











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
In the last years, the prevalence of overweight and obesity in children has increased worldwide (Koning et al., 2016; World Health Organization, 2020; Ferreira et al., 2021). In Brazil, between the 1990s and 2010s, the prevalence rate of overweight and obesity in children increased ate about 12%, achieving the highest rates in the south (10.1%) and southeast (10.6%) regions (NCD Risk Factor Collaboration, 2017; Ferreira et al., 2021). From the set of health problems associated with being overweight during childhood, it has been highlighted that obese children are more prone to become obese adults (World Health Organization, 2020); in addition, high body fat percentage during childhood is associated with an increased risk of chronic diseases development (such as type II diabetes mellitus, hypertension, hypercholesterolemia, coronary heart disease and respiratory disease), which can be observed still during childhood/adolescence, but with health consequences during later life (NCD Risk Factor Collaboration, 2017).
Obesity is a multifactorial trait, influenced by both environmental factors (social, physical, and built) and individual characteristics (such as lifestyle and biological factors), meaning that the mutual relationship between these variables would imply differences in the prevalence of overweight around the world, and also the development of strategies aiming to reduce its incidence should be thought taking into account these factors (NCD Risk Factor Collaboration, 2017; Blüher, 2019).
The health-related behaviours, as well as disease risk factors, tend to track from childhood to adulthood (Koning et al., 2016; NCD Risk Factor Collaboration, 2017). In this context, providing opportunities for physical activity (PA) is relevant to increasing health benefits (Malina, Cumming, & Coelho e Silva, 2016). The health benefits of PA have been largely studied, which involve improvement of self-esteem and self-efficacy, social benefits, decrease in risk for development of chronic diseases, and also controlling and reducing overweight at a population level (NCD Risk Factor Collaboration, 2017; Ferrari, Matsudo, Katzmarzyk, & Fisberg, 2017). However, despite its benefits, a marked reduction in PA levels has been observed among the pediatric population (Koning et al., 2016). Furthermore, in association with the decrease in PA levels, it is observed a reduction in motor competence (MC), health-related physical fitness (HRPF) and perceived motor competence (PMC) levels (Stodden et al., 2008). These factors play a relevant role in child development and can also be relevant in the reduction of the risk of obesity (Ferreira et al., 2021), highlighting that they need to be properly developed during childhood (Estevan, García-Massó, García, & Barnett, 2019; Yuksel, Şahin, Maksimovic, Drid, & Bianco, 2020). The stimulus for the practice of different types of PA should be emphasised, aiming to contribute to physical development. In addition, the improvement of MC and HRPF favour the involvement in a large number of sports practices and PA’s. Thus, motor experiences acquired during childhood tend to contribute to an increase in muscle strength, endurance, flexibility and maintaining healthy weight status (Barnett et al., 2016; Utesch, Bardid, Büsch, & Bernd, 2019).
Previous studies that investigated individual predictors of childhood overweight (especially in the second childhood) (Ferrari et al., 2017), suggested that MC (Cattuzzo et al., 2016; Laukkanen, Pesola, Finni, & Sääkslahti, 2017; Herrmann, Heim, & Seelig, 2019), HRPF (Cattuzzo et al., 2016; Lima et al., 2017; Tyler, Mackintosh, Spacey, & Stratton, 2020), PA (Freire, Pope, & Coyle, 2019), and PMC (Lopes, Saraiva, Gonçalves, & Rodrigues, 2017; Meester et al., 2017) can be related to childhood overweight/obesity in children and adolescents of both sexes. In addition, the associations between MC, HRPF and PMC at this stage of life seem to be associated with health-related markers (Barnett et al., 2016; Cattuzzo et al., 2016; Yuksel et al., 2020). Furthermore, sex differences regarding PA and physical fitness are reported, and studies show that boys are usually more physically active and present higher physical fitness levels than girls (Katzmarzyk et al., 2016; Zaqout et al., 2016; Meester et al., 2017), which may lead to differences in the prevalence of excess weight between sexes (Oliveira, Ferrari, Araújo, & Matsudo, 2017). Thus, low PA and physical fitness levels are largely reported as associated with increases in the risk of overweight and obesity (Katzmarzyk et al., 2016; Lima et al., 2017).
