











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
The Surgical Center is a critical-hospital environment, complex due to technical and technological specificities, where patients who need to undergo anesthetic-surgical procedures, whether elective or urgent or even emergency are taken, in search of diagnostic and/or therapeutic treatment (Martins & Dall’Agnol, 2016). This context and these characteristics give to this unit a scenario marked by stressful situations, which tend to increase progressively as advances in the operative moments are consolidated (Bopp et al., 2013) for both surgical team and patients (Chrouser et al., 2018).
Stress is an English word that originates from the Latin term “stringere” and has the sense of distressing, tightening, describing a threatening situation on the body (Daian et al., 2010). This phenomenon is defined as a state of tension present in new conditions or considered risk situations, which causes a rupture in the balance of the organism by exceeding the adaptive capacity of the person (Kurebayashi et al., 2012).
The study on large surgery corroborates the definition of stress by mentioning that this disease describes not only stimuli that generate breakage in homeostasis in the body, but also behavioral responses created by such imbalance. This study presents historical aspects of the phenomenon, and thus mentions that Hans Selye, a German endocrinologist and precursor of studies in the area, considered stress as three-phase: alarm (initial alert phase where the patient experiences contact with a stressing agent and activates the neuroendocrine system); resistance - phase where internal homeostasis is broken and the person seeks the rebalancing of the organism; and exhaustion - phase arising from the persistence of exposure to the stressing agent (Daian et al., 2012).
The meaning of stress phases focuses on reflecting on the apparent consensus of studies that attribute to surgical treatment the profile of great stressor (Nobre et al., 2011; Oliveira et al., 2019; Parvan et al., 2012) as a new and abruptly imposed experience, able of disrupt the emotional system of the patient (Nobre et al., 2011), in view of the uncertainty regarding surgery and anesthesia (Oliveira et al., 2019). Thus, it is worth highlighting that organic reactions to stress primarily activate the hypothalamic-pituitary-adrenal axis, which, in turn, triggers the production of hormones (adrenaline, noradrenaline and cortisol). The release of these hormones, aiming to produce physiological responses, may or may not prepare the individual to face the stressful condition (Nodari et al., 2014).
In the context of coping and stressful conditions, a study conducted in the preoperative period, pointed out that "Facing surgery as a treatment option to improve or solve the problem" were predictors of lower stress levels; while waiting for surgery, fear of procedure and death were the first causes of patient distress (Esplendori et al., 2018). In the postoperative period, another study revealed that anxiety, pain and lack of information about treatment represent the main factors that lead to the patient's physical and emotional stress (Bagheri et al., 2016).
These references refer to scientific evidence that in the perioperative period the mobilization of expressive amounts of mental and psychic energy by the patient, which causes emotional exhaustion and may compromise their recovery (Daian et al., 2012). These facts, which could be mitigated with interventional measures of orientation to the patient about the procedure to which he or she will be submitted (Lemos et al., 2019).
Therefore, to watch over the phenomenon of stress from the perspective of the patient is essential for the promotion of more humanized care and with a view to a faster and less traumatic recovery (Magalhães et al., 2014). However, it is verified that stress situations related to surgical patients seem to have few approaches in the literature (Daian et al., 2012) and part of investments in the area is directed to studies from the perspective of stressor factors and implications for the patient in the operative moments (Bagheri et al., 2016; Esplendori et al., 2018; Oliveira et al., 2019; Parvan et al., 2012).
On the other hand, it is understood that the perception of nursing about stressors involving the surgical patient and their relationship with clinical practice, will help in the quality of care, reduce the impacts of stressors on the surgical patient and promote patient safety (Parvan et al., 2012); to the extent that it will promote holistic care between perioperative moments and strengthen the dialogue between the patient and the team; in order to review causes of fears, anxiety and doubts (Torrati et al., 2010).
In view of the above, this study aimed to identify through scientific evidence the nursing interventions used to manage stress in surgical patients in the operative moments.
Method
This is an integrative literature review developed based on steps proposed by Mendes et al. (2008). In the construction stage of the research question, the Problem, Interest and Context (PICo) strategy was applied, used in non-clinical research. The following were defined: P= stress I= surgical patient Co= nursing interventions. Thus, the guide question was established: What nursing interventions are used to manage the stress of surgical patients in operative moments?
