











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Engaging in physical activity (PA) has great health benefits; these are well established and include, among others, a lower risk of cardiovascular disease, hypertension, diabetes, and breast and colon cancer (Kumar et al., 2015). Additionally, PA has positive effects on mental health, delays on the onset of dementia, and can help to maintain a healthy weight (Hallal et al., 2012). Despite this, a large percentage of children's remains physically inactive. To quantify the effect of physical inactivity on the world's major non-communicable diseases, we estimated how many of these diseases could be avoided in the population if inactive people were to become more active (Lee et al., 2012). Current recommendations are for preadolescent children to accumulate at least 60 minutes daily of moderate to vigorous PA (Oja & Titze, 2011).
School physical education (PE) is recognized as the most widely available resource for promoting PA among children and adolescent. However, limited data are available on the intensity and duration of PE classes in elementary schools or on the level of activity afforded children in these classes (Study & Network, 2016). Thus the PE teacher needs more tools to improve the quality of the classes especially in the intensity of the activities (Study & Network, 2016). The educative community must are interested in how PE is conducted, particularly it relates to offering and promoting health-related PA (Mckenzie et al., 1995; Sallis & McKenzie, 1991).
Children's health and well-being are highly correlated with their PA and fitness; recently published studies indicate that low levels of fitness (e.g., cardiorespiratory fitness, increase body fat) are associated with an elevated risk of developing adverse physiological events (e.g., blood pressure, plasma glucose) in school-aged students (Ortega et al., 2008).
High levels of cardiorespiratory fitness (CRF) and PA are associated with a favourable metabolic risk profile. PA and CRF are separately and independently associated with individual and clustered metabolic risk factors in children (Ekelund et al., 2007). Some authors (Trudeau et al., 1998) have shown that children with a higher level of PA, or who have been somehow physically trained during childhood, showed a higher level of PA and CRF in adulthood.
Anthropometric characteristics such as increased abdominal fat accumulation, as well as some lifestyle parameters including the lack of PA and the development of poor dietary habits, are strongly and accurately associated with poor fitness in childhood and adolescence (Arnaoutis et al., 2018).
One approach that has the potential to address the high prevalence of children's inactive with increased body fat is to enhance the time and intensity of the PE (Lau et al., 2014).
Recently, interest in higher-intensity intermittent training (HIIT) research has increased among researchers. They have provided evidence that HIIT is associated with a significant impact on CRF and body composition, inducing greater health benefits than less intense forms of exercise (Boutcher, 2011). Unlike adults, children's habitual PA patterns are highly intermittent in nature, characterized by rapid changes from rest to vigorous PA (Howe et al., 2010). HIIT activities are of particular importance, and they reinforce the concept that PA guidelines may be needed to emphasize vigorous-intensity exercises to maximize health benefits among children and youth. However, there is a need for more experimental work to confirm the efficacy and safety of HIIT needed to generate health benefits among youth (Carson et al., 2014). The research strives to develop interventions and strategies to increase students’ activities in PE classes from moderate to vigorous (Sallis et al., 2012). They also provided some data about the effect of higher intensity exercises in children and young people, but the collection of more data is still needed, especially in experimental studies in order to increase the amount of evidence about the use of high-intensity exercises in PE classes. This would allow the development of scalable interventions to be implemented in the school system, considering that, nowadays, most of the interventions where HIIT activities are applied are performed in laboratories or health centers and not in schools (Reyes-Amigo, Gómez, Gallardo, & Palmeira, 2017). That is why this research tries to answer the question of whether it is possible to apply the high-intensity intermittent method in PE classes with the aim to provide evidence on the matter in a safe and secure manner, with the least number of restrictions in connection to participants (age, sex, sexual maturity). Considering the aforementioned information, this study is of great relevance since the need to elevate the intensity of PE classes due to their effect on the students’ health is of upmost importance (CDC, 2010).
