











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
The use of dietary supplements (DS) to enhance athletic performance is a relatively new development in sports. In the past three decades, a vast array of supplements has emerged, transforming DS into a multibillion-dollar industry valued at USD 177.5 billion in 2023 (Grand View Research, 2024). Despite this financial success, contaminated DS remains a problem in this area (Mallick et al., 2023), and the link between DS and doping cases has been widely documented, with multiple studies reporting contaminated supplements and athletes failing in anti-doping tests (Torres et al., 2024; Zapata-Linares & Gervasini, 2024).
Thus, from a probabilistic point of view, it seems reasonable to assume that the higher the consumption of DS, the greater the chances of a tested athlete being caught with prohibited substances, mainly under the strict liability principle established by anti-doping rules (World Anti-Doping Agency, 2021). Consequently, some nutritionists and experts, both in and out of the sports environment, have adopted a “meal first” or “food first” approach (Yasuda et al., 2023; Yu et al., 2024). Despite the good evidence supporting the role of some DS in improving performance and recovery (Maughan, Burke et al., 2018), those who are contaminated with prohibited substances pose a threat to high-performance athletes and their careers (Lauritzen, 2022).
Athletes’ DS consumption is influenced by a number of causes, including age, sex, physiological needs, as well as cultural, financial and psychological factors. A particular sport, region, country, or even a team seems crucial to understanding the risk of doping associated with DS use.
This study aimed to analyse DS consumption among Brazilian athletes from Olympic and Paralympic disciplines, considering gender, the consumption period (in or out of competition), and the number of supplements reported as consumed from 2015 to 2022.
METHODS
Study design
In order to achieve the proposed goal, an analytical observational study was conducted. The researchers analysed all Doping Control Forms (DCFs) under the Brazilian National Anti-Doping Organisation (ABCD) testing authority from 2015 to 2022. According to WADA rules, this authority holds the decision-making power regarding who, when, and how an athlete will be tested (World Anti-Doping Agency, 2021).
Procedures
According to the International Standards for Testing and Investigation (World Anti-Doping Agency, 2020), the DCF is a document with five copies filled in by a Doping Control Officer (DCO) with the corresponding information of the athlete selected for doping control. Thus, the samples (urine, blood, or both) are collected and sent to be analysed by a WADA-accredited laboratory, and, at the same time, the DCO and the athlete provide information regarding their sport and discipline such as whether the test was performed in-competition or not, their sex, the day and time of the sample collection, a self-report of the dietary supplements (DS) and medications consumed in the last seven days prior to the sample collection, among other data. All athletes were tested under the authority of ABCD, and all samples were analysed by the Brazilian Doping Control Laboratory (LBCD), where the researchers evaluated at least one of the copies of all DCFs with the mentioned information. This study did not manipulate any biological samples, and all the necessary information was extracted from the athletes’ DCFs and the Anti-Doping Administration and Management System (ADAMS).
The information regarding the sample number, gender, date, whether it was in-competition or out-of-competition according to WADA definition (World Anti-Doping Agency, 2021), and the sport/discipline was extracted from ADAMS and transferred into an Excel spreadsheet. The declarations of use of medications and supplements in the last seven days reported in DCFs were transcribed into the same spreadsheet.
The copy of the DCFs used for this study omitted the athlete’s name. Thus, it was not possible for the researchers to establish an association between a DCF and any specific athlete, or whether the test result was positive, or not. Additionally, this study was submitted to the Ethics Committee (Plataforma Brasil - CAAE 57397122.5.0000.9433) and was approved, receiving the number 6029126. Furthermore, this study and its methods were also approved by ABCD.