In the Brazilian context, more than six million children aged between five and nine years old are overweight (Abeso, 2021), highlighting the relevance of understanding which variables are associated with overweight and obesity in this age group in order to provide information to be used during intervention programs aiming to reduce health risks in later life (Di Cesare et al., 2019). Thus, the present study aimed to estimate sex differences in BMI, MC, HRPF, PMC, and PA; and identify individual predictors associated with overweight in Brazilian children from the Zona da Mata of Minas Gerais. Hence, based on the literature, we hypothesised that boys would have better results in health variables compared to girls; and a significant association would be observed between MC, HRPF, PMC, and PA with overweight in children.
METHOD
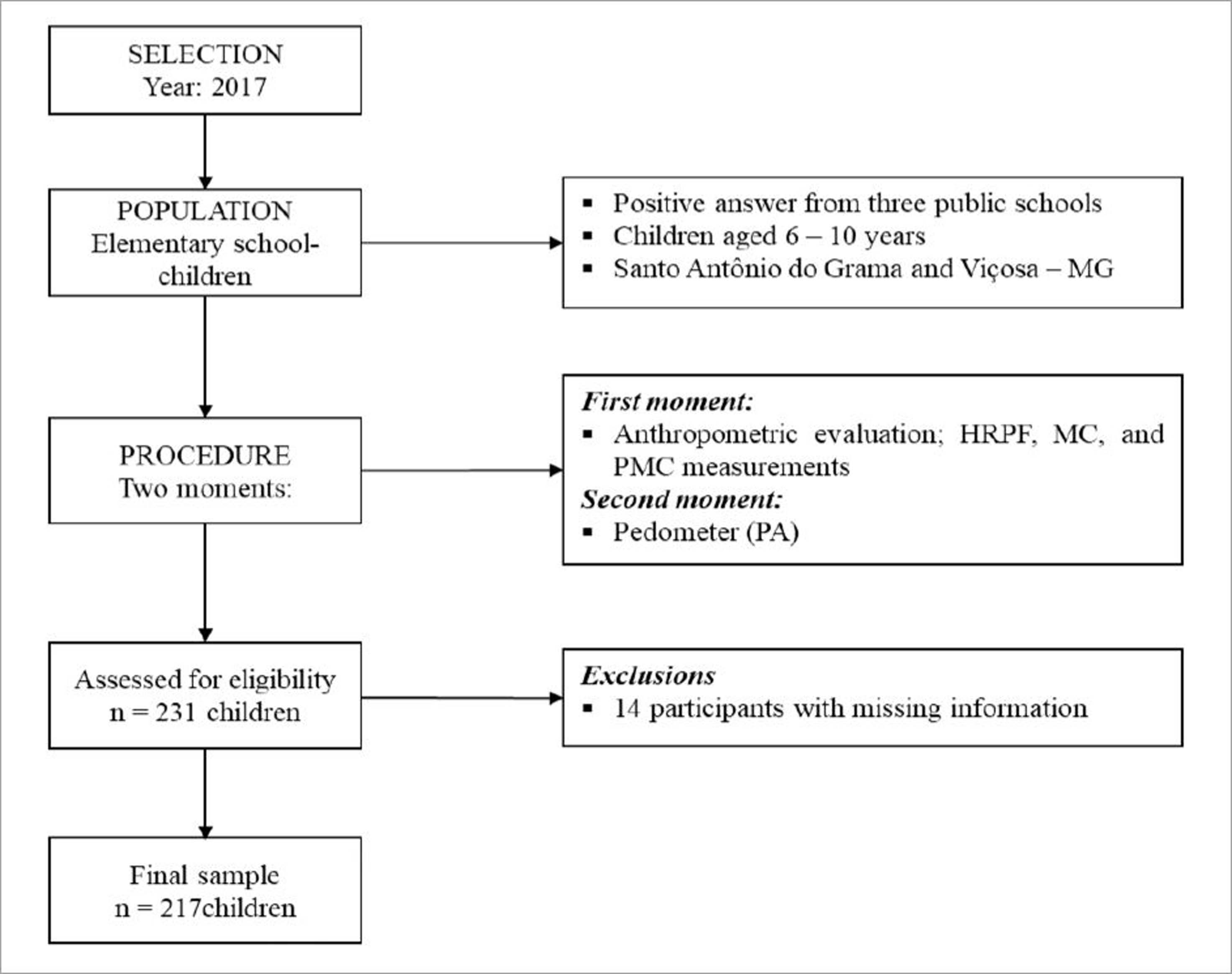
This is a cross-sectional epidemiological study, which is part of the “Relationship between physical activity, motor competence, cognitive abilities and school performance in children aged 3 to 12 years”. The research project was approved by the Ethics Committee on Research with Human Beings of the Universidade Federal de Viçosa, under protocol No. 1.888.177. To participate in the research, children's parents/legal guardians signed the consent form. Figure 1 shows the sampling process.