The effect moderators of interventions with physical exercise differ in their results. The studies that research the moderator on physical fitness are scarce, and single RCTs generally lack the power to investigate the effect of such moderators (Sweegers et al., 2017). There is also significant evidence connected to the analysis of moderators in prepubertal subjects who do not show differences in the adaptations induced by exercise according to the biological maturity and sex (Marta et al., 2014). Therefore, it is important to carry out studies that address this issue.
A study (Bauman et al., 2002) pointed out that a moderator produces different estimates of the association at different levels of a variable. In the case of physical exercise, the moderators are diverse; however, sex and age are common elements in the analysis. These moderators, plus the sexual maturity stage, can influence physical performance (Krombholz, 2006).
Child development – physical, psychological, and mental – is connected to the gradual changes that occur mainly due to the modification in their sexual maturity stage. There are also minor differences connected to sex, however, some findings confirm that physical exercise modifies physical shape variables connected to sex, age, and sexual maturity stage (Malina, 1994).
This study data is part of an investigation that had the aim to assess the effect of an 11-week intervention in a PE class using two different exercise intensities on CRF and body composition in children. The present study was designed to identify the applicability of the intervention in the PE class and its effects regarding sex, sexual maturity stage, and age, as moderators on CRF and body composition.
The first hypothesis is that male students would present a more significant improvement than girls in CRF and body composition. There are studies in which children have better results than girls in variables of fitness related to health (Aires et al., 2011; Carson et al., 2014).
The second hypothesis is that the student's sexual maturity stage Tanner 2 would present greater improvements in the CRF and body composition. No studies were found that would differentiate the effects of intervention between sexual maturity stages in the prepubertal stage. However, the influence of the hormonal changes in body composition may modify the results of the fitness (Ortega et al., 2008).
The third hypothesis is that student's age, 10 years old, would present greater improvements in CRF and body composition. Within a given chronological age group, some children may have an advantage or disadvantage in physical fitness tests due to their maturity status, independent from other factors (Behringer, 2010).
METHOD
Participants
This study is part of an experimental study carried out in a randomized, controlled, pre-post design to evaluate the effects of exercise training in children.
Sixty-six children (23 boys and 43 girls) volunteered to participate. The participants were students recruited through posters, emails, and meetings with parents and teachers from a high-school in Valparaíso, Chile. The students’ age ranged from 9–10 years, with a sexual maturity stage Tanner 1-2 (evaluation supervised by a pediatrician). In order to assess the pubertal development stage of the participants, pictures of Tanner's five stages were used. All participants were requested to self-evaluate their pubertal development showing them pictures of Tanner's stages and asking them to identify which stage they thought they were. This procedure was explained to the subjects by a pediatrician who also supervised all the procedures. In order to respect their privacy and to promote each girl's and boy's comfort level, the classification was carried out individually and independently in a specially assigned room. Each participant was classified in one of Tanner's five stages described for both sexes (Matsudo & Matsudo, 1994).
Parent/guardian consent and child assent were obtained prior to the start of the intervention. Ethical approval was granted for this study by the bioethics committee from Playa Ancha University, Chile (01/2017). The participants selected were not part of any regular exercise-training program. Volunteers were excluded if they presented any type of chronic pediatric disease, cardiovascular or metabolic disease (except for obesity), or any orthopedic limitation. Participants whose attendance rate was lower than 95 percent (%), who failed to attend first or second measurement, and/or presented a negative response to training, were also excluded. The final analysis was carried out with 48 participants (32 girls, 16 boys) because 11 children were part of a regular exercise-training program, and 7 presented a form of chronic pediatric disease. All participants completed the study, and there were no negative effects after the interventions.
Children were randomly assigned to two forms of exercise: a) high-intensity intermittent games (HIIG) or b) moderate-intensity games (MIG) using simple randomization procedures. In this case, the study was performed with 2 groups, and the assignation was decided with the toss of a coin. As a result of the randomization process, the HIIG participants were 25 children (7 boys and 18 girls), and the MIG participants were 23 (9 boys and 14 girls). Both of these groups had a different number of participants, and the presence of boys and girls varied since the groups were created from two 4th-year elementary school classes. The students were assigned a type of intervention through the aforementioned procedure.