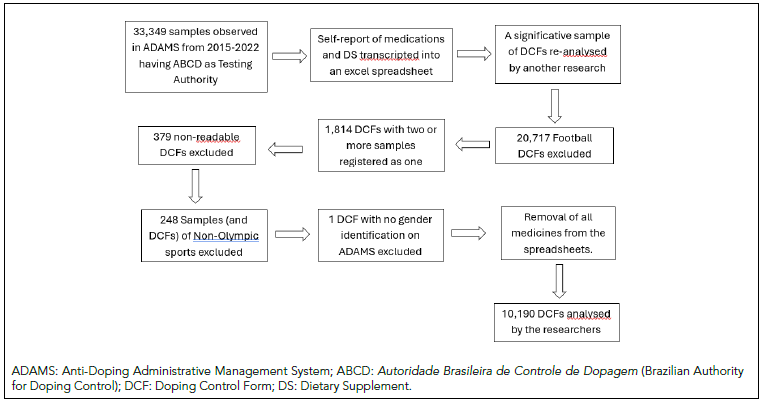
In the study, 10,190 DCFs were analysed from a total of 33,349 samples extracted from ADAMS. Firstly, it was decided to exclude footballers from the study, removing a total of 20,717 samples, for two main reasons. The first concerns the analysed period since the number of footballers who were tested was about two times bigger than all of the other sports combined, and this discrepancy could lead to a misinterpretation of the data. The second reason is the fact that football in Brazil is a sport with a completely different profile than all the others; Brazilian footballers generally have a different socioeconomic status, greater salaries, and competition calendar, their clubs are structured differently, and so on (Guterman, 2009; Proni, 2021). For these reasons, another study will be conducted exclusively with footballers.
Additionally, DCFs with two or more samples were registered as only one sample. 1,814 samples (5.44% of total) fell into this category and were connected to the collection of blood and urine of the same athlete at the same time, or to when the provided urine samples presented a specific gravity below 1,005, in which case a new urine collection was necessary. Beyond that, a total of 379 (1.14% of total) DCFs were unreadable because of poor handwriting, because the carbon copy with the supplements was too clear, or because they were written in a language other than Portuguese, English, Spanish or French. Furthermore, 248 samples (0.74%) were from non-Olympic or Paralympic sports (bodybuilding, squash, automobile sports, arm wrestling, waterskiing, chess, darts, boule sports, mixed martial arts, etc) and were thus not included in this study. Finally, there was one DCF which did not have a gender identification when it was extracted from ADAMS and was removed from the total of analysed DCFs.
To avoid possible mistranscriptions of the DS, another researcher collected a statistically representative sample of the same information. After this second collection, the spreadsheets were compared, and the data was confirmed.
After that, all medications were removed from the original spreadsheet, and only the DS remained. Figure 1 illustrates the methodology used.
Statistical analysis
In regard to the statistics, a frequency analysis was initially conducted to characterise the number of supplements used by athletes both generally and specifically (in or out of competition, by gender, and by sport type).
Subsequently, χ2 tests were applied to compare dietary supplement (DS) use between male and female athletes, in-competition and out-of-competition, throughout the years, including all Olympic and Paralympic sports and disciplines except football. Additionally, the Cramer’s V was calculated as an effect size. A Kruskal-Wallis test with a Dunn´s test and a Bonferroni adjustment test to evaluate differences in the number of DS reported by athletes each year.
The Mann-Whitney test was used to examine differences in the quantity of supplements used according to gender, collection period, and sport type, but only among athletes who reported DS use.
All analyses were performed with a statistical significance level of 95% using SPSS version 21.0.
RESULTS
In total, 10,190 Doping Control Forms (DCF) were analysed. Of those, 39.36% (4,011) are from women and 60.64% (6,179) are from men. Additionally, 69.33% (7,065) represent DCFs from an in-competition period, and 30.67% (3,125) are from an out-of-competition period. Finally, 20.46% (2,085) of the DCFs belong to Paralympic athletes and 79.54% (8,105) to the Olympians. Furthermore, it is important to point out that ABCD is solely responsible for these numbers and proportions.
In total, 28.46% of all athletes reported no consumption of supplements, and 71.54% reported at least 1 DS. Table 1 represents the distribution of frequency related to the number of DS reported by all athletes.
Table 1. Frequency of supplement use reported by Brazilian athletes.
| Number of Reported Supplements | Number of DCFs | % | Accumulated % |
|---|---|---|---|
| 0 | 2,900 | 28.46 | 28.46 |
| 1 | 1,211 | 11.88 | 40.34 |
| 2 | 1,111 | 10.90 | 51.24 |
| 3 | 1,138 | 11.17 | 62.41 |
| 4 | 986 | 9.68 | 72.09 |
| 5 | 747 | 7.33 | 79.42 |
| 6 | 590 | 5.79 | 85.21 |
| 7 | 451 | 4.42 | 89.63 |
| 8 | 274 | 2.69 | 92.32 |
| 9 | 222 | 2.18 | 94.50 |
| 10 | 137 | 1.34 | 95.84 |
| 11-15 | 334 | 3.28 | 99.12 |
| 16-20 | 70 | 0.69 | 99.81 |
| 20 and more | 19 | 0.19 | 100 |
DCFs: Doping Control Forms.