Inclusion and Exclusion Criteria
Primary scientific studies conducted with adult patients (18 years or older) within the perioperative context were included. Studies that described nursing interventions for the management of surgical patient stress in this context and studies that addressed the anxiety of surgical patients were considered (Lemos et al., 2019). Nursing interventions as "any treatment, based on judgment and clinical knowledge, that is performed by a nurse to improve the results of the patient/client" (Bulechek et al., 2010) were considered. Studies in which patients underwent outpatient surgical procedures, texts unavailable in full and articles that did not make clear among the team of researchers whether the nurse was the professional responsible for the intervention were excluded.
Search Strategy
The databases used for the search were Scientific Electronic Library Online (SciELO); Latin American and Caribbean Literature on Health Sciences (LILACS); PUBMED; Cumulative Index to Nursing and Allied Health Literature (CINAHL) e SCOPUS. For each database, a search strategy was defined, considering the use of descriptors, keywords and Boolean operators: "stress and patients and surgery and nursing", in the languages in Portuguese, English and Spanish.
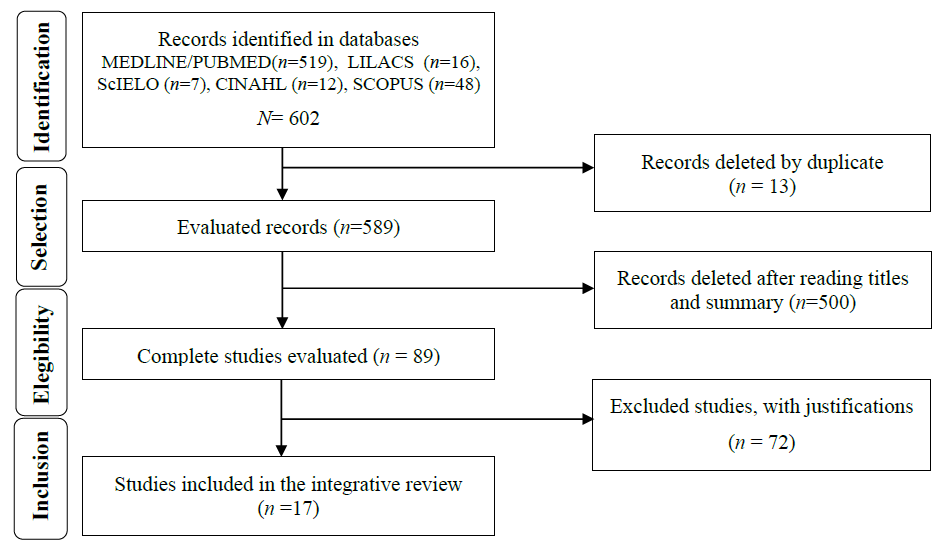
The search in the databases was carried out in July and August 2020, having as time delimitation the last ten years (2010-2020). The search and selection process were performed independently by three researchers. The steps covered were: 1. Search in the databases; 2. Removal of duplicate articles; 3. Selection of articles through the title and abstract; 4. Complete evaluation of the eligibility of the studies, discussion of discrepancies and consensual decision for the final sample of the stage of categorization and analysis of the data. The results of this process are described in the flowchart shown in Figure 1.
Results
In a general context, it is observed that the data show methodological diversity in conducting studies and a greater concentration of research published in American journals (70%, n = 12). These findings corroborate previous data cataloged in Brazilian literature (Daian et al., 2010; Daian et al., 2012). In regarding the design of the studies, it was observed the ones published in English (n=13), 46% (n=6) were randomized clinical trials (Bahrami et al., 2013; Bikmoradi et al., 2015; Daian et al., 2010; Fazlollahpour-Rokni et al., 2019; Garcia et al., 2018; Hudson et al., 2015). While in studies in Portuguese (Bittar et al., 2012; Coppetti et al., 2015; Costa & Sampaio, 2015) and Spanish (Rojas & Azevedo, 2013) there was a predominance of descriptive studies.