Measures
Cardiorespiratory fitness test
Twenty meters shuttle run test (20mSRT) was used to estimate CRF. The subjects were required to run between two lines drawn on the floor 20 meters apart while keeping the pace with an audio signal. The initial speed was 8.5 km/h, which was increased by 0.5 km/h per minute (1 min equals one stage). The test was finished when the participant failed to reach the end line concurrent with the audio signals on two consecutive occasions (Castro-Piñero et al., 2010). The formula (Leger et al., 1988) used to obtain the maximum oxygen intake (VO2max) that allowed the identification of CFR was applied in connection to the age and sex of the participants since all of them were in a prepubertal stage.
Body composition
The percentage of body fat (BF%) was obtained from skinfold thickness measured in two places: triceps and subscapular with a Lange Skinfold Caliper adipometer; and Slaughter et al., (1988) formula was used to obtain the data for the prepubertal population of both sexes. The skinfolds sum was obtained with triceps, subscapular, and calf (Castro-Piñero et al., 2010). Height and body mass were measured with a wall stadiometer and a scale (SECA 703). Body mass index (BMI kg/m2) z-score was calculated with the Software AnthroPlus. Waist circumference (WC) was measured in the horizontal plane, midway between the inferior margin of the ribs and the superior border of the iliac crest in deep expiration (measuring tape Lufkin W606P) (Marshall et al., 2004).
Procedures
Details about the procedures, assessment, and intervention are published in a study protocol already published (Reyes-Amigo et al., 2018).
The testing procedures and measurements were completed pre and post-intervention. The children were familiarized with the assessment of CRF – a pilot and test-retest were performed, however, these data were not statistically analyzed – and body composition since it was part of the regular procedures of the regular PE classes.
Intervention
The intervention was published in a study protocol (Reyes-Amigo et al., 2018). However, the most important aspects of the interventions are described next.
A 2-week pilot trial with children (n = 32; mixed ethnicity, aged 8–9 years) from a school different from the one used in this study showed that children could repeatedly perform HIIG and MIG for the time allotted.
Both groups completed the 11-weeks intervention, with 2 sessions per week (17 sessions) of 45 minutes during PE class. These interventions were comprised of the same exercises as the warm-up and in the cold-down. Teachers of PE directed the PE Class.
The HIIG interventions had the objective of maintaining high-intensity activities according to the recommended time for PE class (CDC, 2010). HIIG in the central part of the class is comprised of four games: two relays games and two games of collaboration and opposition in small spaces to a 75-95 % maximum heart rate (HRmax) intensity and 6-8 of ratings of perceived exertion (RPE). Both activities had a duration of 24 minutes; between each game, there was a recovery time of 2 minutes (Baquet et al., 2001; Bendiksen et al., 2014; Seabra et al., 2016).
The MIG intervention was similar to a standard PE class (Bendiksen et al., 2014). MIG in the central part of the class and comprised of four continuous games between 60-74 % HRmax and 4-5 RPE. Duration 20 minutes. Between each game, a recovery of 2 minutes and 40 seconds is in place.
Both interventions were performed in a high school multipurpose court. The intensity was controlled with heart rate (Lambrick et al., 2016) (Cardiac frequency monitor M400 POLAR, Finland) and RPE (Robertson et al., 2005).
