











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Air Bike leg- and arm- ergometers recently emerged in the fitness industry, especially in CrossFit®, and it became of common use in fitness centres. Air Bike Revolution is a cycle ergometer that allows the use of the upper and lower limbs simultaneously while seated. Its characteristic is that of a system of external load imposed through air resistance which increases with the cadence imposed on the equipment. This equipment is used both in aerobic low-intensity and anaerobic interval high-intensity training programs.
To our knowledge, there are no studies on cardiorespiratory measures with this equipment, probably due to its novelty. Nevertheless, there are several validated protocols in equipment with similar electromagnetic or air resistance (Balmer et al., 2000a; 2000b). There are major differences in heart rate (HR), oxygen uptake (VO2), lactate and respiratory exchange ratio (RER) when they are compared in these equipment (Lindenthaler et al., 2018).
To assess cardiorespiratory fitness, maximal tests with incremental load performed in an ergometer are typical (Stevens & Dascombe, 2015). Data from these tests are either used as a fitness measure or a tool in exercise prescription, enabling a more precise, safe and effective exercise intensity. Physiological measures commonly involved in maximal testing are oxygen uptake (VO2), ventilatory thresholds, HR and rate of perceived exertion (RPE) (Mielke et al., 2009).
Thus, it is relevant to investigate whether cardiorespiratory measures in a maximal test in the leg- and arm- Air Bike ergometer matches those with a standard leg- cycle ergometer. Once the Air Bike Revolution has never been tested regarding its reliability, we herein assess this. Moreover, once standard cycle ergometer VO2max protocols are designed to be applied in leg-only ergometers, e also compared the Air Bike response to that in a leg cycle ergometer. Hence, it is relevant to investigate whether cardiorespiratory measures in a maximal test in the leg- and arm- Air Bike ergometer matches those with a standard leg- cycle ergometer. Therefore, the present study aimed to evaluate the reliability of a ramp test and standard leg- cycle ergometer to assess maximum oxygen uptake (VO2max). We hypothesised that a maximum test on the Air Bike Revolution enabled us to assess the VO2max and that cardiorespiratory measurements are reliable in this ergometer.
METHODS
Participants
Eighteen physically active young men, aged 21.78 ± 2.44 years, 1.77± 0.05 m in height and 75.78± 8.39 kg of body mass, volunteered to participate in the present study. The participants met the following inclusion criteria: they had to be involved in regular exercise for at least 12 months with a frequency of at least twice a week; they could not present any medical condition able to impair maximal exercise tolerance; they could not use any drug during the experiment (including alcohol, tobacco and caffeine); they could not answer positively in any item of the PAR-Q questionnaire. The sample’s representativeness was post hoc adjusted by the sample size calculation, with G-Power software (Faul et al., 2007) requiring an effect size of 1.12 (Cohen, 1988) for a 95% statistical power. After a complete explanation of the methods, each participant filled out and signed a free and informed consent prepared in accordance with the declaration of Helsinki (World Medical Association, 2013). The study was approved by the University of Trás-os-Montes e Alto Douro research ethics committee (Doc25-CE-UTAD-2020).
Experimental design
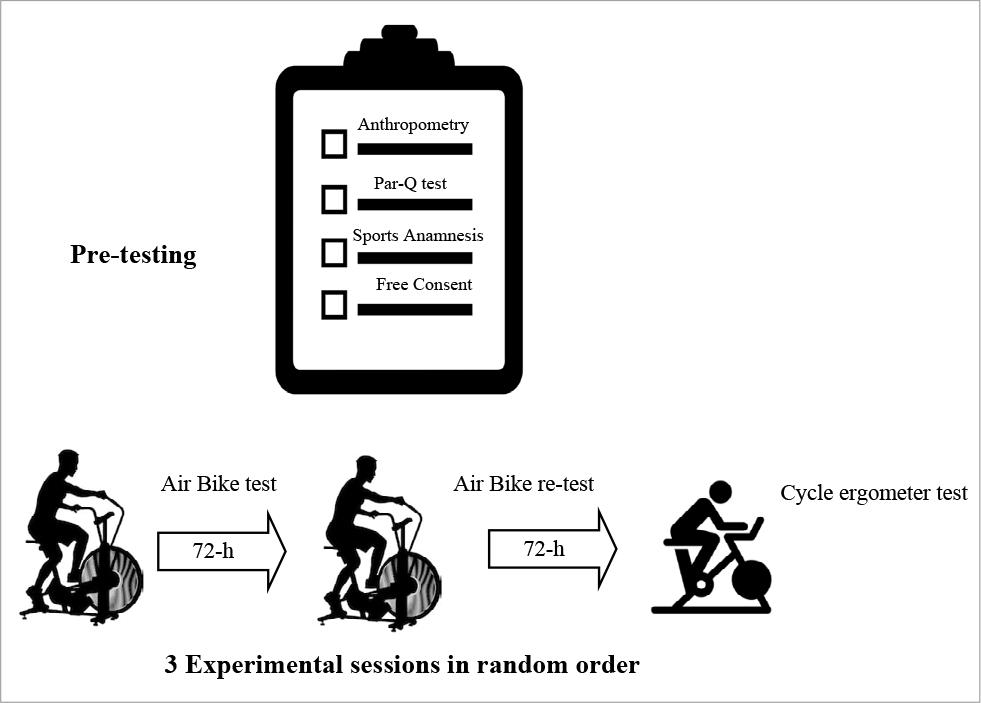
