










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkMotricidade
versão impressa ISSN 1646-107X
Motri. vol.13 supl.1 Ribeira de Pena dez. 2017
ORIGINAL ARTICLE
Lipid profile and associated factors in schoolchildren
Ana Paula de Oliveira Azambuja1,*
1 Paulista State University, Bauru, Brasil.
ABSTRACT
The relationship between anthropometric measurements and lifestyle habits of schoolchildren with lipid profile is assessed by a descriptive, cross-sectional study on a sample of 135 school children aged between 6 and 10 years. Variables comprised body mass index, waist circumference, blood pressure, questionnaires on physical activity, dietary habits and metabolic changes. Analysis compares rates by Mann-Whitney test and associations by chi-square test, while effects were measured by odds ratio at 5% significance (p <0.05). There was no significant association between nutritional status and lipid profile. Lipid changes occurred inclusively in children with normal weight. Physical activity was inversely associated with dyslipidemia and suggests that physical activities associated with eating habits may be a preventive mechanism on cardiovascular disease risk factors.
Keywords: dyslipidemia, obesity, food habits, children.
INTRODUCTION
The distribution of body fat (BF) is positively related to Cardiovascular Diseases (CVD) whose combination may be obtained by anthropometric parameters, such as body circumferences, with easy applicability and high accuracy degree (Burke et al. 2008). Dyslipidemias are associated to BF distribution, with unfavorable nutritional conditions, characterized by abnormal concentrations of lipids or lipoproteins in the blood, and determined by genetic and environmental factors (Burke et al. 2008; Franca, Alves, & Hutz, 2004), In fact, they are defined as a categorical factor for CVD development (Kruger & Ribas-Silva, 2014).
Co-relationships in several populations are well established between risks of coronary arterial disease (CAD) and high blood concentrations of total cholesterol (TC), especially low-density lipoproteins (LDL-c), and reduced high density lipoproteins (HDL-c) (Franca, Alves, & Hutz, 2004; Lanti, Puddu, & Kromhout, 2000; Webber, Srinivasan, Mattigney, & Berenson, 1991).
Children´s lipid profile in investigated to detect possible high lipid rates and early intervention to ward off physiological changes that may occur during the teenager period (Françoso & Coates, 2002).
According to studies on Brazilian populations, dyslipidemias have 10% - 35% prevalence in children and adolescents, depending on region and criteria (Simão, Précoma, Andrade, Correa Filho, & Saraiva 2014). Epidemiological studies on children´s and adolescents´ lipid profile suggest that cholesterol level in childhood is a predictor factor for cholesterol levels in adulthood (Gama, Carvalho, & Miranda, 2007; Leite et al., 2009).
Inadequate feeding habits during childhood are at the basis of lipid alterations in the life phase. They are actually related to food rich in fat and sugar, coupled to lack of physical activities and mistaken family habits which directly affect lipid profile (Leite et al., 2009; Rechenchosky et al. 2009).
Current paper assesses associations between anthropometric indexes and life style (physical activity and food) to school children´s lipid profile.
METHOD
Current descriptive study with a transversal design evaluates the prevalence of weight access and lipid profile associated with physical activities and food intake of primary schoolchildren in the municipality of Cruzeiro do Oeste PR Brazil.
ParticipantsSample size featured a population of 1224 children (N), a tolerated absolute error of sample of 7% (ε = 0.07), 90% confidence interval (error α = 0.10; Zα/2 = 1.64) and an estimated prevalence of 50%, recommended by Luiz and Magnanini (2006) when study contains several variables or when researcher fails to attribute any rate. Since there was a possibility of several schoolchildren being absent for the biochemical tests, 150 children out of those who participated in the project´s first phase were selected (anthropometric evaluations). One hundred and thirty-five schoolchildren, males and females, aged between 6 and 10 years, participated in the second phase (lipid profile assessment)
Inclusion criteria for participation comprised enrolment in the schools selected for the second phase; participation in the project´s first phase; selection for the new phase; parents´ authorization. Exclusion criteria comprised incomplete or absence of data on any information, especially blood collection and analysis; non-compliance with procedures recommended for collection (for instance, an 8 – 12-h fast).