Statistical analysis
Multiple regression was used to analyze simple moderation (Bolin, 2014; Hayes & Rockwood, 2017). Macro Process was used for the analysis in the Statistical Package for the Social Sciences (SPSS) program version 23. The multiple regression model 1 analysis allowed to quantify the regression coefficients B1, B2, and B3; through 5000 bootstrap resamples. These established relationships between the independent variables, intervention programs, dependent variables, Delta (Δ) value obtained from the difference between baseline values, and post-intervention values (i.e., post-baseline): CRF, BF%, the skinfolds sum, BMI z-score, and WC; and the moderator variables: sex, Tanner stages, and age. The most significant result of the study was the interaction between the independent and moderator variables (B3). The threshold for significance was set at P < 0.05.
RESULTS
Forty-eight participants completed all the interventions. No adverse events were registered. Children randomized to HIIG and MIG had an average attendance of 94%: 16 of the 17 available sessions.
Table 1 shows the characteristics of the participants at baseline. All variables were not statistically significant between the groups at baseline, except WC. Chi-Square analysis showed no difference in the proportion of boys and girls in the study groups (Chi-Square= 0,414, P >.05), nor were there differences in relation to the maturation (Chi-Square= 0,882, P >.05).
Table 1 Physical characteristics data in mean (± SD) for HIIG and MIG groups in baseline
| OUTCOMES | HIIG (n=25) | SD | MIG (n=23) | SD | P |
|---|---|---|---|---|---|
| Mean | Mean | ||||
| Age (years) | 9,48 | 0,50 | 9,52 | 0,51 | 0,775 |
| Height (cm) | 138,16 | 6,22 | 138,60 | 6,11 | 0,802 |
| Weight (kg) | 37,89 | 6,99 | 41,21 | 10,04 | 0,235 |
| CRF (VO2max ml *kg−1*min−1) | 44,85 | 3,53 | 44,84 | 3,74 | 0,876 |
| BMI z-score (BMI/E) | 1,20 | 0,73 | 1,65 | 1,03 | 0,093 |
| WC (cm) | 63,62 | 6,67 | 68,22 | 9,73 | 0,049 |
| BF% | 27,67 | 6,24 | 31,77 | 11,47 | 0,212 |
| Skinfolds Sum (mm) | 50,12 | 15,86 | 60,10 | 25,65 | 0,170 |
CRF, Cardiorespiratory fitness; BMI z-score, body mass index z-score; WC, waist circumference; BF%, percentage of body fat
During the 11-week intervention, HIIG presented a significantly higher average heart rate of 153±11 bmp (∼76% HRmax) when compared to the MIG of 129±12 bmp (∼65% HRmax). The maximum heart rate was also significantly higher HIIG (HRpeak of 196±12 bmp; 98% HRmax) when compared to MIG (HRpeak of 184±12 bmp; 92% HRmax).
Effects
Detailed information about the results of the intervention is available elsewhere (Reyes, submitted).
In the analysis of the coefficient B1 in the moderators of sex, stage of sexual maturation, and age, HIIG intervention showed a significantly increased effect on the ΔCRF sex and age. This indicated a greater effect on participants of HIIG intervention compared to MIG (Table 2). Regarding body composition, the HIIG intervention had significant effects on ΔWC sex and age, and Δ skinfolds sum sex and age. The remaining variables failed to show significant effects in the intervention.