A prospective compared single-centre study. On the first visit to the laboratory, the participants were submitted to anthropometric measurements, followed by the first experimental session with cardiorespiratory testing. Each participant performed three experimental sessions of maximal testing on a ProTrainer cycle ergometer (Wattbike, Nothingham, UK) and an Air Bike Revolution ergometer (BoxPt, Póvoa de Varzim, Portugal), through an incremental load ramp protocol. The three experimental sessions were separated by 72 hours and performed in random order at the same time of the day. From the three sessions, two were held with Air Bike Revolution (test and re-test) and one with the cycle ergometer. Figure 1 displays the experimental design. The participants were instructed to maintain an identical food and water intake prior to the 3 experimental sessions. To assure proper hydration, a minimum of 330ml of water were required to be ingested in the 2 hours preceding each experimental session.
Anthropometric measurements
A stadiometer (Sanny ES 2030, American Medical do Brasil, Ltda, São Paulo, Brazil) was used for height measurement. The height was defined as the distance, in a straight line, between the uppermost point of the skull and the lowest point (in this case, the floor where the feet were placed), with the subject in an anthropometric (erect) position. That is, by drawing an imaginary line (using an object as a linear example: ruler) that passes through the lower point of the lower edge of the right eye orbit and the highest point on the upper side of the corresponding external auditory meatus. The subjects stood barefoot, with the heels together, forming a “V” with the feet and the coccyx, a dorsal column, and a posterior part of the head in contact with the stadiometer. The reading was expressed in centimetres to the tenths and recorded after a deep inspiration.
An electronic scale was used to assess the body mass (Tanita BF-562, Tanita Europe B. V., Yiewsley Middlesex, United Kingdom), where subjects wore only shorts and stood barefoot in the centre of the platform of the scale and remained immobile until stabilisation of the scale digits. Body mass was expressed in kg to the nearest tenths.
Maximal testing
Two cycle ergometers were used, a ProTrainer cycle ergometer which required standard leg-only cycling and an Air Bike Revolution ergometer which required lar- and arm-cycling exercise. The individual adjustment of the vertical saddle of the ergometers was standardised by the point where the individual presented a knee extension as close as possible to full extension. The protrainer cycle ergometer is an ergometer that calculates the energy production through an individual load cell for each pedal, thus distinguishing the force performed independently by the left lower limb and the right lower limb. It is a reliable instrument, well studied, validated and with reliable values and tests concerning the measured power (Hopker et al., 2010; Wainwright et al., 2016).
Due to the differences between the cycle ergometers in terms of their relationship between cycle cadence and power output, we conducted several pre-testing with 5 subjects. These pre-tests were performed from lower exercise intensity up to an exercise intensity at the second ventilatory threshold. The pre-tests were designed to standardise the cycle cadence in the two ergometers; in order to attempt to have a similar power output while maintaining standardised constant-intensity increases. While in the leg- cycle ergometer, the load imposed by the electromagnetic mechanism is used to increase power output, in the Air Bike ergometer, power output can only be increased by increasing cycle cadence.
Table 1 presents the standardised protocols applied, from the lowest to the highest intensity attained during the experimental sessions. In both ergometers, the test started with the participants resting seated on the ergometer for 2 minutes (Haapala et al., 2018). In the leg-cycler ergometer, the test started with a load of 25 Watts, with a cadence of 60 rpm, with an increase of 25 W of load every minute (Carey & Richardson, 2003; Hopker et al., 2010). On the other hand, with the Air Bike ergometer, the test started at 30 rpm, with an increase of 5 rpm every minute. The tests were performed until exhaustion, being interrupted when the subject was unable to maintain cadence and/or power output.