When observing the average number of DS consumption reported by the athletes, it becomes clear that there is an increase in this mean in Olympic years (2016 and 2021) when compared to their immediate pre- and post-Olympic Games years. Table 2 shows the number of DS reported on each DCF by year and the respective comparison among these years using ANOVA One-Way with Bonferroni post hoc test.
Table 2. Average number of reported use of Dietary Supplement per year of collection (n= 10,190).
| Collect Year | n | Median | Mean± SD | Post Hoc | Minimum | Maximum | p-value |
|---|---|---|---|---|---|---|---|
| 2015 | 658 | 3 | 3.14± 3.18 | a | 0 | 19 | < 0.001 |
| 2016 | 1,900 | 3 | 3.44± 3.49 | b,c,d | 20 | ||
| 2017 | 1,170 | 2 | 2.90± 3.44 | b,e,f | 25 | ||
| 2018 | 1,272 | 2 | 2.66± 3.27 | a,c,g,h,i,j | 29 | ||
| 2019 | 1,513 | 2 | 3.01± 3.29 | d,g,k | 30 | ||
| 2020 | 611 | 3 | 3.45± 3.42 | e,h | 21 | ||
| 2021 | 1,378 | 3 | 3.67± 3.80 | a,f,i,k,l | 21 | ||
| 2022 | 1,688 | 2 | 3.24± 3.59 | j,l | 29 | ||
| Total | 10,190 | 2 | 3.20± 3.48 | 30 |
Same letters represent a significative difference between years; a: p= 0.003; b, d, f, h, i, j: p< 0.001; c: p= 0.009; e: p= 0.002; g: p= 0.013; k: p= 0.001; l: p= 0.046; p-values after Kruskal-Wallis test with a Dunn´s test and a Bonferroni adjustment test; SD: Standard Deviation.
The data also shows that there is a greater use of dietary supplements (DS) by female athletes in comparison to male athletes, both in and out-of-competition periods. The fact of it being an Olympic or Paralympic sport did not present any difference in the analysed sample (Table 3).
Table 3. Use of Dietary Supplement (DS) according to gender, period of sample collection and the type of sport/modality.
| DS use | Gender | Period of sample collection | Sport Type | |||
|---|---|---|---|---|---|---|
| Female | Male | In | Out | Olympic | Paralympic | |
| No |
|
|
|
|
|
|
| Yes |
|
|
|
|
|
|
| p-value | 0.007 | < 0.001 | 0.160 | |||
| Cramer’s V | 0.025 | 0.055 | 0.010 | |||
In: In competition; Out: Out of competition; p-value obtained after χ2 test.
When examining only the athletes who reported DS consumption on their DCFs, and analysing the number of reported DS, in total, there is an amount of 4.47± 3.35 (mean± SD) per athlete. Furthermore, differences in these numbers among male vs. female athletes and in-competition vs. out of competition periods could be observed. The fact of being an Olympic or Paralympic sport did not show any significance. The Mann-Whitney test was used to compare these results. The results are shown in Table 4.
Table 4. Average of Dietary Supplement (DS) use among athletes who reported DS use.
| Groups | n | Mean± SD | p-value | r | |
|---|---|---|---|---|---|
| Sport Type | Olympic | 5,816 | 4.46± 3.36 | 0.552 | 0.010 |
| Paralympic | 1,474 | 4.54± 3.26 | |||
| Period of sample collection | Out of competition | 2,119 | 4.83± 3.59 | < 0.001 | 0.060 |
| In competition | 5,171 | 4.33± 3.25 | |||
| Gender | Female | 2,924 | 4.65± 3.63 | 0.024 | 0.030 |
| Male | 4,366 | 4.35± 3.16 |
SD: Standard deviation; p-value obtained from Mann-Whitney test; r: Effect size.
Finally, the sample was grouped according to the number of DS reported by athletes and divided according to the sample collection period, gender and the type of sport (Table 5).