Table 2 Regression coefficients of the moderators on ΔCRF, Δ value of BF%, WC, BMI z-score, Skinfolds Sum in the effects of HIIG vs. MIG
| OUTCOMES VARIABLE | MODERATOR VARIABLE | Coefficient B1 Intervention | P | Coefficient B2 Moderator | P | Coefficient B3 Interaction Intervention x Moderator |
P |
|---|---|---|---|---|---|---|---|
| Δ CRF (VO2max ml *kg−1*min−1) | Sex | -2.283 | 0.025 | 0.207 | 0.834 | 0.302 | 0.878 |
| Sexual maturity-Tanner Stage | -1.776 | 0.115 | -1.388 | 0.216 | -1.732 | 0.438 | |
| Age years | -2.208 | 0.022 | 0.164 | 0.860 | 0.830 | 0.658 | |
| Δ BF% | Sex | -1.568 | 0.238 | -.899 | 0.496 | -1.490 | 0.572 |
| Sexual Maturity-Tanner Stage | -1.856 | 0.226 | 1.140 | 0.455 | 0.559 | 0.854 | |
| Age years | -1. 878 | 0.138 | -.682 | 0.586 | -2.073 | 0.409 | |
| Δ WC (cm) | Sex | -2.608 | 0.001 | -1.558 | 0.045 | 0.113 | 0.940 |
| Sexual Maturity-Tanner Stage | -1.374 | 0.121 | 0.447 | 0.609 | -3.549 | 0.047 | |
| Age years | -2.460 | 0.001 | -.428 | 0.569 | 1.176 | 0.434 | |
| Δ BMI z-score | Sex | -.146 | 0.063 | -.050 | 0.511 | -.080 | 0.601 |
| Sexual Maturity-Tanner Stage | -.057 | 0.504 | -.006 | 0.943 | -.331 | 0.059 | |
| Age years | -.131 | 0.065 | 0.094 | 0.181 | 0.274 | 0.054 | |
| Δ Skinfolds Sum (mm) | Sex | -6.267 | 0.044 | -4.017 | 0.191 | -1.662 | 0.785 |
| Sexual Maturity-Tanner Stage | -5.805 | 0.107 | 2.994 | 0.401 | -.811 | 0.909 | |
| Age Years | -6.607 | 0.027 | -2.286 | 0.434 | -5.260 | 0.369 |
Δ, Delta value obtained from the difference between baseline and post-intervention values; CRF, Cardiorespiratory fitness; BMI z-score, body mass index z-score; WC, waist circumference; BF%, percentage of body fat;
B1regression coefficients moderator,
B2regression coefficients intervention,
B3regression coefficients interaction moderator-intervention
Moderators of cardiorespiratory fitness
As shown in Table 2, sex, sexual maturity stage, and age did not moderate the result on ΔCRF. Furthermore, no moderation was observed in the interaction between groups of intervention. Hence, its efficacy does not differ in connection to sex, sexual maturity stage, and age.
Moderators of Body composition
Sex, sexual maturity stage, and age did not moderate the effect of the HIIG intervention on ΔBF%. Also, there was no moderation in the interaction between groups of intervention, thus they do not differ in their efficacy according to sex, sexual maturity stage, and age on ΔBF% (Table 2).
As shown in Table 2, sex moderated the effect on ΔWC. Sex does not moderate the interaction between groups of intervention; they do not differ in their effectiveness according to sex.
Sexual maturity stage and age does not alter the result on ΔWC. Different results were observed in moderation of the interaction between groups of intervention. As Figure 1 shows, MIG has a lower ΔWC compared to HIIG in the participants with a sexual maturity stage in Tanner 2. The participants in the sexual maturity stage Tanner 1 did not show differences between the groups.