Instruments and ProceduresVariables included weight by scale (Filizola; 0.1 kg precision) and height by stadiometer SECA (Bodymeter 206) to calculate Body Mass Index (BMI) and employed for the classification of the nutritional state, following criteria by Cole et al. (2007). Waist Circumference (WC) was calculated by non-elastic band (0.1 cm precision) and rates were classified following Férnandez et al. (2004). Systolic (SAP) and diastolic (DAP) arterial pressure were measured and classified according to the criteria by V Brazilian Guidelines for Arterial Hypertension.
Blood lipid components in current assay comprised total cholesterol (mg/dL), HDL-cholesterol (mg/dL), LDL-cholesterol (mg/dL), triglycerides (mg/dL) and glycaemia (mg/dL). Reference rates for the first four blood lipid components were recommended by I Guidelines for the Prevention of Atherosclerosis in Childhood and Adolescence of the Brazilian Society of Cardiology (Giuliano et al. 2005). In 2004, the American Diabetes Association recommended lowering from 110 mg/dL to 100 mg/dL for fasting glycaemia.
The project was forwarded to the Committee for Ethics involving Humans of the Institution (n. 556/2009). Data were collected in 2010 after explaining to participants the details on the research work and after obtaining the parents´ or tutors´ consent.
Statistical analysisKolmogorov-Smirnov test verified normality of data. According to results, non-parametric statistics (mean/minimum and maximum) and analysis of variables were applied. Mann-Whitney´s test compared mean rates and χ² was employed to associate nutritional state and lipid profile. Odds ratio (OR) was employed for effect measurement. Further, 5% significance was adopted (p<0.05). Data were analyzed with Statistical Package for the Social Science (SPSS) 17.0.
RESULTS
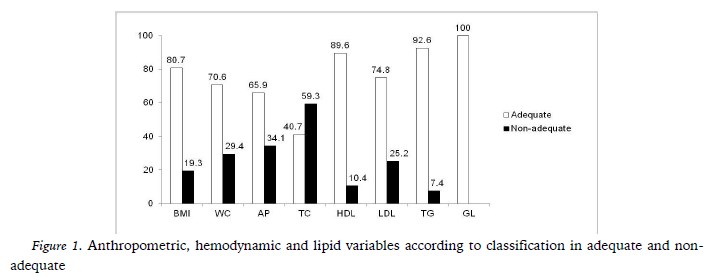
Schoolchildren comprised 50.4% (n=68) males and 49.6% (n=67) females. Mean rates of variables did not differ between the genders. Since anthropometric, hemodynamic and blood lipids variables of the sample showed homogeneity between genders, they were analyzed together.
Figure 1 shows that variable TC had the highest change percentage (59.3%), with no children featuring changes in glycaemia levels.
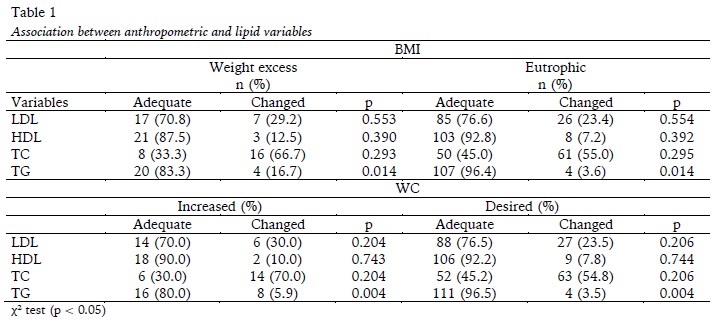
Lipid variables LDL-c, HDL-c and TC were not associated with BMI (Table 1), except for variable TG (p=0.014), similar to variable WC with significant association only for TG (p=0.004).
