.87 for the subscales (Turner et al., 1997). Taking into account that the studies in which this instrument was used in the Portuguese language do not show references to its psychometric characteristics (Silva & Quintas, 2010), the psychometric analysis of the IDTS was an additional goal of this study.
Penn Alcohol Craving Scale (PACS)
The PACS was designed by Flannery et al. (1999) as a craving assessment tool. It is a brief self-administered instrument, with a multi-item unifactorial structure consisting of five items. This scale has shown good psychometric qualities in terms of reliability (Cronbach's α=0.92), and concurrent, predictive, and discriminant validity (Flannery et al., 1999). This instrument has been validated in Portuguese alcohol-dependent outpatients (Cronbach's α=0.94), with good psychometric properties (Pombo et al., 2008).
Results
The sample comprised 128 patients, 104 males (81.2%) and 24 females (18.8%). Age varied between 27 and 66 years, with a mean value of 45.5 years (DP=9.7). Regarding civil status, 34.1% were married or lived in a marital union, 35.8% were single and the others were separated/divorced (30.1%). The mean value of school attendance was 9.0 years (DP=4.3). Regarding professional activity, 56.9% were active workers, 32.5% were unemployed and the rest were retired (10.6%). Concerning drinking history, the weekly average of alcohol consumption per drinking day was 99.6 (DP=90.1) and the average age of drinking onset, alcohol misuse and AUD were 14.5 (DP=3.8), 24.3 (DP=8.0), 32.5 (DP=9.1), respectively. Approximately half the sample reported Family History of Alcoholism (57.1%) and previous history of alcohol detoxifications (58.2%). Seizures were observed in 12.4% of the cases. Lifetime diagnosis of depression (MINI) was observed in 30.3% of the patients. Considering gender differences, as expected, male patients started to misuse (F=8.3; p<0.01) on alcohol significantly earlier when compared to female patients and the lifetime diagnosis of depression was more prevalent among female patients (X2=6.4; p<0.01) when compared to male patients. No other significant differences were observed between genders. Initial analyses revealed no gender differences in IDTS (p>0.05). The same was observed regarding the relation between past history of major depression disorder and IDTS (p>0.05). This eliminates concerns about a potential confound of gender and depression.
Psychometric properties of the Inventory of Drug-Taking Situations (IDTS) - alcohol version
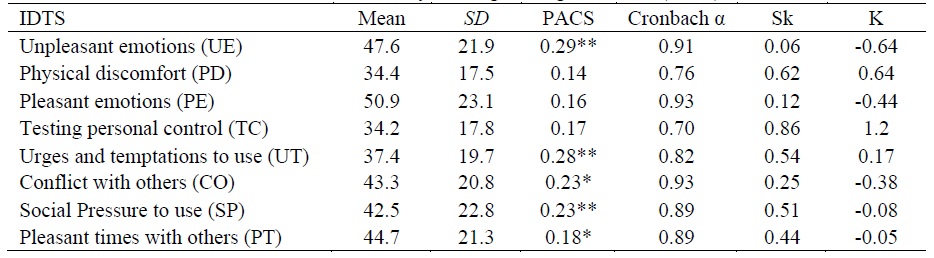
Considering mean values of the IDTS subscales, patients reported higher scores on the dimensions UE, PE, CO, SO and PT, followed by UT, TC and PD. The statistics of IDTS is presented in table 1. Cronbach's coefficient alpha was used to estimate internal consistency of the scale and each of the 8 subscales. For the total scale (50 items), the alpha was 0.96. All the subscales had alphas above 0.70, indicating good internal consistency. All items positively correlated to their subscales, with the following ranges: UE (item 9 0.70 - item 3 0.80), PD (item 14 0.55 - item 11 0.76), PE (item 20 0.83 - item 19 0.93), TC (item 21 0.55 - item 22 0.76), UT (item 26 0.67 - item 30 0.82), CO (item 37 0.71 - item 34 0.85), SO (item 44 0.73 - item 41 0.84), and PT (item 50 0.71 - item 48 0.90). Corrected item-total correlations, that is, the correlation between each item and a scale score that excludes that item, showed that all items presented positive correlations above 0.30, ranging from item 14 (0.34) to item 48 (0.75). The estimation of the construct validity was made by correlating the IDTS scores with alcohol-use-related variables. Since the IDTS aims to identify specific situations in which a patient tends to engage in excessive alcohol use, it was expected to correlate with the levels of reported craving, as measured with the PACS. Table 1 presents the correlations of the IDTS with the PACS. Support was found for a significant positive relation between the scores of PACS and the subscales of IDTS. As expected and taking into account the phenomenology of craving, PACS significantly correlated with the IDTS dimensions of UE, CO, PT e particularly UT.