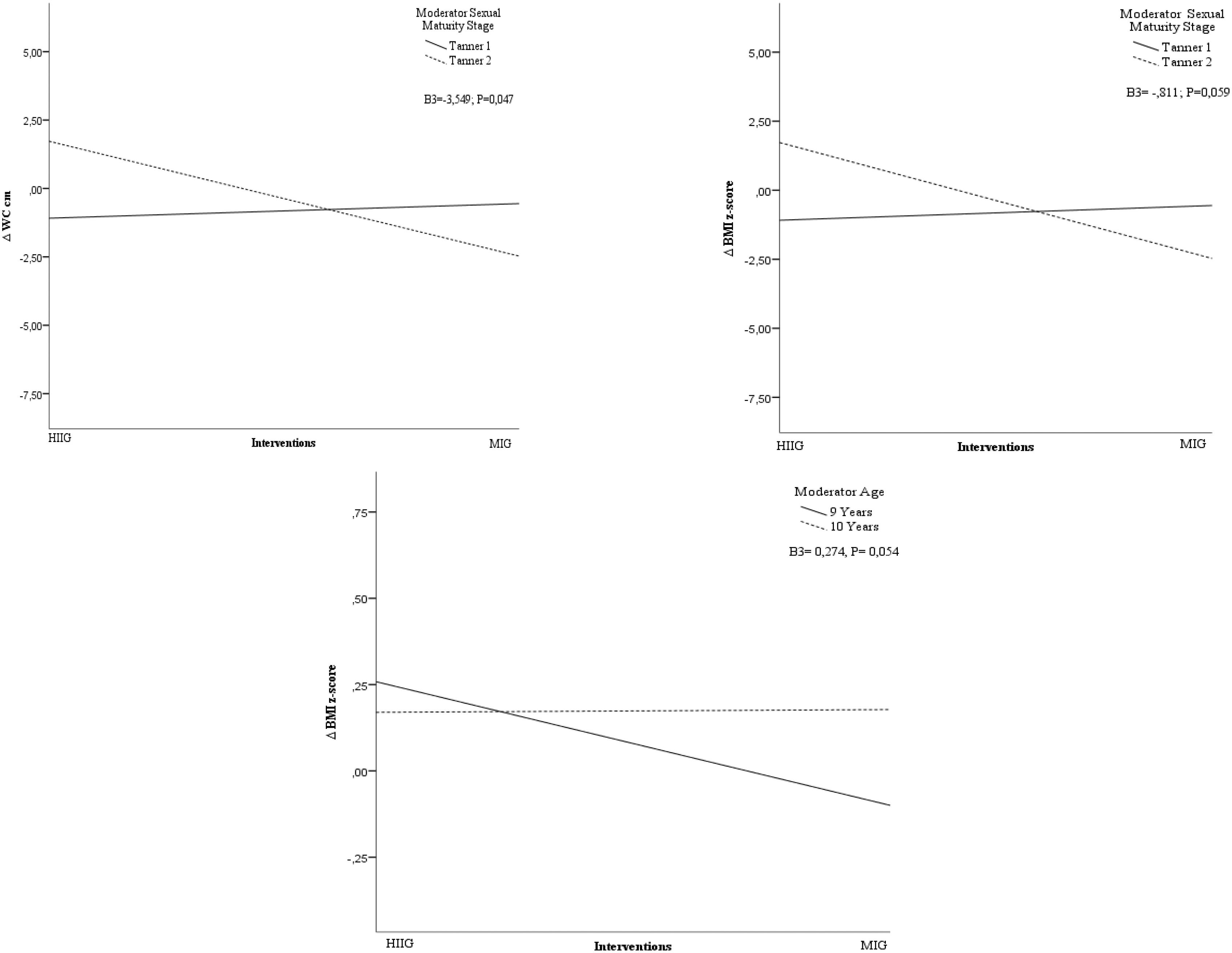
Figure 1 Results Moderation. Interaction. (A) Δ WC – Sexual Maturity Stage; (B) Δ BMI z-score – Sexual Maturity Stage; (C) Δ BMI z-score – Age.
A significant moderation effect on sex was not established in the ΔBMI z-score in the participants of the HIIG intervention. Also, there was no moderation of the sex in the interaction between groups of intervention. Thus, they do not differ in their effectiveness according to sex on ΔBMI z-score (Table 2).
When observing the sexual maturity stage moderation on ΔBMI z-score (Table 2), we noticed that it did not alter the result of ΔBMI z-score. A quasi-significant value of moderation of the interaction between groups of the intervention was observed. Looking at Figure 1, it seems that students in the sexual maturity stage Tanner 2 responded better to MIG than to HIIG, while on Tanner 1, the response was similar to both interventions.
Age does not moderate the result on the ΔBMI z-score. A quasi-significant value of moderation of the interaction between groups of the intervention was detected. Hence, it might have an effect in accordance with the age. Looking at Figure 1, it seems that students of 9 years responded better to MIG than to HIIG, while on 10 years, the response was similar to both interventions.