In addition, at the another analysis, the nurse's role in the care of surgical patients and in the perspective of stress management was viewed more frequently (59% of investigations) in the preoperative moment (Bahrami et al., 2013; Bittar et al., 2012; Coppetti et al., 2015; Costa & Sampaio, 2015; Fazlollahpour-Rokni et al., 2019; Garcia et al., 2018; Gürsoy et al., 2016; Hosseini et al., 2016; Ko & Lin, 2012; Nazari et al., 2012; Rojas & Azevedo, 2013) including for all studies conducted in Brazil (Bittar et al., 2012; Coppetti et al., 2015; Costa & Sampaio, 2015; Garcia et al., 2018). On the other hand, the intraoperative period was reached by only 3 (18%) of the American studies (Handan et al., 2018; Hudson et al., 2015; Jiménez-Jiménez et al., 2013), in vascular (Hudson et al., 2015; Jiménez-Jiménez et al., 2013) and obstetric interventions (Handan et al., 2018).
Table 1 Synopsis of the main information of the 17 primary studies included in the integrative review.
| Study | Context | Methodology | Intervention | Results |
|---|---|---|---|---|
| Bittar et al., 2012 | Preoperative (Cardiac Surgery) | Descriptive, Exploratory, Prospective Study | The nursing intervention as a form of surgical preparation contributed to the reduction of anxiety and stress in the face of surgery. | Preoperative visit and delivery of Manual of Pre and Postoperative Guidelines of Cardiac Surgery with clarification of doubts. |
| Costa & Sampaio, 2015 | Preoperative (General Surgery) | Descriptive Study, Almost Experimental | The levels of trait and anxiety status of the oriented patients remained low; Patients not guided by the nursing team significantly increased their anxiety levels. | Preoperative nursing guidelines. |
| Coppetti et al., 2015 | Preoperative (General Surgery) | Descriptive Qualitative Research | The orientations received were important to minimize the feelings that contributed to the triggering of stress and the resulting effects. | Preoperative nursing guidelines. |
| Rojas & Azevedo, 2013 | Preoperative (General Surgery) | Comparative Quantitative Study, Descriptive Analytical | Patients submitted to the educational program did not present anxiety before and after surgery compared to patients in the control group (those who did not receive an educational program). | Educational intervention on the operative process. |
| Ko & Lin, 2012 | Preoperative (General Surgery) | Almost Experimental Study | The relaxation Digital Versatile Disc (DVD) significantly reduced the level of anxiety and vital signs related to anxiety in surgical patients. | Relaxing DVD delivery one day before scheduled surgery. The tests were performed before and after the patients watched the DVD. |
| Nazari et al., 2012 | Preoperative (Ophthalmology) | Interventional Study | Hand massage 5 minutes before ophthalmologic surgery (under local anesthesia) reduced anxiety in patients. Therefore, this method can be used to increase patient comfort and reduce anxiety before surgical intervention. | Hand massage to improve anxiety in patients undergoing ophthalmologic surgery with local anesthesia. |
| Jiménez-Jiménez et al., 2013 | Intraoperative (Vascular) | Randomized Prospective Trial | The music therapy intervention implemented in the context of nursing care received during varicose vein surgery was positively accepted and valued by most patients in reducing anxiety and stress in the study patients. | The experimental group received a passive intervention of music therapy that consisted of hearing musical fragments during varicose veins surgery. |
| Bahrami et al., 2013 | Preoperative (General Elective Surgery) | Randomized Clinical Trial | Serum cortisol (stress hormone) levels were lower in the intervention group compared to the control group. | Evaluation of patients based on the nursing process and necessary training in anxiety reduction techniques. |
| Lim et al., 2014 | Postoperative (Orthopedics) | Pre-Test-Post-Test Almost Experimental Study | After the intervention, participants reported significant reduction in pain, stress and anxiety | Patients in the postoperative period of total knee arthroscopy were submitted to three relaxation interventions composed of breathing exercises, muscle relaxation and guided images. |
| Bikmoradi et al., 2015 | Postoperative (Cardiac Surgery) | Simple Randomized and Blind Trial | Lavender essential oil instilling aromatherapy had no significant effect on mental stress and vital signs in patients after CABG, except for systolic blood pressure | Lavender essential oil aromatherapy to reduce mental stress and improve vital signs of patients after myocardial revascularization surgery (CABG) |