Participants
A total of 231 children (125 boys and 106 girls) were evaluated, of which 14 children were excluded during the data analysis process due to missing information. Thus, the final sample comprised 217 children (100 girls, 117 boys), aged six to 10 years old, enrolled in public municipal schools from Viçosa and Santo Antônio do Grama, MG, Brazil. A preliminary analysis was performed the estimate differences in variables studied between children from both cities, and no statistically significant differences were observed. To be included in the study, children must be aged between six to 10 years old, and present the consent form signed by their legal guardian; children who presented some physical/cognitive impairment that prevented regular physical activity, and who had missing information were not included in the study.
Measures
Height was assessed using a high-precision portable stadiometer (Sanny, São Paulo, Brazil, precision of 0.1 cm) and body mass was measured using a digital scale (TEC-117, Tech Line, São Paulo, Brazil, with a precision of 0.1kg). Both measures followed standard procedures described by Lohman, Roche and Martorell (1988) and BMI was computed using the standardised formula [BMI= body mass (kg) / height (m2)]. The children's nutritional status was determined according to the WHO cut-off point, and children were classified as low weight, eutrophic, overweight, and obese (De Onis et al., 2007). For further analysis, children were regrouped into two groups, namely “eutrophic” (included low weight and eutrophic) and “overweight” (overweight and obese).
The pedometer (Yamax, Digi-Walker, Model SW 200, Japan) was used to estimate the number of children's daily steps, being a valid and reliable instrument for measuring PA in children (McNamara, Hudson, & Taylor, 2010). Children were taught to use the device during their awake time for seven consecutive days, including at least two weekend days. Children with valid pedometer information for at least four days (with at least one weekend day) were considered “eligible” to be included in the study, of which at least one day should refer to a weekend day (Duncan, Al-Nakeeb, Woodfield, & Lyons, 2007).
A total of five tests were used to estimate the HRPF: abdominal strength (curl up), upper limb strength (push up) and flexibility (sit-and-reach) from the FITNESSGRAM test battery (Plowman & Meredith, 2013); lower limb strength (horizontal jump) and cardiorespiratory fitness (6-minute walk/run), from the PROESP-BR test battery (Gaya & Gaya, 2016). The HRPF test scores were converted to “z values”, and summed to compute an “HRPF total score”, which was later used during the analyses, as performed in previous studies (Lima et al., 2017; Jaakkola et al., 2019; Tyler et al., 2020).
MC was evaluated by the use of the Test of Gross Motor Development 2nd Edition (TGMD-2) (Ulrich, 2000), which evaluates twelve fundamental motor skills, divided into locomotion and object control skills. This test battery provides scores for each of these skills, and the sum of them allows the estimation of a motor quotient (MQ) properly adjusted for age and sex. In the present study, values of the total MQ achieved by the child were used.
The PMC was evaluated using the Pictographic Evaluation Scale of Perceived Competence in Motor Skills (Barnett, Robinson, Webster, & Ridgers, 2015). This scale aims to measure the children's perception of motor competence in the same skills evaluated by the TGMD-2 test battery, with both, female and male versions. The results for each item in each subscale range from one (low competence) to four (high competence), resulting in four possible levels of PMC for each skill. In the analyses, the mean values from the twelve questions of the scale were used, according to the amplitude of the answers on the Likert scale.