As shown in Table 2, sex, sexual maturity, and age do not moderate the result on the Δskinfolds sum. Also, sex, sexual maturity stage, and age do not moderate the interaction between groups of intervention; thus, they do not differ in their effectiveness in accordance with sex.
DISCUSSION
The aim of this study was to assess the effect of putative moderators: sex, sexual maturity stage, and age in two types of intervention on CRF and body composition in school-age children.
Cardiorespiratory fitness
CRF is influenced by several factors, including sex, age, body composition, health condition, and genetics (Sardinha et al., 2014). Nevertheless, its principal modifiable determinant is fitness through interventions (Lobelo et al., 2009). However, in the present study, some of these factors did not modify the effect of the intervention. In this study, sex did not moderate the result on ΔCRF since there was no difference in the effect of the intervention with respect to sex. A study with children compared 3-group. Experimental design was applied where short high-intensity intermittent-running training was compared with moderate-intensity continuous-running training and a non-exercising control condition; the findings of this investigation showed that short high-intensity intermittent-running training for boys and girls were mixed, and the results showed no gender effect after training, indicating that both boys and girls increased their CRF (Baquet et al., 2010). The high-intensity intervention and the characteristics of the sample of that investigation (age and students) were similar to our study, and the results correlate with the findings of the present study since sex did not moderate the results. On the opposite, we did not have the same results as Rump et al., (2002) since their study showed that boys performed for a longer period of time, completed a bigger CRF workload, and achieved higher maximal work heart rate than girls. The observed differences in CRF between boys and girls were largely attributable to a difference in body composition and their relationship with CRF.
The findings of the current study did not indicate moderation of the sexual maturity stage, and the interaction of the interventions did not differ in their effectiveness according to the sexual maturity stage. However, it is important to consider the effects of maturity when assessing the fitness of children and adolescents (Malina & Koziel, 1999). The findings of Mota et al. (2002) suggest that the process of sexual maturation per se plays an important role in aerobic fitness, especially in boys and girls.
Age did not moderate the effect of the intervention on ΔCRF, and there was no moderation in the interaction. These results do not match with the results of other studies because evidence showed that modification on CRF increases with age (Lang et al., 2016). However, differences in CRF are more important during adolescence (Pate et al., 2015).
Our study focuses on elementary PE as that can be improved with a program that is feasible in real environments. According to Sallis et al. (1997), health-related PE curricula, with effective teacher training and support, have the potential to provide children with much more PA than they receive in typical PE class, and this increased PA is expected to contribute to multiple health benefits in youth.
PE and classroom programs may increase PA throughout the day, but specific programs to promote generalization must be developed and rigorously evaluated (Sallis et al., 1997; Salmon et al., 2003).
Studies with HIIT programs have consistently shown a greater increase in variables associated with health as cardiorespiratory fitness, but only in extra PE classes or other sessions outside of the educational context (Reyes-Amigo et al., 2017). The present study showed that the high-intensity intervention program performed in the PE classes was effective in participants regardless of sex, sexual maturity stage, and age. The novelty of our study is that the CRF increase is the result of an intervention in a PE class. This study is the first one, to the extent of our knowledge, which as shown that it is possible to integrate high-intensity exercises in PE classes and increase an important indicator of good health in children.
Body composition
Regarding body composition, sex, sexual maturity stage, and age, they did not moderate the effect of the HIIG intervention on ΔBF% and skinfolds sum. Also, there was no moderation in the interaction between groups of intervention. Thus, they do not differ in their effectiveness according to sex on ΔBF%, and skinfolds sum. Unlike our results, another study (Arabi et al., 2004) with schoolchildren – boys and girls ranging from 10 to 17 years old – showed differences in the fat mass and the lean mass with respect to sex. In our study, the intervention was performed in prepubertal children, thus the result correlated with the findings of Mota et al., (2002) in which the indicators of new body fat curves reflected the well-known differences in the development of adiposity between boys and girls. However, the curves are similar in both sexes until puberty, but then they diverge significantly: males proportionately decrease body fat, and females continue to gain.