| Hudson et al., 2015 | Intraoperative (Vascular) | Prospective, Non-Blind, Randomized and Controlled Study | Intraoperative anxiety assessments were significantly lower when participants interacted with nurses, used anti-stress balls, or watched a DVD during surgery compared to the usual treatment. | Participants were randomly allocated for intraoperative distraction techniques: patient-selected music, patient-selected DVD, interaction with nurses, touch (stress balls) or treatment as usual. |
| Saatsaz et al., 2016 | Postoperative Period (Obstetrics) | Single-Blind Clinical Trial | There was a significant reduction in the level of anxiety and a significant increase in the frequency of breastfeeding after massage. This intervention may be useful in the management of postoperative pain and stress. | Application of hand and foot massage |
| Hosseini et al., 2016 | Preoperative (Cardiac) | Single-Blind Clinical Trial | The results showed the positive effect of aromatherapy (lavender essence) on anxiety and cortisol level in patients' blood | The study and control groups instilled two drops of lavender and distilled water for 20 min, respectively. |
| Gürsoy et al., 2016 | Preoperative (General) | Almost Experimental Study | The nurse's visits to the patient before surgery contributed to the reduction of preoperative stress levels | Preoperative visits of the CC nurse, one day before the surgical procedure. |
| Garcia et al., 2018 | Preoperative (General) | Randomized Clinical Trial | On the eve of the surgical procedure, the care and attitudes offered by the nurse to the patient were effective in reducing the variables evaluated (anxiety and surgical fears). | Use of therapeutic listening in anxiety and surgical fears as a nursing intervention in patients in preoperative colorectal cancer. |
| Handan et al., 2018 | Intraoperative (Obstetrics) | Experimental Study | Music therapy reduced physiological and cognitive anxiety responses in patients submitted to multiple cesarean sections and can be used in clinical practice. | Songs chosen by the patients were played during the cesarean section for the experimental group. No music for control group. |
Discussion
The data showed that among the operative stages, the period preceding the surgeries is the one with the greatest investment in research. This stage includes: pre-operative visits and guidance resources with educational focuses (in the interface to promote anxiety reduction), as interventions with greater choice and positive results in the proposal to manage stressful demands of the patient undergoing surgical treatment. In the other stages (intra-operative and post-operative), it was observed that alternative therapies, such as music therapy, aromatherapy and therapeutic massage, can be important elements as interventional and impactful tools in the process of physical and emotional response that converge to a point of recovery from surgery in a more balanced way.
It is noteworthy that randomized clinical trials (RCTs) are considered quality scientific methods because they allow a better design between causality and the effectiveness of an intervention (Pedrolo et al., 2016). Furthermore, the RCTs are designed to definitively answer a specific question, focusing strictly on a research hypothesis, isolating the effect of one or a small number of therapies (Oliveira et al., 2015). Descriptive research, in turn, is defended as important for science, because description is usually the first and essential step to move towards the understanding of the phenomenon (Volpato, 2015).
In contrast to these methods, a study on stressors and hemodynamic instability in the postoperative period mention about the importance of longitudinal studies, with an investigative focus on the effectiveness of the implementation of care protocols, aimed at preparing the patient for the anesthetic-surgical procedure, with the greater objective of reducing exposure to stressors (Dessotte et al., 2018). There are many studies in different areas of nursing that emerge demands for the construction of new knowledge that represent, for professional practice, an abstraction to be materialized in technology corresponding to the characteristics and peculiarities of nursing practices in certain situations. Among these studies, the following stand out: general (Bahrami et al., 2013; Coppetti et al., 2015; Costa & Sampaio, 2015; Garcia et al., 2018; Gürsoy et al., 2016; Ko & Lin, 2012; Rojas & Azevedo, 2013), vascular (Hudson et al., 2015; Jiménez et al., 2013), orthopedic (Lim et al., 2014), ophthalmological (Nazari et al., 2012), obstetric (Handan et al., 2018; Saatsaz et al., 2016), and cardiac (Bikmoradi et al., 2015; Bittar et al., 2012; Fazlollahpour-Rokni et al., 2019; Hosseini et al., 2016).
