











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Cerebral palsy (CP) is the major developmental disability limiting function in children due to a defect or lesion that occurs while the brain is under development in the prenatal, perinatal, or postnatal period (Russman & Ashwal, 2004). CP describes a group of movement disorders with various types of motor dysfunctions causing functional activity limitations that are attributed to non-progressive disturbances (Burtner, Woollacott, Craft, & Roncesvalles, 2007; Woollacott & Shumway-Cook, 2005). This disability is associated with different movement patterns, including spastic, dyskinetic, hypotonic, ataxic, and mixed forms (Lambrecht, Urra, Grosu, & Pérez, 2014). Posture and movement are affected, with reduced muscle strength and cardiorespiratory fitness (Nooijen et al., 2014), a limited ability to adjust the postural activity to task-specific circumstances (Ju, Hwang, & Cherng, 2012), and poor selective motor control (Chruscikowski, Fry, Noble, Gough, & Shortland, 2017). Moreover, motor disorders are accompanied by behavior disturbances, limitations on sensation and perceptions, communication problems, and sometimes epilepsy (Bax et al., 2005). Although CP is a lifelong disability, there are many therapeutic interventions that can help reduce its impact on the body/movement and improve the quality of life of these persons (Knox & Evans, 2002).
Physical and occupational therapists use various techniques to improve postural control and motor functions. Hippotherapy must be included in the rehabilitation programmes to improve gross motor function and functional performance (Casady & Nichols-Larsen, 2004) and to improve the psychological and social well-being of children with CP (Jang et al., 2016). Hippotherapy is a therapeutic intervention (Tseng, Chen, & Tam, 2013) that has been used for decades to improve posture, balance, mobility, and function by using the tri-dimensional dynamic movement of horse-riding (Wang et al., 2015). The horse serves as a dynamic basis of support (Haehl, Giuliani, & Lewis, 1999), on which the children do not have any control over but allows to be moved by it. The horses move in step, varying their amplitude, which interferes with the stimulus received by the ride; the greater the amplitude of the horse's pitch, the more adjustments the rider needs to perform. The therapist is the one who controls the movement by varying the horse's stride, cadence, acceleration/deceleration, and direction to facilitate motor skill learning of different abilities to promote gross motor function (Debuse, Gibb, & Chandler, 2009; Haehl et al., 1999; Park, Rha, Shin, Kim, & Jung, 2014). Through the repetitive and rhythmical movements of the horse-riding under various conditions for 30–45 minutes, children experience 3000–5000 repetitions of head and trunk movements, pelvic movements on each of the three axes, and righting reactions (Shurtleff & Engsberg, 2010). These movements affect the sensory, musculoskeletal, vestibular, and oculomotor systems, promoting modifications on the central nervous system and modifications on muscular activation (Casady & Nichols-Larsen, 2004; Pelletier, Higgins, & Bourbonnais, 2015). Therefore, practice and experiences of these movements may promote neuroplastic changes across the central nervous system (Friel et al., 2016; Pelletier et al., 2015) and acquisition of motor abilities (Bartlett & Palisano, 2002).
Hippotherapy has been shown to improve gait (Kwon et al., 2011; McGee & Reese, 2009), head and trunk stability (Shurtleff & Engsberg, 2010; Shurtleff, Standeven, & Engsberg, 2009), gross motor function (Casady & Nichols-Larsen, 2004; Kwon et al., 2015; Park et al., 2014), and functional performance (Casady & Nichols-Larsen, 2004; Park et al., 2014). However, the studies have been centered on the use of hippotherapy and its effects on functionality, but not on frequency (number of sessions) and volume (total time of practice) of hippotherapy per week in these functions. Current practice guidelines in Brazil (ANDE, National Association of Hippotherapy) recommend that hippotherapy sessions be taken once a week for 30 min. Most interventional studies on equine-assisted therapy had an intervention of 15 to 45 minutes in weekly sessions (Borges, Werneck, Silva, Gandolfi, & Pratesi, 2011; Davis et al., 2009; Herrero et al., 2012; Shurtleff & Engsberg, 2010; Shurtleff et al., 2009; Temcharoensuk et al., 2015). Other studies’ interventions showed a duration ranging between 30 to 45 minutes for twice a week sessions (Cherng et al., 2004; Kwon et al., 2011; Park et al., 2014).