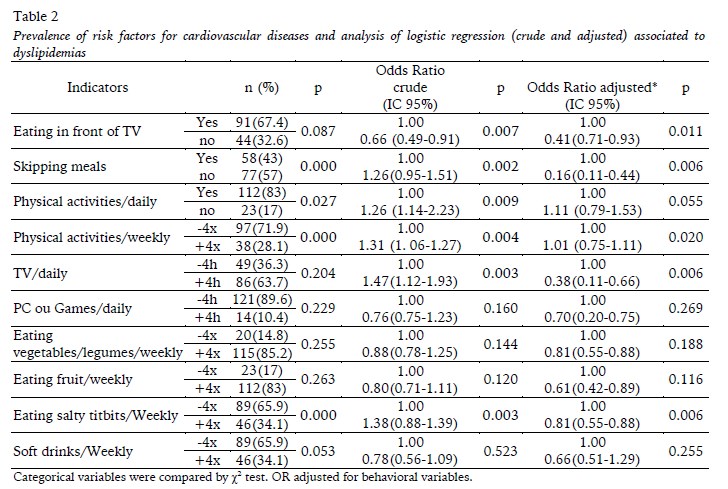
Table 2 demonstrates significant associations between results and variables in crude and adjusted analyses: eating while watching TV, time spent watching TV, time before computer or playing games, eating vegetables and legumes, eating fruit and drinking soft drinks. Skipping meals was reported for 43% of children and the habit of eating packet tit-bits was registered four times a week for 34.1% of the children. Both are associated with dyslipidemia (p=0.000). Refraining from daily physical activities or the practice of physical activities at least four times a week was reported by respectively 83% and 71.9% of schoolchildren, a habit highly combined to dyslipidemia, (p=0.027) and (p=0.000) respectively.
Children who skipped meals had a 1.26 probability of having dyslipidemia than those without this habit, whilst children with the habit of eating tit-bits had a 1.38 more chance for acquiring dyslipidemia than those who do not.
The association between the practice of PAs and dyslipidemia indicated that children who failed to practice daily PAs had 1.26 (IC95%: 1.14-2.23) and 1.31 (IC95%: 1.01-1.67) more probability of acquiring the disease than those who practiced PAs weekly or four times a week.
DISCUSSION
Results revealed that 19.3% of schoolchildren were overweight, corroborating rates given by Casey et al. (2012) in France (19.7%) but lower (25.4%) than those by Rechenchosky et al. (2009) in a survey in a different municipality in the state of Paraná, Brazil. A study in Rio de Janeiro with 5 – 9-year-old children showed 68.4% of children with some type of change in their lipid profile (Savva et al., 2000), whereas Turkish children had high lipid rates, albeit lower than those mentioned above. The author reported that 42% of children and adolescents had changes in their lipid profile (Atabek, Pirgon, & Kurtoglu, 2006). In current study, schoolchildren who did not have simultaneous changes in their anthropometric, hemodynamic and lipid profile amounted to 34.8%, whilst 32.6% showed at least one change. A study with Chilean schoolchildren from 20 schools in 2015 revealed that 32% had at least one alteration in their lipid profile (Barja et al., 2015).
Results on the lipid profile enhance the fact that 59.3% of schoolchildren revealed high TC rates for their age. Forti et al. (1996) showed that 57.7% of children and adolescents had altered TC, with proven family links. Result are highly relevant since longitudinal studies such as those by Menotti et al. (2000) have shown a relationship between TC rates diagnosed in childhood with rates during adulthood.
Eutrophic lipid alterations among schoolchildren in current analysis demonstrated 20.2% hypercholesterolemia and indicated the need to evaluate lipid profile during early childhood, even though the study has not provided any significant rates between BMI and lipid alterations. As shown by several studies, overweight is a categorical factor. Kruger and Ribas-Silva (2014) insist that feeding reeducation and physical activities should be practices in the school milieu so that obesity and associated diseases, such as dyslipidemias, would be prevented.
The percentage of children with altered LDL-c was higher than the rates provided by Rechenchosky et al. (2009) in a study with same age schoolchildren in Maringá PR Brazil. The authors reported altered LDL-c levels in 12.3% of samples, contrastingly to 25.2% in current study.