Table 1. External load during the tests.
| Stage | Air Bike ergometer | Cycle ergometer | ||
|---|---|---|---|---|
| Cadence (rpm) | Power (watt) | Cadence (rpm) | Power (Watt) | |
| 1 | 30 | 27 | 60 | 25 |
| 2 | 35 | 44 | 60 | 50 |
| 3 | 40 | 65 | 60 | 75 |
| 4 | 45 | 89 | 60 | 100 |
| 5 | 50 | 121 | 60 | 125 |
| 6 | 55 | 156 | 60 | 150 |
| 7 | 60 | 205 | 60 | 175 |
| 8 | 65 | 306 | 60 | 200 |
| 9 | 70 | 377 | 60 | 225 |
| 10 | 75 | 466 | 60 | 250 |
| 11 | 80 | 558 | 60 | 275 |
| 12 | 85 | 778 | 60 | 300 |
| 13 | 60 | 325 | ||
Physiological measurements
The ventilation and expired gases were measured using a portable open circuit system (COSMED® K4b2, Rome, Italy). This device was used in a breath-by-breath analysis during all sessions, with subsequent averaging in 20-s intervals (Haapala et al., 2018). The gas analyser was previously switched on 45 minutes before use until it reached the internal temperature of 36°C of the device (McLaughlin et al., 2001). Subsequently, the device was calibrated before each session with a mixture of ambient gas and a mixture of gas of the known calibration (16.00% oxygen and 5.00% carbon dioxide). The device turbine was also calibrated with a 3-litre syringe (McLaughlin et al., 2001) supplied by the manufacturer. Room air and delay calibrations were also performed. HR was obtained through a strap (Wireless Double Electrode, Polar®, Kempele, Finland) placed on the participants’ chests in all experimental sessions. The electrodes were moistened and placed at the level of the xiphoid appendix. The HR values were obtained beat by beat. The OMNI CYCLE rate of perceived exertion scale of 10 values (Robertson et al., 2004) was used during all experimental sessions,
The VO2max was the highest 20-s average value of relative VO2 obtained during the maximum tests. Criteria to declare VO2max included: i) VO2 plateau; ii) respiratory exchange ratio≥ 1.10; iii) HR≥ 90% of the predicted maximum HR (Poole & Jones, 2017); iv) inability to maintain power output; v) rate of perceived exertion≥ 8 on the OMNI (Mezzani, 2017). At least 4 of the 5 criteria were required to declare the VO2max.
The analysis of all data was performed using the IBM SPSS Statistics for Windows (Version 25) predictive analytics software. Exploratory data analysis was performed where normality and homoscedasticity assumptions were verified. The Intraclass Correlation Coefficient was used to test the reliability between the maximum VO2 measurements in the Air Bike ergometer (test and re-test), and t-tests were performed to compare measurements between the two ergometers. In these comparisons, data with the Air Bike ergometer were the average of both measurements. Bland-Altman plots (Bland & Altman, 2010) were also used to investigate the agreement between the 2 ergometers and simple linear regression between vales with the two ergometers showed the standard error of the estimate. The level of significance was set at 5%.
RESULTS
An excellent intra-class correlation (ICC) was observed for VO2max measures in the two tests with the Air Bike ergometer (r= 0.96), and good correlations were found in all other variables that were analysed, HR (r= 0.75), RER (r= 0.87) and test duration (r= 0.86).
The values in Table 2 VO2max and maximum heart rate (HRmax) were significantly higher in the Air Bike compared with the cycle ergometer (53.06± 8.72 vs 47.38± 9.15 mL/min/kg), 181.93± 10.20 vs 176.07± 5.28 bpm, p< 0.001; 95%CI 3.41–7.95; ES= 0.30 and p= 0.01; 95%CI 1.44–10.29; ES= 0.34, respectively for VO2max and HRmax).