Group comparisons (“Pure AUD” vs. “poly-addicted AUD”)
Comparative analysis reveals some significant differences among the subgroups. “Poly-addicted AUD patients” were younger (F=12.7; p<0.01) and presented a lesser educational status (F=25.3; p<0.01), when compared to “pure AUD patients”. PACS scores were significantly higher among “Poly-addicted AUD patients” when compared to “pure AUD patients” (F=11.6; p<0.05). There were no other significant differences between groups regarding socio-demographic features and drinking related variables.
Bivariate analysis showed that the subscale “urges and temptations to use” and “conflict with others” of IDTS significantly correlate age (r=-0.23, p<0.01; r=-0.18, p<0.01, respectively). No significant relations were observed between IDTS and other socio-demographic features or drinking related variables. Comparative analysis showed that the scores of the dimensions PE, SP, PT and the factors “positive situations (P)” and “temptation situations (T)” were significant higher among the poly-addicted AUD subgroup when in comparison with the “Pure AUD subgroup” (see table 2). However, considering that the subgroups significantly differentiate in terms of age, educational level, craving and drinking chronology and we observed a significant interaction between IDTS and age, an analysis of covariance (ANCOVA) was conducted to compare the profile of high-risk situations for alcohol use among the subgroups, using age, years of education and PACS as covariate variables. Thus, following an ANCOVA, bonferroni corrected multiple comparisons tests identified significant differences in PE (F1 100=4.3; ηp2=0.81; p<0.05), SP (F1 100=7.4; ηp2=0.59; p<0.05), PT (F1 100=5.7; ηp2=0.45; p<0.05) and P (F1 100=4.8; ηp2=0.39; p<0.05). All results are summarized in table 2.
Table 2 IDTS scores according to subgroups
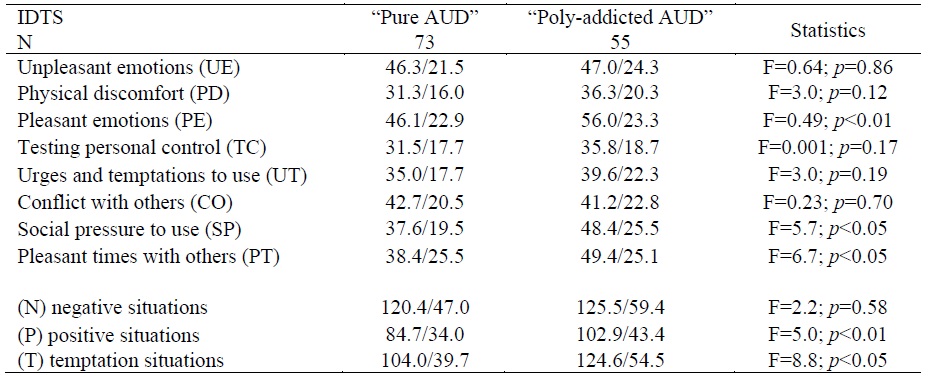
Note: IDTS (Inventory of Drug-Taking Situations), “Patients with a diagnosis of alcohol use disorder (AUD) without drug use disorder comorbidity (“pure AUD patients”), patients with a diagnosis of AUD with past history of drug addiction (“poly-addicted AUD patients”). Values are expressed in means and standard deviations (M/SD). Groups were compared using Student t (F) tests.
Discussion
The aim of this study was to determine whether or not two different subgroups of alcohol dependent patients use alcohol in response to high-risk drinking situations. Findings revealed significant differences in motives for alcohol use among the subgroups.
Considering the psychometric properties of the alcohol version of the IDTS assessed in the current study, i.e. item characteristics, reliability and validity, the results were comparable to those reported in other studies (El-Sheikh Sel & Bashir, 2004; Lau-Barraco et al., 2009; Pashaei et al., 2013; Turner et al., 1997). Cronbach’s alpha was 0.96 for the total scale. Overall, the results provide preliminary support for the use of IDTS in research and clinical settings.
Negative situations have long been stated to be the most frequent alcohol relapse cause (Bradizza et al., 1998; Mousali et al., 2020; Shafiei et al., 2014). A previous study by Connors et al. (1988) suggests that expectations regarding the utility of alcohol in relapse situations revolve predominantly around mediating or getting through difficult situations, principally dealing with or coping with intrapersonal or interpersonal conflicts in a social situation. In a 24-month follow-up, the authors assessed what factors had contributed to any returns to drinking. Results showed that almost half of the expectancies reported dealt with drinking as an aid in coping with a social situation. Another one-quarter of the expectancies dealt with drinking to gain control of a situation, with the remainder divided between drinking to cope with a non-social situation or to create an altered physical state. In the Bradizza et al. (1998) study, the data for the alcohol group indicated that experiencing unpleasant emotions was a slightly higher risk situation for alcohol use, and all other situations were about equal risk. In contrast, the drug group found two situations-social pressure to use and pleasant times with others-to be the highest risk situations for drug use. These conclusions go in accordance with our main finding, which is that poly-addicted AUD patients, when in comparison with “pure” AUD patients, are more prone to drink alcohol when they are feeling good or socially pressed, though with different samples considered. This result is partially supported by studies that have previously documented an association between some specific drugs and situations involving pleasant or positive feelings or events (Kelly & Parsons, 2008; Hartwell et al., 2012; Starks et al., 2010). In a study comparing high-risk situations among persons with alcohol or cocaine dependence, with or without PTSD, Waldrop et al. (2007b) argued that cocaine may actually improve the ability to tolerate social settings for some PTSD+ individuals and may enhance hypervigilance, allowing PTSD+ individuals to feel safer or more in control in public/social settings. Also, cocaine's stimulant properties may enhance self-confidence for social settings. In contrast, alcohol may lead PTSD+ individuals to feel a loss of control and dampened hypervigilance due to sedative properties. A recent study offers novel data on the interaction between situational risk factors and physiological features in cocaine use in women. In a double-blind study, it was hypothesized that women with higher IDTS scores would have a greater cortisol response to the cue-reactivity task while receiving yohimbine versus placebo. Results showed that elevated situational use factors (negative, positive, and temptation as defined by the IDTS) were associated with higher cortisol reactivity (Campbell et al., 2019).