This reflexive construct redirects attention to studies in the cardiac surgical area (Bikmoradi et al., 2015; Bittar et al., 2012; Fazlollahpour-Rokni et al., 2019; Hosseini et al., 2016) and its particularities focused on the many physiological, psychological and emotional consequences due to stress (Parvan et al., 2012).The complex, threatening and enforcer character of organic stress of this type of surgery was linked to the "fear of dying" and this configured a more cited category as stressors perceived by the cardiac patient; perhaps by the perception of the heart as a vital organ (Esplendori et al., 2018). Therefore, identifying and understanding the nature of stress can help nurses control and reduce it (Parvan et al., 2012). Furthermore, it is worth highlighting strategies for discussions and training of the nursing team as a contribution to improving care for cardiac surgery patients (Felippe et al., 2013).
The scenario related to the nurse's role in the care of surgical patients and in the perspective of stress management, it is likely to be associated with the fact that in this surgical stage, the possible changes of the patient are investigated, in order to reduce the surgical risks and the moment when the patient is more vulnerable in his/her physical-emotional needs; therefore, more prone to emotional imbalance (Ascari et al., 2013). Considering the intraoperative period was reached only in three interventions, it is suggested that the type of anesthesia in these procedures, where the patient can occasionally be adept, may contribute to interventions to control stress and anxiety, especially by the presence of the anesthesiologist nurse along the lines of the American surgical team (Curi & Peniche, 2004). In this sense, the nursing intervention during surgeries is highlighted as a contributing factor in the significant improvement of patients' experience, since the higher the level of anxiety, the worse the post-surgical results (Hudson et al., 2015).
The postoperative moment was visualized only in American studies (Bikmoradi et al., 2015; Lim et al., 2014; Saatsaz et al., 2016) in three different specialties: orthopedics (Lim et al., 2014), cardiac (Bikmoradi et al., 2015) and obstetric (Saatsaz et al., 2016). This evidence refers to the study (Silva et al., 2018) on postoperative discomforts, which is attentive to the stress factor, as an influencing element in the performance of surgery and recovery of surgical patients. Thus, stress management is explained as a factor of improvement in the quality of nursing care in surgical procedures (Gürsoy et al., 2016), in view of the view that this syndrome can leave patients more susceptible to infections and complications (Good et al., 2013).
Although the research problem in the present study is stress, in 14 studies (82%) interventions aimed at the phenomenon of anxiety emerged. This phenomenon is argued as an unquestionable event in surgical interventions at both psychological and physiological levels (Costa & Sampaio, 2015); it is now presented as coming from stressful situations (Bagheri et al., 2016); now as a stress-inducing trigger (Barell et al., 2018); and also approached as a nursing diagnosis and interpreted from the stress-related factor angle (Gonçalves & Medeiros, 2016). Research dealing with preoperative anxiety in anesthetic procedures mentions the existence of different types of anxiety disorders (panic, generalized anxiety disorders, mixed anxiety depressive disorders). However, in this study it is considered that the anxiety generated in the patient by the anesthetic-surgical act is a psychic and physical discomfort that arises from the sensation of immediate danger and is characterized by a diffuse fear, which can go from restlessness to panic, which in many cases can arise at least one week before the procedure (Rojasu & Azevedo, 2013).
In the scope of nursing interventions, Brazilian studies and the Spanish study worked "educational intervention (Bittar et al., 2012; Coppetti et al., 2015; Costa & Sampaio, 2015; Rojas & Azevedo, 2013) and preoperative nursing visits (Bittar et al., 2012; Garcia et al., 2018) as a form of stress management and anxiety in surgical patients. The American studies presented a diversity of interventions: music therapy (Handan et al., 2018; Jiménez-Jiménez et al., 2013), therapeutic massage (Nazari et al., 2012; Saatsaz et al., 2016), aromatherapy (Bikmoradi et al., 2015; Fazlollahpour-Rokni et al., 2019; Hosseini et al., 2016), preoperative visit (Gürsoy et al., 2016) and relaxation techniques (Bahrami et al., 2013; Hudson et al., 2015; Ko & Lin, 2012; Lim et al., 2014).