Procedure
Data collection occurred in two moments (between February and March of 2017). In the first moment, anthropometric evaluation, as well as HRPF, MC, and PMC measurements were performed. In the second moment, after the conclusion of all evaluations previous cited, children were asked to wear the pedometer to estimate their PA. Data collection was performed by a research team (professors, undergraduate and master students from the Universidade Federal de Viçosa), trained to perform the procedures.
Statistical analysis
The analysis was conducted for the total sample, as well as by sex, through the statistical software IBM SPSS STATISTIC® version 22 (IBM Corporation, Armonk, New York, United States). Descriptive statistics information (mean, median, standard deviation, interquartile ranges and frequencies) was used to characterise variables. The assumptions of normality distribution were tested (Kolmogorov-Smirnov test), and the Mann Whitney U test for independent samples was used to test differences between sexes for all variables.
Multiple logistic regression analysis was performed to identify predictors of overweight in children. The model was adjusted by sex and age. All independent variables were introduced at the same time into the model, according to the forced entry method “enter”. The quality of fit of the model was evaluated by the log-likelihood test, and odds ratios (OR) and associated 95% confidence intervals (95%CI) were calculated to determine the strength of the model (Hair, Black, Babin, & Anderson, 2009). For all analyses, the significance was set at p< 0.05.
RESULTS
In the present sample, 87.1% of the children were classified as normal weight, while 12.9% were classified as overweight. Table 1 presents descriptive information and a comparison by sex. The sample showed a mean age of 8.34± 1.59 years. The results showed that boys presented a better performance in the HRPF total score (U= 4,295, p= 0.001), and had higher average daily steps on weekend days (U= 4,872.50, p= 0.034) and in the whole week (U= 4,854, p= 0.031) when compared to girls. No statistically significant differences were observed for other variables (p> 0.05).
Table 1 Descriptive sample information and comparison by sex.
| Variables | Girls | Boys | Total | p-value | |||
|---|---|---|---|---|---|---|---|
| Mean± SD | Median (IQR) | Mean± SD | Median (IQR) | Mean± SD | Median (IQR) | ||
| N | 100 | 117 | 217 | ||||
| Age (years) | 8.35± 1.71 | 8.25 (3.70) | 8.13± 1.47 | 8.11 (2.30) | 8.34± 1.59 | 8.20 (3.20) | 0.310 |
| Height (cm) | 130.66± 11.44 | 131 (16) | 130.83± 9.59 | 131 (12) | 130.75± 10.46 | 131 (15) | 0.775 |
| BM (kg) | 28.86± 7.70 | 27.10 (10.75) | 29.12± 8.23 | 27.70 (9.77) | 29.00± 7.97 | 27.45(10.47) | 0.806 |
| BMI (kg/m2) | 16.65± 2.39 | 16.22 (3.36) | 16.77± 3.00 | 16.05 (2.98) | 16.71± 2.73 | 16.15 (3.15) | 0.834 |
| MC | 80.50±12.06 | 79 (18.) | 77.54± 10.74 | 76 (15) | 78.89± 11.45 | 79 (18) | 0.080 |
| HRPF (score z) | 0.66± 2.67 | - 0.71 (2.93) | 0.56± 2.73 | 0.42 (3.69) | 0.00± 2.77 | – 0.29 (3.61) | 0.001 |
| PMC | 3.26± 0.51 | 3.33 (0.87) | 3.40± 0.42 | 3.41 (0.67) | 3.33± 0.47 | 3.33 (0.75) | 0.060 |
| PA - Week days (steps) | 7,109.3± 3,525.59 | 6735.00 (4761.00) | 8,804.30± 4,022.40 | 7,638.00 (5,377.00) | 7,635.02± 3,824.07 | 7,045.75 (4,877) | 0.138 |
| PA - Weekend days (steps) | 6,820.5± 4,363.66 | 6,462.11 (5,288) | 8,029.30± 4,600.20 | 7,521.50 (7,162.00) | 7,635.02± 3,824.07 | 7,045.75 (4,877) | 0.034 |
| Total PA (steps) | 7,042.1± 3,519.25 | 6,371.75 (4,705.25) | 8,066.00± 3,683.80 | 7,416.66 (4,786.75) | 7,635.02± 3,824.07 | 7,045.75 (4,877) | 0.031 |
Multiple logistic regression analysis revealed that MC (OR= 0.97; 95%CI 0.92– 0.98; p= 0.043) and HRPF (OR= 0.78; 95%CI 0.66– 0.93; p= 0.007) were significantly associated with overweight. Further, PA and PMC were not statistically significant associated with overweight (Table 2).