Table 5. Athletes who reported the consumption of different number of Dietary Supplement (DS) and divided according to the period of sample collection, gender and the type of sport.
| Quantity of DS used | Freq | % | Period of sample collection | Gender | Sport type | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| In competition | Out of Competition | Male | Female | Olympic | Paralympic | |||||||||
| Freq | % | Freq | % | Freq | % | Freq | % | Freq | % | Freq | % | |||
| 1 | 1,211 | 16.6 | 904 | 17.5 | 307 | 14.5 | 711 | 16.3 | 500 | 17.1 | 970 | 16.7 | 241 | 16.3 |
| 2 | 1,111 | 15.2 | 807 | 15.6 | 304 | 14.3 | 680 | 15.6 | 431 | 14.7 | 874 | 15.0 | 237 | 16.1 |
| 3 | 1,138 | 15.6 | 820 | 15.9 | 318 | 15.0 | 717 | 16.4 | 421 | 14.4 | 925 | 15.9 | 213 | 14.5 |
| 4 | 986 | 13.5 | 699 | 13.5 | 287 | 13.5 | 603 | 13.8 | 383 | 13.1 | 782 | 13.4 | 204 | 13.8 |
| 5 | 747 | 10.2 | 525 | 9.0 | 222 | 10.5 | 479 | 11.0 | 268 | 9.2 | 609 | 10.5 | 138 | 9.4 |
| 6 | 590 | 8.1 | 436 | 8.4 | 154 | 7.3 | 350 | 8.0 | 240 | 8.2 | 466 | 8.0 | 124 | 8.4 |
| 7 | 451 | 6.2 | 314 | 6.1 | 137 | 6.5 | 243 | 5.6 | 208 | 7.1 | 370 | 6.4 | 81 | 5.5 |
| 8 | 274 | 3.8 | 170 | 3.3 | 104 | 4.9 | 155 | 3.6 | 119 | 4.1 | 218 | 3.7 | 56 | 3.8 |
| 9 | 222 | 3.0 | 150 | 2.9 | 72 | 3.4 | 125 | 2.9 | 97 | 3.3 | 168 | 2.9 | 54 | 3.7 |
| 10 | 137 | 1.9 | 87 | 1.7 | 50 | 2.4 | 69 | 1.6 | 68 | 2.3 | 104 | 1.8 | 33 | 2.2 |
| 11-15 | 334 | 4.6 | 204 | 3.6 | 130 | 6.1 | 200 | 4.6 | 134 | 4.6 | 259 | 4.5 | 75 | 5.1 |
| 16-20 | 70 | 1.0 | 42 | 0.7 | 28 | 1.3 | 28 | 0.6 | 42 | 1.4 | 54 | 0.9 | 16 | 1.1 |
| 21-30 | 19 | 0.3 | 13 | 0.1 | 6 | 0.3 | 6 | 0.1 | 13 | 0.5 | 17 | 0.3 | 2 | 0.1 |
| Total | 7,290 | 100 | 5,171 | 100 | 2,119 | 100 | 4,366 | 100 | 2,924 | 100 | 5,816 | 100 | 1,474 | 100 |
Freq: Frequency.
DISCUSSION
This study analysed DS consumption among Brazilian athletes from Olympic and Paralympic disciplines, considering gender, the period of consumption (in or out of competition), and the number of supplements reported as consumed from 2015 to 2022, encompassing a total of 10,190 DCFs.
To the best of our knowledge, this is the first study to outline the DS consumption profile of a large sample of high-performance Brazilian athletes. It addresses a critical knowledge gap and offers insights that can help nutritionists, sports managers, and anti-doping educators in directing their efforts more effectively.
Maughan, Shirrefs et al. (2018) stressed that DS use should be supported by scientific evidence demonstrating performance and health benefits, mainly for elite athletes subject to doping control. Such caution is essential due to the risk of product contamination (Martínez-Sanz et al., 2017) and the strict liability policy enforced by the World Anti-Doping Agency (2021). Despite these risks, 71.54% of the athletes in this study reported DS use, and among these, 560 DCFs (7.68%) reported consuming more than 10 DS, and 19 DCFs reported the use of over 20 different DS.