To better understand these interventions, the results of the articles included in this integrative review were gathered in two thematic categories, namely: Educational intervention in the management of stress and anxiety in surgical patients and non-pharmacological interventional practices as an alternative to nursing care. These categories will be discussed individually below.
Educational interventions in the management of stress and anxiety
The experience of surgery generates stress and anxiety to the patient and his/her family, due to fear of the unknown and doubts and inaccuracies regarding the recovery process (Bittar et al., 2012). Among the actions that can be developed in the search for complete understanding of surgery and physical and psychological preparation for surgical intervention, we highlight the orientations regarding the surgical procedure and anesthesia (Coppetti et al., 2015). The nursing guidelines and their efficacy in reducing the level of anxiety in preoperative patients were studied (Costa & Sampaio, 2015), with the identification of the disease, to greater significance, in patients who did not receive the guidance. In this perspective, researchers (Gürsoy et al., 2016) confirm that the preoperative education provided by nurses contributes to increased patient self-care skills and compliance; and therein lies the help in reducing anxiety.
For American researchers, the practice of education, through educational material, contributes not only to the easing of anxiety, but also to depression, levels of surgical pain and a better recovery of the patient. However, for an efficient intervention, it is necessary that the material is easily accessible, with language appropriate to the target audience, and that allows consultation during the perioperative stages (Paiva et al., 2017).
The preoperative nursing visit was an intervention performed in two studies (Bittar et al., 2012; Gürsoy et al., 2016), being characterized as an important moment for guidance and preparation of the patient for the surgical experience with less stress and anxiety. This type of intervention is relevant, since it implies the qualification of the communication and trust process between nurse and patient, as well as helps in accepting and improving coping with the situation (Coppetti et al., 2015).
The patient's perspective on the subject was investigated in light of educational practice and its importance. It was found that this type of intervention provides benefits in relieving anxiety, reducing pain, speeding recovery and increasing self-esteem (Perrando et al., 2011). Therefore, it is recommended to maintain educational interventions for surgical clients in order to prevent the repercussions of the health-disease process, associated with situations of stress, fear, anxiety and other problems that alter health and biopsychosocial integrity (Rojas & Azevedo, 2013).
From the only study in Spanish (Rojas & Azevedo, 2013), the command emerges that there are several strategies for the use of nursing professionals in the treatment of situations of stress and anxiety to the patient who will undergo a surgical intervention, although health education is the most used and should have as its axis, support and teaching actions to promote tolerance to surgical stressors and prevent pre- and postoperative complications. However, other authors recall that it is necessary to know the patient's schooling, so that the nursing team can share information and guidance and facilitate understanding by patients (Felippe et al., 2013).
Non-pharmacological interventions for the management of stress and anxiety
Stress and anxiety and its psychological and physiological reactions are common disorders in surgical patients, which can trigger impairments in the process of surgery and recovery, thus fitting adequate management (Nazari et al., 2012). Among the clinical practices that can benefit nursing science as part of the care of patients in perioperative surgery, there is the offer of relaxation intervention in the control of physical pain and emotional tension (Lim et al., 2014) and therapeutic listening in the person-centered approach (Garcia et al., 2018) in assisting with sensitivity and availability for dialogue and listening, in relation to the needs and doubts that patients present (Felippe et al., 2013).
Regarding relaxation interventions, it is cited as feasible, easy to learn and practice because it does not require special facilities or equipment; checking a low-cost tool that nursing can use in the management of stressor factors, such as postoperative pain and anxiety; as well as being aggregated to institutional policies in the area of routine care (Lim et al., 2014).
Still under interventional investigation, alternative intraoperative distraction therapies (DVD, music, distraction with anti-stress balls) were used during minimally invasive venous surgery under local anesthesia (Hudson et al., 2015). This approach refers to the evidence of another study (Jiménez-Jiménez et al., 2013) that correlates intraoperative anxiety with a higher incidence of postoperative pain and thus, interactive nursing measures during surgery may favor not only distraction and patient care, but also to significantly reduce anxiety and pain (Hudson et al., 2015).