Therefore, considering that no interventional studies have been identified that have evaluated the effects on gross motor functions and functional performance of different frequencies per week, the purpose of this study was to determine whether the practice of hippotherapy daily versus twice a week has a different effect on gross motor function and functional performance of children with CP. Therefore, we hypothesize that children who take hippotherapy sessions twice a week have better functional performance and gross motor skills than those who do only once a week.
METHOD
Study design
A quasi-experimental design pre-test/post-test with a comparison group was selected to show changes before and after treatment. The groups were randomly selected. There were four test dates (pre-intervention 1, pre-intervention 2, post-intervention 1, post-intervention 2) with an interval between test data of 16 weeks. Outcomes measures collected four times were gross motor function (GMFM – gross motor function measure) and functional performance (PEDI – Pediatric Evaluation of Disability Inventory). Before the first measurements (baseline), the participants were classified at the gross motor level (gross motor function level – GMFCS) (Palisano, Rosenbaum, Bartlett, & Livingston, 2007). A single-blind assessor to the participant's group conducted the evaluations. The collected data was fully encrypted to ensure the privacy of the participants.
Hippotherapy treatment was administered once a week to a group (30 min per session) and twice a week to the other group (30 min each session) for 16 weeks in both groups (16 and 32 sessions). The sessions were conducted by a physical therapist with ten years of experience, certified in hippotherapy by ANDE BRASIL. All children continued conventional therapy sessions once weekly.
The study 50019415.3.0000.0030 was performed with the approval of the ethical committee of the Faculty of Health Sciences, Universidade de Brasília, Brazil, on February 2, 2016, and carried out in accordance with the standards set by the Declaration of Helsinki. Subjects who are legally responsible for participants had given written consent to the inclusion in the study.
Participants
All participants diagnosed with CP who already performed traditional physiotherapy were recruited from the Center of Hippotherapy in Brasília (ANDE BRASIL) that were registered on the waiting list. The inclusion criteria were as follow:
age 2 to 5 years and 11 months;
GMFCS II to V;
no physical limitation to sit on the horse;
medical authorization.
The exclusion criteria were as follow:
previous participation in hippotherapy;
associated syndromes that make it impossible to perform hippotherapy;
surgery performed in the previous year or expected to be performed;
uncontrolled seizures;
limitation to understand the verbal and non-verbal communication.