With respect to the mechanism that may underlie our main finding, we can hypothesize that this subgroup is doubly (alcohol + drug) vulnerable to substance-related cues, influencing cognitive related beliefs, coping strategies effectiveness and drinking related-decisions. Once facilitated by a process of Pavlovian learning, in which repeated reward experiences are associated with the environmental stimulus, these situationally precipitants for alcohol or other drugs use mutually activated brain reward regions causing a pronounced increase in dopamine release. Repeated alcohol/drug consumption episodes promote a neural sensitization of mesolimbic dopamine neurons causing a long-term hyperreactivity in the dopaminergic transmission due to repeated dopamine releases. As a result, certain brain systems become hypersensitive to specific associated contexts (locations, “friends” of consumption). In other words, circumstances trigger and modulate the power of motivational incentive (Kalivas & Volkow, 2005).
According to the literature, men seem to drink mostly in the context of pleasant emotions while women more often when experiencing negative emotions. However, the studies are still inconclusive with regard to the mechanisms that may underlie this variance. For example, it may be due to subsyndromic presentation and/or specific symptoms of depression and/or anxiety (Abulseoud et al., 2013; Karpyak et al., 2016; Karpyak et al., 2019; Lau-Barraco et al., 2009). Although we currently have some accumulated evidence indicating that negative and positive emotions may impact alcohol consumption contexts in a sex-specific manner, possibly mediated by dysregulated affective states, we did not found any significant relationship between IDTS, gender or history of major depression disorders.
There are several limitations that need to be considered in the study. First, our data was collected on a cross-sectional basis. Second, it was impossible to specify what type of drug could be associated with a particular high-risk situation. Third, our population comes from a specialized care unit which makes these patients more likely to present a more severe alcohol problem, limiting the generalizability of the findings. Fourth, retrospective self-reports are subject to recall bias. Fifth, the contextual use of multiple substances by an alcohol dependent individual over a longer period of time might also reflect personal needs connected to personality functioning. Personality characteristics seem to interact with other biological, psychological and social environment variables in the development of polydrug-taking behavior. Although it was not properly measured in the study, we may posit that the personality traits of poly-addicted AUD patients might contribute to explain the results. For instance, “openness to experience”, a personality trait strongly connected with the sensation seeking construct (need for excitement, adrenaline rush), have been hypothesized to promote a behavioural functioning marked by emotional and intellectual curiosity that, when linked to frequent alcohol intoxication, leave alcohol dependent patients more prone to experience the effects of other drugs. These traits have been attributed to extraverted and impulsive individuals and are related with the proneness to high stimulating activities such as adventure sports, intake of drugs, sex, illegal activities, and so forth as well as the willingness to take risks in pursuit of novelty (Aluja et al., 2003; Novais et al., 2016; Zuckerman & Neeb, 1979). Finally, we cannot exclude the influence of poly-substance use in the clinical profile of AUD patients. For instance, poly-addictive individuals could be more disposed than alcohol dependents to self-report high-risk situations. We agree with El-Sheikh Sel and Bashir (2004), who claim that “typical” alcoholic participants tend to have severed defenses, which may make them hesitant in identifying their real high-risk situations.
In conclusion, contextual motives for drinking are important predictors of relapse. Our findings suggest that in dually diagnosed individuals (alcohol and drug addiction), when compared to “pure” alcohol dependent patients, positive drug/alcohol (conditioned) reinforcement may play a role in high-risk situations. Because drugs can potentiate positive emotions, it seems probable that polydrug patients might be more reactive to individual or environmental events connected to positive experiences. Because effective cognitive behavioral treatment to prevent relapse involves teaching patients how to successfully anticipate and cope with the high-risk situations, our data suggest that is necessary also to monitor positive situations.
Therefore, future studies should have a longitudinal design to better understand the real impact of polydrug consumption to relapse in high-risk situations.