A study was also found that tested psychological and physiological indices in the performance of hand massage before surgery with local anesthesia, as a way to reduce anxiety and provide comfort to the patient (Nazari et al., 2012). The same therapeutic approach was applied to primiparous women submitted to elective cesarean section, including foot massage, to determine the effect of this intervention on pain and post-cesarean anxiety (Saatsaz et al., 2016). Both studies corroborated the elucidation of beneficial results of therapeutic massage and the recommendation to be performed this type of intervention in patients to reduce pain and anxiety.
In an approach implemented in the context of nursing care, during varicose veins surgery, music therapy was the intervention of choice, as a safe procedure that has been proven to reduce the anxiety and stress of patients (Jiménez-Jiménez et al., 2013). This proof is explained by a study in biopsy surgeries, which describe music as a factor capable of positively affecting the state of anxiety and pain, triggering a neuroendocrine effect, caused by invasive procedures and thus, this therapeutic modality is suggestive of being used by nurses in the recovery of patients (Song et al., 2018).
In relation to other non-pharmacological therapeutic modalities, it was evidenced that the nurse resorted to tests with "aromatherapy", configured to surgical patients, in a potential state of stress and anxiety. Aromatherapy for stress is defended as a great holistic alternative and scientific art of body, mental and emotional health promotion (Sacco et al., 2015). This form of intervention was contemplated in studies that used lavender (Bikmoradi et al., 2015; Hosseini et al., 2016) and pink (Fazlollahpour-Rokni et al., 2019) essences; of these, only one showed the positive effect of aromatherapy (lavender essence) on the level of anxiety and cortisol (Hosseini et al., 2016). Thus, it is suggestive as a strategy to be adopted as a complementary branch of care in multiple areas, including nursing.
Regarding aromatherapy being effective in one study and not in another, researchers highlight that this event can be associated with the type of surgery and the method of comparison applied (Hosseini et al., 2016). There were few studies on the studied theme, especially in Brazil and Spain. This data contrasts with the consensus that attention to surgical patients in stress management by nursing is necessary; the peculiarities of the complex scenario of the perioperative period.
It is estimated that alternative therapeutic multimodalities found in American studies (music, aromatherapy, massages and other relaxation practices) may be associated with the reality of a perioperative team in that region, which has an anesthesiologist nurse, and thus, attention to surgical patients is likely to be better managed. However, regardless of this professional in the Brazilian reality, the issues of anxiety, pain, fear, lack of knowledge of the treatment process and other stressors that make up surgical treatment, place the nurse ethically responsible for searching for alternative indicators for intervention in general, even than under the educational focus. If he cannot perform the care, he can teach the patient how to do it, as is the case with relaxation strategies; and for this he must train himself.
It was understood that waiting for surgery, fear of the procedure, unknown situations, death, anesthesia, among other fears highlighted in the literature, give the operative moments and the surgical environment a profile of "risk factors" for stress in the clientele under treatment. They represent broad stressors and as such, scientifically capable of interfering in organic homeostasis and therefore in a more effective recovery.
It was concluded that the experiences of the studies that worked interventions, had successful results in alleviating the situation of stress and anxiety in surgical patients and, thus, are suggestive of contributing to the management of the phenomenon in order to qualify care assistance. Thus, it is considered that diagnoses made to understand stress situations and strategic planning with actions customized to this type of patient can configure an important space, to be occupied by the nurse, in the aspect of expanded holistic care. The performance of studies using phenomenology with a view to allowing a more holistic approach in the pre, intra and post-surgical phases under a "staggered" look at levels and phases of stress of the surgical patient, can mean a differential in the presentation of new facets of the phenomenon and intervention priorities.
It is also recommended to conduct intervention studies based on the implementation of measures aimed at stress control and that contribute to evaluate strategies that have proved effective in this context. In this context, the development of comparative studies between different treatment sectors (surgical clinic, surgical center, and other sectors of specialized hospitalization, such as ICU, hemodynamics, pediatrics, etc.), may represent a relevant method in helping nursing managers, in order to share both successful experiences to minimize stress, as well as those that have not achieved results in certain scenarios of practice. The limitations of this study lie in the exclusions of studies with outpatient and pediatric surgical patients, which are presumed to be important sources of nursing action.