Table 2. Means (± standard deviation) in the two ergometers and standard error of the estimations with Air Bike ergometer.
| Air Bike | Cycle Ergometer | SEE | Relative SEE (%) | |
|---|---|---|---|---|
| VO2max (mL/min/kg) | 53.06± 8.72 | 47.38± 9.15** | 4.42 | 9.3 |
| HRmax (bpm) | 181.93± 10.20 | 176.07± 5.28* | 8.21 | 4.7 |
| RER | 1.21± 0.13 | 1.21± 0.14 | 0.1 | 8,3 |
| Time (s) | 598.06± 37.28 | 612.22± 86.40 | 26.12 | 4.3 |
VO2max: maximum oxygen uptake; HRmax: maximum heart rate; RER: respiratory exchange ratio; Time: total duration of maximum test; SEE: standard error of the estimate; **P< 0.001; *P= 0.01.
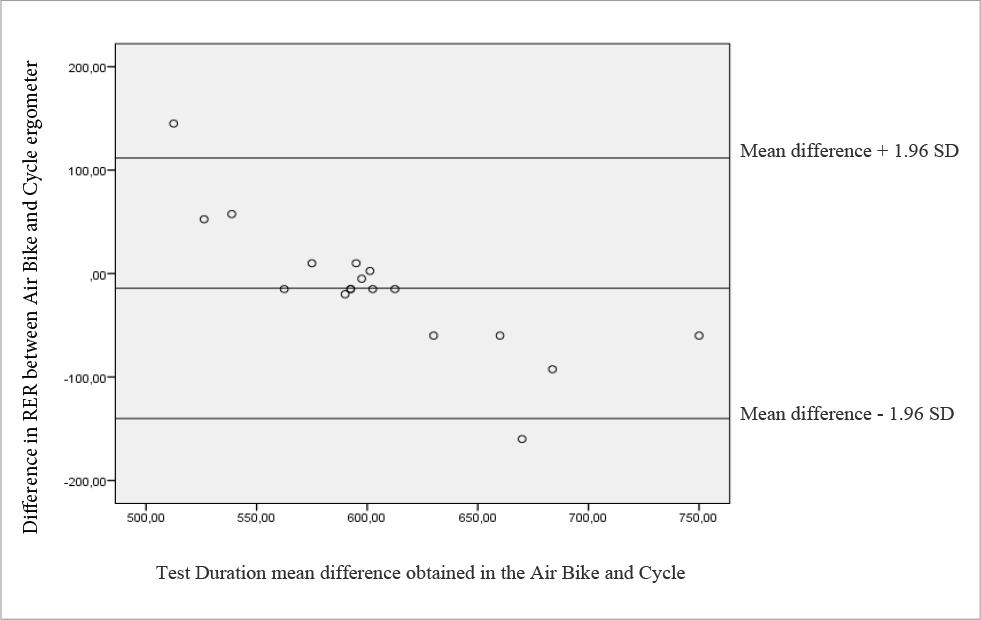
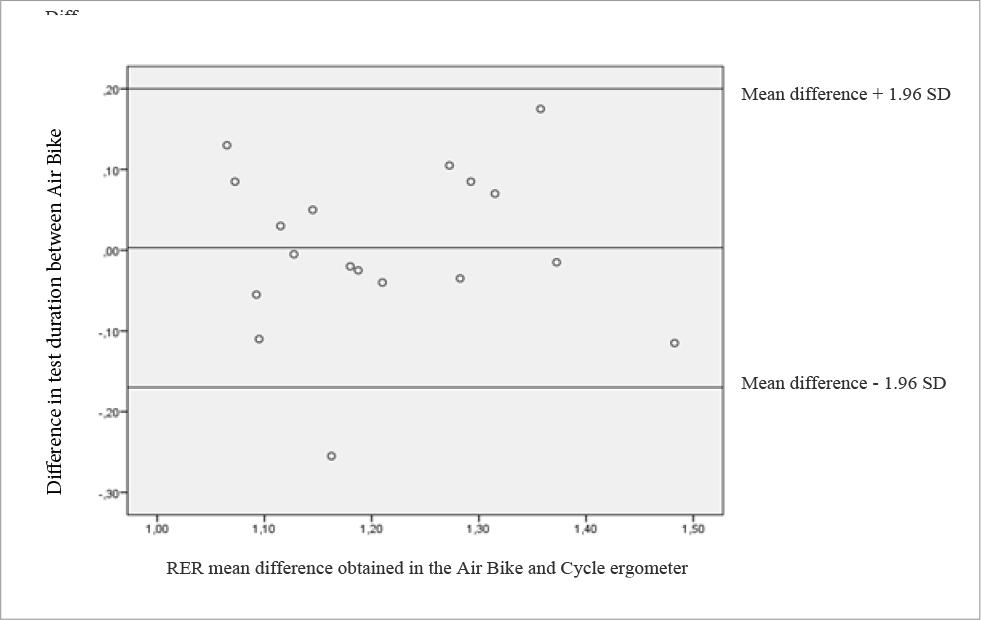
There are no significant differences between ergometers in RER and test duration, as confirmed by the Bland Altman plots (see Figures 2 and 3).