Lower HDL-c concentrations occurred in 10.4% of schoolchildren analyzed. Rates are actually lower than those in a research with children and adolescents in the city of São Paulo, with rates at 13.5% of children between 2 and 12 years old and at 14.2% of adolescents with a family history of early CVD (Savva et al., 2000). Several studies show that lower HDL-c concentrations accelerate the onset and development of atherogenesis. Lower HDL-c rates are frequently due to heredity, to other atherogenic lipoproteins and obesity, as several studies have shown (Leite et al., 2009; Savva et al., 2000). HDL-c reduction with an increase in LDL-c and serum TG levels increases twenty-fold the development of coronary diseases in adults (Gama, Carvalho, & Miranda, 2007).
The same authors reported TG alterations in 10.4% of children. Rechenchosky et al. (2009) registered alterations in 10% and current study in 7.4% of children. High LDL-c in adults may bring about the onset of CVDs. In the case of TG, more than 7% had higher rates than desired for their age, even though data were lower than those reported by other authors who registered high TG in 14% of children and adolescents with a family history of early CVDs in studies at INCOR, São Paulo, Brazil. A hypothesis was raised that several lipoproteins rich in TG may be involved regardless of the development of atherosclerosis (Webber et al., 1991).
Studies by Savva et al. (2000) with samples of 10 – 14-year old Cypriot children showed that WC is the best predictor for CVDs when compared to BMI. In fact, children with altered WC had higher TC, LDL-C and TG rates. Results in current study demonstrated a significant association between high WC and altered TG.
Dyslipidemia in current research reached 65.9% of children. Dyslipidemias in eutrophic children suggest the influence of other risk factors (but not obesity) on lipid conditions (Savva et al., 2000). Forti et al. (1996) emphasize that dyslipidemias in children and adolescents worldwide is related to inadequate individual or family feeding habits, such as deficient PAs (Cassey et al. 2012).
TV watching for more than 4 hours daily is a habit practiced by 63.7% of schoolchildren, but was not associated with dyslipidemia in current study. However, a 2006 study in Taiwan insisted on the importance of reducing time spent watching TV and of increasing PAs to prevent metabolic syndrome (Li, Leec, & Tsenga, 2007). Time spent watching TV was positively associated with significantly greater chances of high triglyceride levels and fast glycaemia. The authors state that previous analyses suggested that TV watching increases food intake due to the habit of eating while watching TV.
Li et al. (2007) showed that obesity and PAs significantly determine dyslipidemia. In fact, current study shows that lack of daily PAs or PAs at least four times a week is associated with dyslipidemia.
Fernandes et al. (2009) suggest a positive PAs influence during childhood and adolescence on dyslipidemia in adulthood and may be attributed to the chronic effect of PAs throughout one´s life. The above evidences the need for stimulating the regular practice of activities during childhood and adolescence.
Sedentary lifestyle triggers the onset of obesity, arterial hypertension, low HDL-c concentrations and increase in TG, well known for their association with atherosclerosis. Further, lack of PAs in childhood is also prolonged into adulthood (Leite et al., 2009).
According to Françoso and Coates (2002), cardiovascular risk factors should be controlled in childhood and adolescence for CVD prevention through enhancement of cardiovascular health by preventing and controlling obesity, regular practice of physical exercises, control of arterial pressure and particularly healthy feeding habits.
Forti et al. (1996) associated dyslipidemias in children and adolescence related to feeding habits and inadequate individual and familial habits, such as insufficient PAs, similar to current analysis associating the habit of skipping meals, lack of daily PAs and PAs at least four times a week plus and eating tit-bits more than four times a week. PAs has been inversely associated with dyslipidemia and suggests that PAs may be a preventive mechanism on CVDs risk factors.
It must be underscored that current study had its limitations since it failed to establish a co-relationship between data on family history. However, it is relevant with regard to data in southern Brazil due to lack of investigation focused on hinterland towns with small populations.