Table 2 Multiple logistic regression analysis for individual predictors of overweight, adjusted by sex and age.
| Predictors | β | OR (95%CI) | p-value |
|---|---|---|---|
| Motor competence | -0.02 | 0.97 (0.92– 0.98) | 0.043 |
| Health-related physical fitness | - 0.23 | 0.78 (0.66– 0.93) | 0.007 |
| Physical activity | 0.01 | 1.00 (0.99– 1.01) | 0.893 |
| Perceived motor competence | 0.03 | 1.03 (0.95– 1.12) | 0.443 |
| Constant | - 6.10 | -- | 0.081 |
Results showed a negative association between MC and HRPF with overweight, meaning that high levels of MC (β= -0.02) and HRPF (β= -0.23) decrease the odds of children being overweight.
DISCUSSION
This study aimed to estimate sex differences in BMI, MC, HRPF, PMC, and PA and describe the individual predictors associated with overweight in Brazilian children aged six to 10 years. Sex differences were observed in HRPF and PA, with boys presenting higher physical fitness scores, and also being more physically active. In addition, regarding the predictors of overweight, MC and HRPF were significantly associated with overweight in children. Finally, our hypothesis was partially confirmed, since boys showed better health indicators when compared to girls, in some variables (HRPF and PA), and some of the predictors were associated with overweight in children.
Regarding sex differences for PA and HRPF, the results of the present study are similar to previous studies, in which boys tend to perform better than girls (Oliveira et al., 2017; Tyler et al., 2020), suggesting that these differences may be associated with the type of PA and/or motor activity boys and girls take part in their daily routine (Freire et al., 2019). Such differences can be related to social values and practices, where during childhood, girls are encouraged to play static games while boys are motivated to get engaged in dynamic and vigorous activities (Yuksel et al., 2020). At this point, it is possible that cultural aspects lead boys to be more physically active than girls, and this fact may lead to higher improvement in HRPF compared to girls, given that the relationship between physical fitness and PA is complex and apparently bidirectional (Katzmarzyk et al., 2016; Slykerman, Ridgers, Stevenson, & Barnett, 2016; Meester et al., 2017).
In the present study, no statistically significant differences were observed in the comparison between sexes for MC, similarly to studies conducted by Herrmann et al. (2019) and Slykerman et al. (2016) where authors suggested that habits and activities that require motor tasks may offer greater opportunities for practice for both sexes. Furthermore, the lack of a significant difference between sexes may be due to the fact that the total MC score comes from the sum of all the subtests (locomotion and object control). Where boys performed better in the object control subtest, while girls showed better results in the locomotion subtest (data not shown), but these differences were mitigated when considering all the tests together (total MC score), indicating the absence of sex differences. Similarly, for the PMC variable, no statistically significant differences were observed between sexes, and this is in agreement with some previous studies (Lopes et al., 2017; Meester et al., 2017). In general, age has been pointed out as a factor that influences the PMC (Meester et al., 2017; Jaakkola et al., 2019), where the youngest children often do not have a PMC that matches their MC. In the present study, when analysing each item of the pictographic scale, we did not observe significant differences in mean values; however, girls presented higher mean values in items related to locomotion skills, while boys presented higher mean values for object control skills (data not shown). Similar to results observed for total MC, these findings can be related to the absence of significant sex differences in this variable.