DISCUSSION
The present study investigated whether cardiorespiratory measures in a maximal test in the leg- and arm- Air Bike ergometer are reliable and if they match those with standard leg- cycle ergometer. We hypothesised that a maximum test on the Air Bike Revolution enabled the measure of VO2max and that cardiorespiratory measurements are reliable in this ergometer. To the best of our knowledge, this is the first study to investigate maximal testing on a leg- and arm- cycle ergometer as the Air Bike herein.
The main results of this study show that the maximum test performed on the Air Bike ergometer enabled higher VO2max and HRmax as compared with the standard cycle ergometer. Moreover, the maximum test performed on the leg- and arm- ergometer proved to be reliable for VO2max and HRmax.
Cycle ergometers are often used either in a recreational or competitive context, more often to carry out efforts of longer duration and moderate intensity (predominantly aerobic). However, these are also used in high-intensity exercise, at intensities that enable the VO2max. Hence, maximal cardiorespiratory testing is often performed with standard leg- cycle ergometers. Different ergometers are expected to yield different maximal cardiorespiratory measures. Indeed, different VO2, HR and ventilation have been shown by the study of (Lindenthaler et al., 2018), who compared a Wattbike cycle ergometer /the same as used in the present study) with the Concept II Rower ergometer at various and similar power outputs. In addition, the later study describes that when the VO2 values were equal between ergometers, differences in HR and ventilation were observed, reinforcing the specificity of each ergometer. In another study (Egan et al., 2016) performed the same comparison, cycle ergometer vs. rowing ergometer, and observed differences in VO2 and HR, both at sub-maximal intensities (50% VO2max) and at maximal exertion. In fact, differences in cardiorespiratory measures between lower limb vs upper limb exercise were longtime established (Schneider et al., 2002). Our data confirm all these, as leg- and arm- cycle exercise did enable higher cardiorespiratory output (VO2 and HR), though this was the first study to conclude the Air Bike ergometer in comparison against standard cycling.
Maximum VO2 in the Air Bike ergometer was more than 10% above that measured in the cycle ergometer. Generally, large muscle mass involvement is the main reason to explain higher VO2 and HR (Reis et al., 2017), as seen by Egan et al. (2016) and by Lindenthaler et al. (2018) in cyclical exercise of durations from 4 to 20-min. Also, the same phenomenon has been described in exercises with anaerobic predominance, for example in resistance training (Farinatti et al., 2016). Moreover, the fact that the power output was much higher in the Air Bike for the similar protocol stages and exercise duration can also help to explain the larger VO2max.
Although the training status and subsequent adaptations to specific ergometers have also been presented as explanations for differences between the physiological response to different ergometers (McNarry et al., 2011), this was not the case in the present study, as the subjects were regularly active but not involved in specific training with either of the two ergometers herein.
Even when ergometers with similar movement are compared, differences may result from differences in the loading system, which can be imposed either by electromagnetic or air resistance (Balmer et al., 2000a). Additionally, the manufacturers of the ergometers are not the same, so the magnitude and/or kinematics may differ, which can increase the bias of internal load markers (Balmer et al., 2000b; Mahony, 1999). The two ergometers used in the present study had different loading systems. Therefore, a thorough pre-testing was warranted to establish a ramp protocol that would be as close as possible to the two ergometers. Still, though implementing concomitant relative increases in the load, clear different power output was observed when the Air Bike ergometer exercise cadence surpassed 60 rpm (see Table 1). The most fit subject attained stage 13 in both tests. The majority of subjects attained around 10 min in both ergometers, resulting in a power output of 466w in the Air Bike ergometer and 250w in the cycle ergometer.
Some possible limitations of the current study include the sample size and the fact that the VO2max protocol used as reference was performed on a watt bike ergometer, whose mechanics are slightly different from that of standard le cycle ergometers.
CONCLUSION
It is concluded that a maximal ramp test carried out on the Air Bike is a reliable tool to assess VO2max and enables a higher VO2max as compared with a standard leg- cycle ergometer. Since leg- and arm cycle ergometers are currently found in most gyms and fitness centres, the results herein show that this ergometer may be used to test maximal aerobic power and to be used as an alternative to leg-only cycle ergometers.