A physiotherapist blind to the study screened 29 participants (19 boys, 10 girls) by inclusion criteria. Of the 29 participants who were screened, seven did not meet all the eligibility criteria. After explaining the objective of the study, parents were asked to sign an informed consent. The remaining 22 were randomly allocated by an honest broker, using a table of random numbers to the group with practice once a week (Gp1, n= 11) or to the group with practice twice a week (Gp2, n= 11). The allocation was blinded by the researcher and concealed from the parents until randomization was revealed. The draw was made with a closed envelope. After the randomization and before the first assessment, 2 participants from Gp1 dropped out of the study. The reasons for withdrawal from the Gp1 were residence change and transport difficulty. The final sample consisted of 20 participants, 9 in the Gp1 and 11 in the Gp2 (Figure 1). Participants characteristics for each group are shown in Table 1.
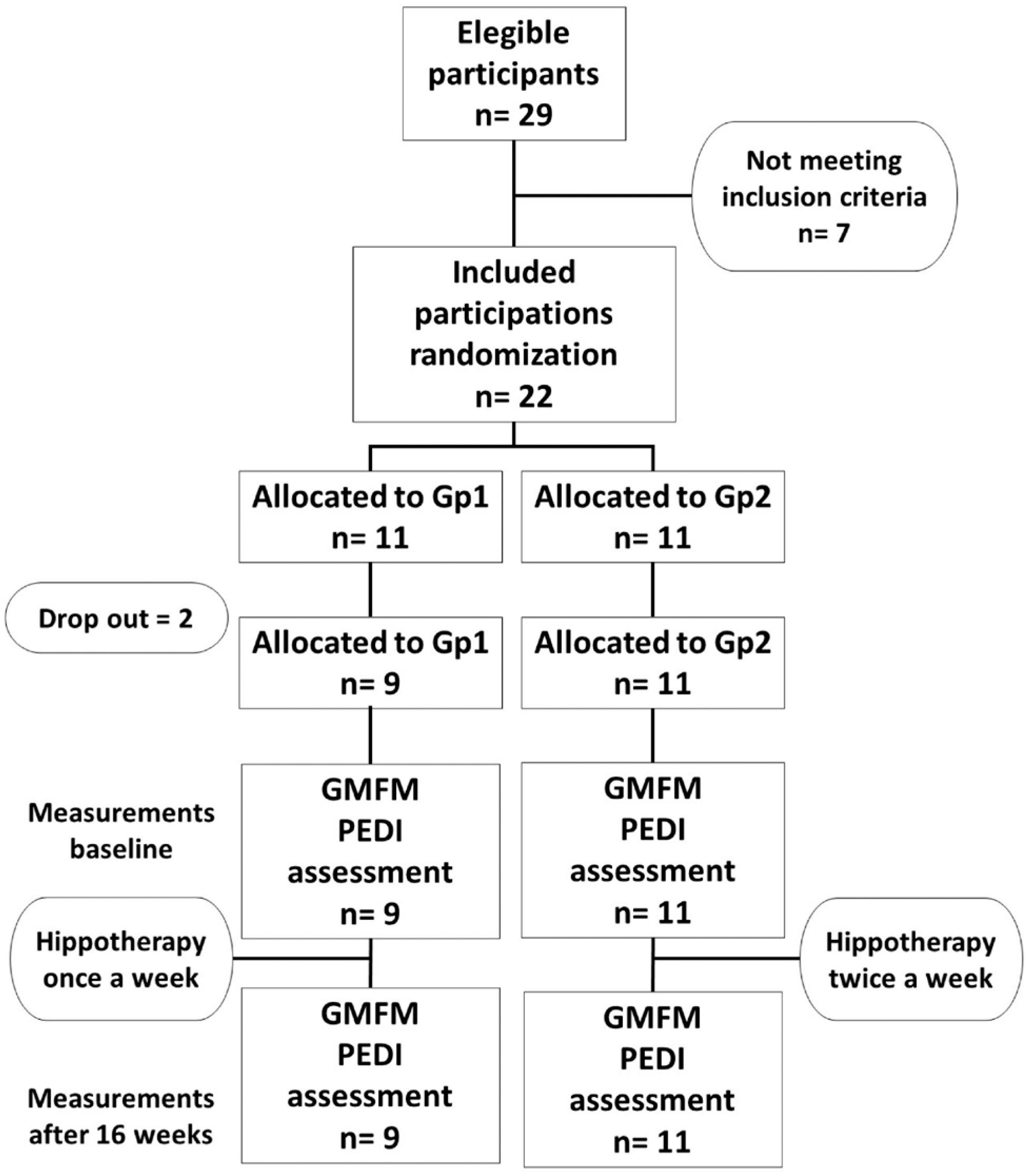
Figure 1 Flowchart of participants in the trial. Gp: group; GMFM: gross motor function measure; PEDI: Pediatric Evaluation of Disability Inventory.
Table 1 Participants characteristics.
| Practice once a week Gp1 (n= 9) | Practice twice a week Gp2 (n= 11) | |
|---|---|---|
| Age (mean± SD) | 40.11± 10.56 | 40.72± 8.91 |
| Sex (M: F) | 8: 1 | 4: 7 |
| GMFCS level (II: III: IV: V) | 1: 3: 1: 4 | 3: 2: 4: 2 |
M: male; F: female; SD: standard deviation; Gp: group; GMFCS: gross motor function classification system.
Hippotherapy intervention
The hippotherapy was performed from March to December 2016 in the center of the hippotherapy of ANDE, Brasília. The hyppotherapeutic interventions were performed from a writing and detailed protocol (Prieto, 2017). Two well-domesticated horses were used for activities. Through the sessions, the children are accompanied by a horse leader responsible for starting, guiding, and stopping the horse, and intervention providers, who are two side walkers responsible for children's safety. The children used a protective helmet. They seated in the horse with a bareback pad to perform various activities to enhance movement in forward and upward directions to solicited postural control, movements of the head, trunk, and pelvic, strength, and coordination. The protocol included activities in the sand and outdoor arena, with asphalt and grass, different slopes, as well as differentiated postures as classic, lateral, inverted, or quadrupedia.
During each individual session, the physical therapist followed target objectives aimed to develop strength, muscle tone, postural stability, sensorimotor and perceptual-motor skills to achieve functional outcomes. The duration of a session was in the range of 30–35 minutes, once or twice a week. The sessions of the group with practice twice a week (Gp2) were not consecutive.
Outcome measures and instruments
For the evaluation of gross motor function (primary outcome measure) and functional performance (secondary outcome measure) were used, respectively, the GMFM-66 and PEDI that are valid and reliable when applied to children with CP (Ketelaar, Vermeer, & Helders, 1998).