Contrary to our results about the sexual maturity stage moderation on ΔBF% and skinfolds sum, a recent study of Dias et al. (2018) about the HIIT effect in obese children found differences in the Tanner stage of puberty between boys and girls on BF%, BMI z-score. Our sample had a Tanner stage 1 and 2, so the non-moderation of the biological age coincides with another research (Mezzaroba & Machado, 2014) since the main differences in that research, performed with children and adolescents, were the anthropometrical variables occurred around 12 years old or in the sexual maturity stage Tanner stage 3. The prepuberal group, 10 to 11 year-old-children, had significantly lower values in connection to body composition. Loomba-Albrecht and Styne (2009) showed that the differences in body composition prior to puberty are minor compared with postpuberal differences. Possibly, these results are due to the fact that in the prepuberal stage or chronological ages minor to 12 years, there are no significant differences in body composition (Loomba-Albrecht & Styne, 2009).
The sexual maturity stage of the participants moderated quasi-significantly the interaction between variables about ΔBMI z-score. Better results were seen with MIG. Our results are different from other studies with similar participants that show that high-intensity exercises have better results in the body mass index (Lau et al., 2014). Also, there is evidence showing unclear results about the efficacy of HIIT on body composition (Eddolls et al., 2017).
The present study showed that sex moderated the effect on ΔWC. A similar result was observed in the moderation of the interaction between the intervention and sexual maturity stage on ΔWC groups. These results can be connected to the findings of Filgueiras et al. (2018) due to the difference in the results between boys and girls, as it was identified that girls had higher percentages of fat in the abdominal area (measured with DXA) and a higher WC. A different profile has been observed in children, and a study with the age group of 3–10 years, showed that girls are about four times more likely to accumulate fat in the central region of the body (Melzer et al., 2015). A study performed by Taylor et al. (1997) with children aged 3–8 years showed that even before puberty, there is a difference in body composition between sexes, with girls showing approximately 50% more body fat than boys.
The scientific evidence is not yet clear on the effects of HIIT on the body composition in children and adolescents since there are systematic reviews that conclude that this type of exercise is effective in prepubertal period and point to the need for more research on this matter (Garcia-Hermoso et al., 2016).
The main limitation of our study was the number of participants since this type of study ideally suggests a greater number of participants. Data from the physical activity level and dietary intake were not included in this report, albeit they were collected and are at this moment being processed.
Among the practical applications connected to the findings, it is possible to mention that this method (HIIT) can be incorporated safely in PE classes since it increments CRF with no restriction of age, sex, or sexual maturity stage in students in prepubertal age.
CONCLUSION
This study gives new data on the effect of 3 moderators: sex, sexual maturity stage, and age, in the results of intervention with high-intensity and moderate-intensity exercises during PE classes with a 2 times-a-week frequency.
Sex, sexual maturity stage, and age did not moderate the result on ΔCRF. Furthermore, no moderation was observed in the interaction between groups of intervention. This means that HIIG can be incorporated into PE classes as a tool independent of sex, sexual maturity stage, and age of the student. This finding is important since PE class needs evidence about programs that show positives results in the CRF in real class conditions.
These results were especially important since the present study shows that only the sexual maturity moderated the interaction between groups of intervention on the ΔWC significantly, and sexual maturity and age moderated the interaction between groups of intervention significantly on the ΔBMI z-score. Therefore, the exercises performed by the MIG group had a better effect on students with sexual maturity stage Tanner 2, and children who are 9 years old.
Further research is needed to address the effect of the moderators using low-volume high-intensity interval training in PE classes to improve the overall health in children.
The results of the present study contribute to future lines of research on the moderators of interventions connected to CRF results versus the fatness paradigm, hormonal effect in body composition in the prepubertal period, and the relationship between body composition and high-intensity exercise.