Multiple logistic regression analysis showed that MC and HRPF were associated with overweight in the studied sample, meaning that by increasing MC and HRPF, children were less likely to be overweight. These results highlight the relevance of stimulating and developing the motor skills in children, in order to subsidise their involvement in different physical activities, which can improve HRPF (Estevan et al., 2019; Utesch et al., 2019). It should be noted that the results of this study corroborate results reported in previous studies that found that MC and HRPF are negatively associated with weight status (Zaqout et al., 2016; Laukkanen et al., 2017). As children remain engaged in a range of activities, health-associated benefits may be observed. It's known that the negative association found may represent a reciprocal relationship of the interactions of predictors with overweight, in other words, children who develop adequate levels of MC and HRPF may present healthy weight status in childhood. This mechanism acts over time, showing the highest strength of association between variables alongside child development (Cattuzzo et al., 2016). However, it was not possible to verify the strength of the associations due to the cross-sectional design of our research. We believe and support that the strength of the associations between the variables becomes more intense with the growth and development of children (Lima et al., 2017).
On the other hand, no significant association was observed between PA and PMC with overweight in children. Eventually, these results, regarding PA, can be due to the fact that the sample of the present study may experience similar PA opportunities and environments to be active, regarding the characteristics of the cities they are from. As an example, from the set of possible activities performed by children, most of them reported to be involved in football, karate, dance, and swimming (data not shown), highlighting the similarities regarding the activities they were involved in, which can explain the absence of significant association between PA and overweight, since they must have similar PA levels. We support future research, that can help to better understand this variable (measuring the type and intensity of PA) and its association with childhood overweight. Although PA was not associated with overweight in our study, we support and encourage the regular practice of PA in children. PA maintenance during the growth and development processes seems to be an important factor not only in increasing body weight control but also in the structural and functional integrity of skeletal muscle tissue (Malina et al., 2016), in addition to the benefits (physical, psychological and social) associated with this practice, especially in this age group (Bull et al., 2020).
The PMC predictor showed no significant association with overweight. In addition, as proposed by Stodden et al. (2008) younger children seem to show limited accuracy of PMC, usually overestimating it. In the present study, when the sample was stratified by age groups, those aged 6-7 years (representing about 40% of the total sample), it was observed that this group showed high levels of PMC (data not shown), similar to that suggested by Stodden et al. (2008). This fact can have led to the absence of significant results regarding its association with overweight, given these children may have reported their PMC higher than their real MC. In addition to the age factor, other aspects such as the instrument used, cultural, social, and geographical characteristics of the environment, may have influenced the PMC, however, the importance of this construct in childhood, as well as its relationship with overweight, is emphasised.
Results of the present study are of relevance due to the fact that investigated, at the same time, different predictors of overweight in children, which can allow a better understanding of its expression. We believe that the development and improvement of motor skills, and consequently the MC, aligned with PMC, as well as good levels of HRPF, may contribute to a healthy body weight status. In addition, even though PA and PMC were not significant predictors of overweight in the present study, we suggest and encourage children to practice and engage in different PA’s, free play, play, and other expressions of human movement, which can be important strategies to children healthy weight status over time.
The use of objective measures and/or techniques to assess BMI, MC, HRPF and PA, is one of the strengths of our study. In addition, we investigated predictors associated with overweight in a sample with unique characteristics (both in economic and cultural aspects). On the other hand, we recognise the limitations of our study and they may contribute to future studies. We support that other methods of body composition analysis are more reliable than BMI, currently employed. The pedometer, even though it is a valid and reliable instrument for measuring children's PA, does not evaluate the intensity of the activity, which limited the understanding of our findings. The sample of our study is not representative of the state, or even the country, which limits the generalisation of the results. We suggest future studies can address predictors of childhood overweight through follow-up and/or interventions throughout childhood.
CONCLUSION
The present study analysed individual predictors associated with overweight in children aged six to 10 years old. In general, boys had a better HRPF profile as well as a higher PA level than girls. Furthermore, results indicated that MC and HRPF were significantly associated with overweight in children.
Such results point to the relevance of investigating and evaluating the set of individual predictors from an early age, especially in understanding their association with childhood overweight. Promoting physical activities that stimulate and challenge children to perform them, can be one strategy to improve their MC and HRPF, increasing the chances of maintaining a healthy weight status during childhood and later life.
The results found, highlight the relevance of children being engaged in a large number of PA’s, aiming to develop/improve different motor skills, which would be related to increment in MC and HRPF, leading, as consequence, to decreases in the chances of excess weight during childhood.