Gross motor function measure – GMFM-66
The GMFM is a tool used to measure the capacity of gross motor function in children from 6 months to 16 years of age. Represents the unidimensional construct of gross motor ability and is recommended for research purposes when comparing changes in gross motor function over time in children with CP (Lundkvist Josenby, Jarnlo, Gummesson, & Nordmark, 2009; Russell et al., 2010).
The GMFM-66 were selected from the original GMFM-88 test items through Rasch analysis (Avery, Russell, Raina, Walter, & Rosenbaum, 2003) and provide detailed information on the level of difficulty of each item which is grouped into five dimensions or sub-scales:
A 4-point Likert scale assessment was used for each item (0= does not initiate, 1= initiates, 2= partially completes, and 3= completes) (Lundkvist Josenby et al., 2009).
Pediatric Evaluation of Disability Inventory
The PEDI is a parental/caregiver report measure used for assessing the functional performance of children from 6 months to 7.5 years old. PEDI identifies functional performance in the home and community in three dimensions: functional skills (eating, grooming, toileting, dressing, and sphincter control), mobility (transfers, indoor and outdoor locomotion, and use of stairs), and social function (e.g., communication, problem-solving, interactions). All items were checked as either capable (score 1) or unable (score 0) (Feldman, Haley, & Coryell, 1990).
Statistical analysis
The sample size was calculated considering:
factorial ANOVA test;
2 groups;
type I error= 5%;
type II error= 20%;
power of the statistical test= 80%;
effect size= 60%;
number of measurements= 2.
With the described parameters, it was determined that the total number of individuals would be 20, that is, 10 in each study group. This calculation was performed using the G Power* program, version 3.0.10.
A mixed between-within subjects analysis of variance was conducted to assess the impact of two different interventions (practice once weekly–Gp1, practice twice weekly–Gp2) on participants’ scores on the Gross Motor Function Test, and Functional Performance test with the dimensions “functional skills”, “mobility” and “social functions” across two time periods (pre-intervention, post-intervention).
Descriptive statistics (mean, standard deviation) were computed for each outcome. Shapiro-Wilk test was used to verify the normality of the data. A two-way mixed ANOVA was used, with the moment being a repeated factor to determine the differences between the groups (practice once a week–Gp1 and practice twice a week–Gp2) and between moments (pre-intervention and post-intervention). Effect sizes (ES, Cohen's d) were calculated to demonstrate effects and trends. ES of approximately 0.2, 0.5, and 0.8 are generally considered small, medium, and large effects, respectively (Cohen, 1998). Statistical analyses were performed using SPSS 22.0 software for Windows (Statistical Package for Social Sciences Inc., Chicago (IL), USA), and the criterion for significance was set at p< 0.05.
RESULTS
There was one significant outlier in the data, as assessed by inspection of a boxplot. The outlier from Gp2 was removed from the analysis (Gp2, n= 10).
Gross motor function measure
The data was normally distributed, with homogeneity of variance and homogeneity of covariance. A non-significant time x group interaction for gross motor function (F(1,17)= 1.446, p> 0.05, partial η2= 0.078). There were no significant differences between Gp1 and Gp2 in mean gross motor function score between intervention groups, at the two times points (baseline, and after 16 weeks) (F(1,17)= 1.721, p> 0.05, partial η2= 0.092). In the intra-group analysis, there were significant improvements in the Gp1 (F(1,17)= 37.658, p< 0.001, partial η2= 0.689), and in Gp2 (F(1,17)= 67.532, p< 0.001, partial η2= 0.799).
Functional performance
The data of total functional performance was normally distributed, with homogeneity of variance and homogeneity of covariance. There were no statistically significant interactions between the intervention type and time on total function performance (F(1,17)= 1.459, p> 0.05, partial η2= 0.079). The main effect comparing the two types of intervention was not significant (F(1,17)= 2.354, p> 0.05, partial η2= 0.122). In the intra-group analysis (pre-test and post-test moment), there were significant improvements in the Gp1 (F(1,17)= 26.565, p< 0.001, partial η2= 0.61) and in Gp2 (F(1,17)= 51.668, p< 0.001, partial η2= 0.752).