The overall percentage of DS consumption aligns with findings from other studies, as noted by Knapik et al. (2016). However, when examining the quantity of DS used, this study revealed that Brazilian athletes who reported DS consumption had an average of 4.47 DS per athlete. In contrast, Norwegian athletes reported an average consumption of 2.24 DS (Lauritzen & Gjelstad, 2022), while U.S. endurance athletes of a similar age showed an average consumption of 2.7 DS (Graybeal et al., 2023). A similar average was found among Brazilian recreational triathletes, who reported 4.4 DS per athlete (Oliveira et al., 2024).
The literature, including the International Olympic Committee’s position statement on dietary supplements (Maughan, Burke et al., 2018), does not define a maximum number of DS an athlete should consume. Nevertheless, consuming more than 10 DS appears to present an excessive and unnecessary risk. The apparent lack of adherence to a behaviorally informed approach (Backhouse, 2023) or triple assessment, as proposed by Lauritzen and Gjelstad (2022), among Brazilian athletes may reflect a lack of information and education on this subject. Moreover, Brazil, like many other countries, does not have a third-party certification program, leaving athletes vulnerable to the risks associated with unregulated DS (Jagim et al., 2023).
Contrary to Lauritzen and Gjelstad’s (2022) findings, this study observed variations in DS consumption throughout the years, with significantly higher consumption during Olympic years (2016 and 2021). This trend is likely linked to athletes’ heightened focus on performance enhancement during these periods, as suggested by Dietz et al. (2014). This rationale may also explain the significant differences in DS use based on the competition period, with higher prevalence during in-competition periods compared to out-of-competition periods (as detailed in Table 3). Interestingly, the number of DS consumed was higher during out-of-competition periods, suggesting that some athletes reduce or stop certain DS out of fear of testing positive for prohibited substances.
Table 3 also highlighted significant differences in DS use between male and female athletes. The literature suggests that these differences are more closely associated with the type of sport or supplement than gender itself (Isenmann et al., 2024). However, our study found not only a higher prevalence of DS use among female athletes but also a significantly greater number of DS consumed. While physiological demands are similar for both genders, specific nutritional needs, such as iron supplementation to compensate for blood loss during menstruation (Pengelly et al., 2024), may explain this discrepancy. This pattern mirrors findings in the general Brazilian population (Pavlak et al., 2024). Preventive strategies, such as addressing the female athlete triad (Nattiv et al., 2007), may also play a role. Further research is necessary to explore whether Brazilian female athletes face a heightened anti-doping risk due to their DS use.
No significant differences in DS use or prevalence were observed between Olympic and Paralympic athletes. This result aligns with expectations, as their physiological demands and associated eating behaviours appear similar (Iwasa-Madge & Sesbreno, 2022).
Table 5 provides more detailed information, highlighting differences among groups, including the number of DS consumed. For instance, 31.5% of female athletes reported consuming six or more DS, raising concerns not only about doping risks and dietary quality but also about potential body dissatisfaction or disordered eating behaviours (Vardardottir et al., 2023). Similarly, 24.9% of athletes tested out of competition reported consuming seven or more DS. This group likely includes high-level athletes in Brazil’s Registered Testing Pool (ABCD), who are subject to more frequent testing (Equey et al., 2024). These findings raise questions about whether these athletes are receiving adequate nutritional education and information.
Despite certain limitations of this study, particularly the lack of identification of which athlete each analysed DCF belongs to, how many times an athlete may have been tested within the studied period, and whether their results were positive or not. Furthermore, as the information extracted from DCFs is self-reported, the athletes could omit or neglect information, voluntarily or not. In fact, this kind of situation has been reported previously by Garthe and Maughan (2018). However, this large cohort and extended timeframe provide valuable insights for the sports and anti-doping context.
CONCLUSIONS
A higher consumption of dietary supplements (DS) among female athletes, greater prevalence in competition situations, and a higher quantity of DS consumed out of competition were our main findings, with no differences observed between Olympic and Paralympic athletes. Overall, the results reveal a high prevalence and a very high amount of consumed DS among Brazilian athletes.
Further research is necessary to investigate the factors driving these findings. Additionally, greater attention should be given to educating athletes to ensure they make informed and conscious decisions, particularly as contaminated DS continue to pose significant risks to unwary or inattentive individuals