The systematic analysis of data on the efficaciousness of interventions to enhance PAs and health with the children´s and adolescents´ age bracket revealed better results when there is an association of school activities that involve the family and/or the community to change food intake habits for a better health behavior, including the habit of PAs (Menotti et al., 2000; Rechenchosky et al., 2009).
CONCLUSION
Changes in anthropometric, hemodynamic and lipid variables recur in schoolchildren. Since lipid alterations are present even in children with adequate weight, the control of obesity, guidelines for eating habits and PAs should start during childhood.
PT teachers are better prepared to cope with the process and they should be alert to identify and intervene early on risk factors. These teachers are health professionals that should act directly and continually with schoolchildren and thus contribute towards education and health programs in the schools through adequate eating habits and healthy lifestyles, especially increase in PAs, and thus decrease VCD risk factors in Brazil. Consequently, PE should be underscored as a necessary contribution for schoolchildren´s health, by means of discussions and the formation of a critical conscience so that they would adopt individual actions for the onset of collective benefits.
REFERENCES
American Diabetes Association (2005). Diagnosis and classification of diabetes mellitus. Diabetes Care, 28(Suppl), S37-S42. http://dx.doi:10.1038/ijo.2012.10 [ Links ]
Atabek, M.E., Pirgon, O., & Kurtoglu, S. (2006). Prevalence of metabolic syndrome in obese Turkish children and adolescents. Diabetes Research and Clinical Practice, 72(3), 315-321. [ Links ]
Barja Yáñez, S., Gómez, P. A., Del Pino, L. V., Landa, A. D., Valenzuela, O. C., Jofre, M. F., & Santander, F. M. (2015). Dislipidemias em escolares chilenos: prevalência y factores asociados. Nutrición Hospitalaria, 31(5), 2079-2087. doi: 10.3305/nh.2015.31.5.8672
Burke, G. L., Bertoni, A. G., Shea, S., Tracy, R., Watson, K.E., Blumenthal, R.S., , & Carnethon, M. R. (2008). The impact of obesity on cardiovascular disease risk factors and subclinical vascular disease. Archives of Internal Medicine, 168(9), 928-35. doi: 10.1001/archinte.168.9.928 [ Links ]
Casey, R., Chaix, B., Weber, C., Schweitzer, B., Charreire, H., ., & Simon, C. (2012). Spatial accessibility to physical activity facilities and to food outlets and overweight in French youth. International Journal of Obesity, 36(7), 914-919. [ Links ]
Cole, T. J., Bellizzi, M. C., Flegal, K. M., & Dietz, W. H. (2000) Establishing a standard definition for child overweight and obesity worldwide: international survey. British Medical Journal, 320, 1240-3. [ Links ]
Fernandes, R. A., Sponton, C. H. G., & Zanesco, A. (2009). Atividade Física na Infância e na Adolescência Promove Efeitos Benéficos na Saúde de Adultos. Revista SOCERJ, 22(6), 365-372. [ Links ]
Fernández, J. R., Redden, D. T., Petrobelli, A., & Allisson, D. B. (2004) Waist circumference percentiles in nationally representative samples of African-American, European-American, and Mexican-American, children and adolescents. Journal of Pediatrics, 145(4), 439-444. doi: 10.1016/j.jpeds.2004.06.044 [ Links ]
Forti, N., Giannini, D., Diament, J., Issa, J., Fukushima, J., Bó, C. D., & Barretto, A. C. P. (1996). Fatores de risco para doença arterial coronariana em crianças e adolescentes filhos de coronariopatas jovens. Arquivo Brasileiro de Cardiologia, 66, 119-23. [ Links ]