The data of dimension “functional skills” was normally distributed (p> 0.05), with homogeneity of variance (p> 0.05), and homogeneity of covariance (p= 0.879). There were no statistically significant interactions between the intervention type and time on functional skills (F(1,17)= 1.602, p> 0.05, partial η2= 0.086). The main effect comparing the two types of intervention was not significant (F(1,17)= 2.773, p> 0.05, partial η2= 0.14). There was a substantial main effect for time (F(1,17)= 30.94, p< 0.001, partial η2= 0.645), with both groups showing an increment in functional skills scores across time periods: pre-, post-test (Table 2).
Table 2 Mean (standard deviation) of groups at pre-, post-test, and between-group comparison on the outcomes variables.
| Gp1 (practice once weekly, n= 9) | Gp2 (practice twice weekly, n= 10) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-test | Post-test | Δ% | Cohen's d | aa | Pre-test | Post-test | Δ% | Cohen's d | pa | pb | |
| GMFM | 32.35± 18.22 | 38.68± 18.47 | 19.57 | − 0.344 | 0.000* | 40.46± 11.18 | 48.5± 11.02 | 19.87 | − 0.725 | 0.000* | 0.246 |
| PEDI total | 33.99± 12.46 | 38.48± 13.78 | 13.20 | − 0.339 | 0.000* | 41.64± 11.04 | 47.58± 10.5 | 14.26 | − 0.552 | 0.000* | 0.079 |
| PEDI functional skills | 35.73± 11.78 | 39.81± 13.10 | 11.41 | − 0.325 | 0.009* | 43.40± 10.83 | 49.88± 11.42 | 14.93 | − 0.581 | 0.000* | 0.233 |
| PEDI mobility | 21.94± 16.14 | 28.73± 15.01 | 0.94 | 0.43 | 0.008* | 27.69± 15.71 | 36.44± 13.92 | 31.59 | 0.592 | 0.001* | 0.536 |
| PEDI social functions | 45.97± 9.14 | 46.73± 14.81 | 1.65 | − 0.006 | 0.793 | 55.03± 19.36 | 55.52± 15.43 | 0.89 | − 0.028 | 0.858 | 0.842 |
*denotes significant difference (p< 0.05); GMFM: gross motor function measure; PEDI: Pediatric Evaluation of Disability Inventory; Δ%: percentage variation of each parameter, calculated as the ratio of absolute variation to the base value [
aavalues for within group comparison Gp1;
pavalues for within group comparison Gp2;
pbvalues for group x time.
The data of dimension “mobility” was normally distributed (p> 0.05), with homogeneity of variance (p> 0.05), and homogeneity of covariance (p= 0.994). There were no statistically significant interactions between the intervention type and time on mobility (F(1,17)= 0.399, p> 0.05, partial η2= 0.023). The main effect comparing the two types of intervention was not significant (F(1,17)= 0.976, p> 0.05, partial η2= 0.054). There was a substantial main effect for time (F(1,17)= 25.272, p< 0.001, partial η2= 0.598), with both groups showing a increment in mobility scores across time periods (Table 2).
The data of dimension “social function” was normally distributed (p> 0.05), with homogeneity of variance (p≥ 0.05), but the covariance matrices are not equal (p= 0.029), so the interaction (time x group) are not interpreted. There were no significant differences in mean social function scores between intervention groups, in pre-test (F(1,17)= 1.636, p= 0.218, partial η2= 0.088), and post-test (F(1,17)= 1.597, p= 0.0223, partial η2= 0.086). There were no significant differences in mean social function scores between pre, and post-test, in Gp1 (F(1,17)= 0.007, p= 0.793, partial η2= 0.004), and Gp2 (F(1,17)= 0.033, p= 0.858, partial η2= 0.002).
DISCUSSION
This study hypothesized that children with CP who underwent hippotherapy twice a week would have a better gross motor function and functional performance, but our results point out an improvement within groups, but not between the groups after the intervention.
Gross motor function
When the data related to the gross motor function of the participants of groups 1 and 2 were analyzed, no significant differences were found between the groups after the experimental period. However, when analyzing the averages obtained in the evaluations of the children, the group with the frequency of twice a week seems to have a slight increase compared to the group once a week. Both groups had statistically significant differences after hippotherapy (intragroup analysis). Regarding the size of the effect, it was noted that it was the only variable that presented a moderate effect size among group 2.
Other research has also sought to evaluate gross motor function after hippotherapy. The studies proposed by Sterba, Rogers, France and Vokes (2002) and Cherng et al. (2004) reported improvements of 7 and 5% in the total GMFM score, respectively. Similar results were found by Kown et al. (2015) and Park et al. (2014) who presented positive results after hippotherapy, the last one with 91 subjects randomly distributed with significant differences both intra-group and between groups. A study in Thailand (Temcharoensuk et al., 2015) also observed positive outcomes in this study variable, comparing three groups: the control group, the hippotherapy simulator group, and the traditional hippotherapy group, which presented higher results. However, the Australian study proposed by Davis et al. (2009), which managed to gather the largest number of subjects (99), did not observe significant differences in the gross motor function of this same population studied.
Some authors have also proposed to carry out systematic review studies on this topic. In all reviews, including a meta-analysis, no consistent increases in GMFM were observed after the hippotherapy practice (Cherng et al., 2004; Snider, Korner-Bitensky, Kammann, Warner, & Saleh, 2007). These studies report that most of the included studies have poor methodological quality, reduced number of participants, absence of control groups, and no randomization of the sampling process (Casady & Nichols-Larsen, 2004; Snider et al., 2007).
Functional performance
Analyzing the intragroup data obtained in the PEDI inventory in relation to functional performance, a statistically significant difference was observed in the dimensions of self-care and mobility, which did not occur in the social function dimension. However, the results between the groups did not show significant change. However, like GMFM, in PEDI, the differences in means were also larger in the group twice a week.
Previous studies have also concluded an improvement in functional performance after hippotherapy. Moraes, Copetti, Angelo, Chiavoloni and David (2016) observed a statistically significant difference after 24 sessions that happened twice weekly. Other authors also reported significant improvements in functional performance after the hippotherapy (Casady & Nichols-Larsen, 2004; Haehl, Giuliani, & Lewis, 1999; Park et al., 2014). In addition to hippotherapy, other studies also used the PEDI inventory to evaluate the effects of rehabilitation programs. Knox and Evans (2002) investigated treatment with the Bobath method in children with CP, identifying positive changes in functional performance in 15 children with a mean age of 7 years and 4 months. Another study evaluated the PEDI inventory before and after traditional physiotherapy and concluded favorable results, indicating that the treatment facilitates normal movement, improving strength, flexibility, amplitude, and movement patterns and, in general, functional performance (Leite & Prado, 2004).
The activities selected for the protocol as the type of utensil used in the mount, in our case, the blanket without stirrup, may also have contributed to improved motor function and functional performance of participants (Antunes et al., 2016). The blanket was selected for providing greater contact with the horse, allowing a greater sensation of the animal's movement and greater recruitment of the trunk muscles (Espindula, 2014; Espindula et al., 2012). The zigzag movements, up and down movements, change in the frequency and amplitude of the horse's gait, and the variations in posture generate different physical challenges and modify the proposed stimuli, besides prioritizing neuropsychomotor development (Leite & Prado, 2004; Moraes et al., 2016).
It is also suggested that improvements in tonus, postural control, gross motor function, and functional performance may occur due to the non-clinical and enjoyable environment in which the therapy happens (Casady & Nichols-Larsen, 2004; Lindroth, Sullivan, & Silkwood-Sherer, 2015; Snider et al., 2007). Therefore, children are rich and stimulating motor activity participants and can be fun and therapeutic, essential factors to promote physical and psychic improvements (Casady & Nichols-Larsen, 2004; Moraes et al., 2016; Sterba, 2007). CP is a chronic condition where the therapeutic process occurs throughout life (Rothstein & Beltrame, 2013); therefore, motivation is necessary for attendance and frequency in the treatment (Shurtleff et al., 2009; Snider et al., 2007).
The limitations of the present study include a selection of subjects at various functional levels and reduced numbers of participants in both groups. This same difficulty in recruiting a representative number of subjects is common in studies on CP (Herrero et al., 2012), besides the complexity of the pathological condition in homogenizing the sample (Temcharoensuk et al., 2015). However, our study was the first to compare the weekly frequency of care, seeking answers to hippotherapy practice results. Despite the small sample, the groups were divided randomly and blinded.
Future studies should address these limitations by increasing sample size and homogeneous groups to elucidate the effect of hippotherapy in children with CP. It is also suggested to investigate the frequency, time, and duration of treatment.
CONCLUSIONS
This study showed significant benefits in GMFM-66 and PEDI of children with CP; however, a greater effect size of treatment was observed twice a week. The results found in the study are relevant mainly in relation to public policies for people with disabilities. Because it is a high-cost and often inaccessible therapy for some of these people, and with the results found in this study, it can be concluded that the hippotherapy performed once or twice a week seems to produce positive effects on gross motor function and functional performance in children with CP.