Franca, E., Alves, J. G. B., & Hutz, M. H. (2004). Apolipoprotein and polymorphism and its association with serum lipid levels in Brazilian children. Human Biology, 76(2), 267-275. [ Links ]
Françoso, L. A., & Coates, V. (2002). Evidências anatomopatológicas do início da aterosclerose da infância e adolescência. Arquivo Brasileiro de Cardiologia, 78(1), 131-136. [ Links ]
Gama, S. R., Carvalho, M. S., & Miranda, C. R. M. (2007). Prevalência em crianças de fatores de risco para as doenças cardiovasculares. Caderno de Saúde Pública, 23, 2239-45. doi:10.1590/S0102-311X2007000900032 [ Links ]
Giuliano, I. C. B., Carameli, B., Pellanda, L., Duncan, B., Mattos, S., & Fonseca, F. H. (2005). I Diretriz de Prevenção da Aterosclerose na Infância e na Adolescência. Arquivo Brasileiro de Cardiologia, 85(Suppl. VI), S1-36. [ Links ]
Kruger, G. R. O., & Ribas-Silva, R. C. (2014). Perfil lipídico e índice de massa corporal de escolares de um colégio estadual da região centro-ocidental do Paraná. Revista Adolescência e Saúde, 11(4), 54-60. [ Links ]
Leite, N., Cieslak, F., Milano, G. E., Góes, S. M., Lopes, M. F. A., Bento, P. C. B., Prestes, A. L. C., & Randominski, R. B. (2009). Associação entre o perfil lipídico e medidas antropométricas indicadoras de adiposidade em adolescentes. Revista Brasileira de Cineantropometria e Desempenho Humano, 11(2), 127-133. [ Links ]
Li, J. D., Leec, S. J., & Tsenga, R. F. (2007). Associations between the metabolic syndrome and its components, watching television and physical activity. Public Health, 121, 83–91. [ Links ]
Luiz, R. R., & Magnanini, M. M. F. (2006). O tamanho da amostra em investigações epidemiológicas. In: Medronho, R. A., Carvalho, D. M., Bloch, K. V., Luiz, R. R., & Werneck, G. L. (Eds.), Epidemiologia. São Paulo: Atheneu. [ Links ]
Menotti, A., Lanti, M., Puddu, P. E., Kromhout, D. (2000). Coronary heart disease incidence in northern and southern European population: a reanalysis of seven countries study for a European coronary risk chart. Heart, 84(3), 238-44. http://dx.doi:10.1136/heart.84.3.238 [ Links ]
Rechenchosky, L., Netto-Oliveira, E. R., Oliveira, M. R. N., Günther, L. S. A., Oliveira Filho, A., Oliveira, A. A. B. (2009). Estado nutricional e perfil lipídico de crianças. Revista da Educação Física, 20(3), 431-440. doi:10.4025/reveducfis.v20i3.5323 [ Links ]
Savva, S. C., Tornaritis, M., Savva, M. E., Kourides, Y., Panagi, A., Silikiotou, N., Georgiou, C., Kafatos, A. (2000). Waist circumference and waist-to-height ratio are better predictors of cardiovascular disease risk factors in children than body mass index. International Journal of Obesity and Related Metabolic Disorders, 24(11), 1453-1458. [ Links ]
Simão, A. F., Précoma, D. B., Andrade, J. P., Correa Filho, H., Saraiva, J. F. K. (2014) I Diretriz de Prevenção Cardiovascular da Sociedade Brasileira de Cardiologia. Arquivo Brasileiro de Cardiologia, 2(5), 420-431. [ Links ]
V Diretrizes Brasileiras de Hipertensão Arterial. (2007). Arquivos Brasileiros de Cardiologia, 89(3), e24–e79. https://doi.org/10.1590/S0066-782X2007001500012 [ Links ]
Webber, L. S., Srinivasan, S. R., Mattigney, A., Berenson, G. S. (1991). Tracking of serum lipids and lipoproteins childhood to adulthood: the Bogalusa Heart Study. American Journal of Epidemiology, 133(9), 884-99. [ Links ]
Acknowledgments:
Nothing to declare.
Conflict of interests:
Nothing to declare.
Funding:
Nothing to declare.
* Corresponding author: Paulista State University, Av. Edmundo Carrijo Coube, Vargem Limpa, 17033-360, Bauru, Brazil. Email: ana_paula_3005@yahoo.com.br


{kind=link}
{kind=link}
{kind=link}