











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
INTRODUCTION
Human skin (HS) plays a direct role in the heat exchange process between the body and its surrounding environment. Through the activation of thermal receptors, the human body identifies different environmental conditions such as cold or heat and generates an adaptive physiological response, which can be autonomic (e.g., vasoconstriction and vasodilation) or behavioral (e.g., seeking cooler places, fluid intake, and reduction of workload) (Charkoudian, 2016; Flouris & Schlader, 2015). Furthermore, when exposed to high ambient temperatures, the body increases cutaneous blood flow to promote heat loss through convection. In contrast, during exposure to cold, cutaneous blood flow is reduced to conserve body heat and prevent hypothermia (Cramer & Jay, 2016). Thus, skin temperature (ST) is tightly regulated by changes in cutaneous blood flow, increasing with higher blood flow and decreasing with lower blood flow (Ootsuka & Tanaka, 2015).
Accurate, continuous, and practical ST monitoring has emerged as an indispensable tool in various fields. In the prevention of heat-related illnesses, it facilitates the early detection of heat stress, enabling effective interventions and reducing the risk of hyperthermia (Taylor et al., 2014). In clinical settings, it supports the management of thermoregulatory conditions during illness and surgical procedures, as well as contributing to the detection of skin and breast cancers (Arora et al., 2008). Furthermore, in sports science, it plays a crucial role in optimising performance and preventing injuries by allowing precise workload control and recovery management (Merla et al., 2010).
In this context, infrared thermography (IRT) is a practical tool for assessing heat exchange and identifying temperature changes associated with physiological responses. IRT is a measurement technique capable of recording the heat radiated by body tissues through a camera that detects a range of the spectrum imperceptible to the naked eye (Sherman et al., 1996). Some aspects, such as the lack of need for direct contact between the evaluator and the evaluated, low cost, and ease of application, make its use indispensable in certain sports contexts (Hildebrandt et al., 2012; Priego Quesada et al., 2017). One of the most common applications is estimating the local average skin temperature (LST) based on values recorded by the pixels captured by the camera (Formenti et al., 2018).
In sports, this technique enables the creation of individual thermal profiles, allowing for the monitoring of thermal changes that may indicate inflammatory processes or thermal overload. Increases in LST are also associated with inflammatory processes resulting from increased blood flow and cellular metabolic activity following a catabolic process (Santana et al., 2022). This process is considered a fundamental part of the recovery response, aiming to regulate and repair the affected muscle fibers (Freire & Van Dyke, 2013). Thus, understanding these thermal variations through IRT not only aids in performance monitoring but also provides insights into the inflammatory and recovery processes in athletes.
Building on these advantages, infrared thermography has been increasingly employed to study specific body regions prone to thermal changes, such as the knee joint (Bagavathiappan et al., 2013). Variations greater than 0.5°C between contralateral regions are considered clinically significant, potentially indicating physiological or metabolic changes, such as localised inflammation or reduced blood flow (Selfe et al., 2008). Additionally, the anatomical characteristics of the knee influence its thermal distribution. The anterior region, which includes the patella, typically exhibits lower temperatures compared to the posterior region due to the direct thermal radiation emitted by the popliteal artery. Understanding these anterior-to-posterior thermal differences is crucial for monitoring training load and detecting early indicators of injury risk, particularly in athletes subjected to high physical demands (Alfieri et al., 2020; Fokam & Lehmann, 2019). Despite its potential, this type of analysis has been primarily explored in preliminary studies with specific athlete populations, highlighting the need for broader investigations across various sports and activity levels.
In this context, the present study aimed to address a significant gap in the literature regarding the thermal profiles of the knee region in individuals with differing physical activity levels. While previous research has largely focused on general body temperature responses to exercise, localised thermal patterns and their implications for injury prevention, performance monitoring, and rehabilitation remain underexplored. To bridge this gap, we hypothesized that: (1) athletes would exhibit higher average skin temperatures in the knee region compared to sedentary individuals, reflecting increased vascularization and metabolic activity associated with regular physical training; and (2) the posterior knee region would display higher temperatures than the anterior region in both groups, due to anatomical and vascular differences, such as the proximity of the popliteal artery. These hypotheses are supported by prior evidence indicating that localised thermal patterns can reflect training adaptations and vascular characteristics, offering valuable insights into physiological and biomechanical processes (Alfieri et al., 2020; Selfe et al., 2008).
This study specifically analysed and compared the average skin temperature of the knee region between athletes and sedentary individuals to explore how physical activity and training influence localised temperature regulation. Additionally, it sought to evaluate temperature differences between the anterior and posterior regions of the knee, providing a detailed understanding of training-induced adaptations and their practical applications in optimising training and recovery protocols.
METHODS
Sample
This study followed a cross-sectional observational design to compare the skin temperature of the knee region between athletes and sedentary individuals. A convenience sample consisted of 32 male participants. Of 16 athletes (age: 24.0 ± 3.6 years; height: 1.79 ± 0.06 m; body mass: 73.29 ± 11 kg; body mass index (BMI): 22.84 ± 2.52 kg/m²), elite men’s soccer players from second division of Brazilian football and compete in competitions organized and/or recognized by the Brazilian Football Confederation (CBF) with at experience in systematized soccer training and 16 sedentary individuals (age: 22.5 ± 3.3 years; height: 1.71 ± 5.3 m; body mass: 71.7 ± 11 kg; BMI: 24.5 ± 0.39 kg/m²). Participants were included if they were male and had no physical disorders or conditions that would affect their participation. Individuals were excluded if they had a history of knee injuries, recent surgeries, or any musculoskeletal conditions that could influence skin temperature or physical performance.
This study complied with all standards established by the National Health Council (Resolution 466/2012) regarding research involving human beings. All volunteers (or their legal guardians) signed the Free and Informed Consent Form after explanations about the procedures and possible risks involved in the research.
Experimental procedures
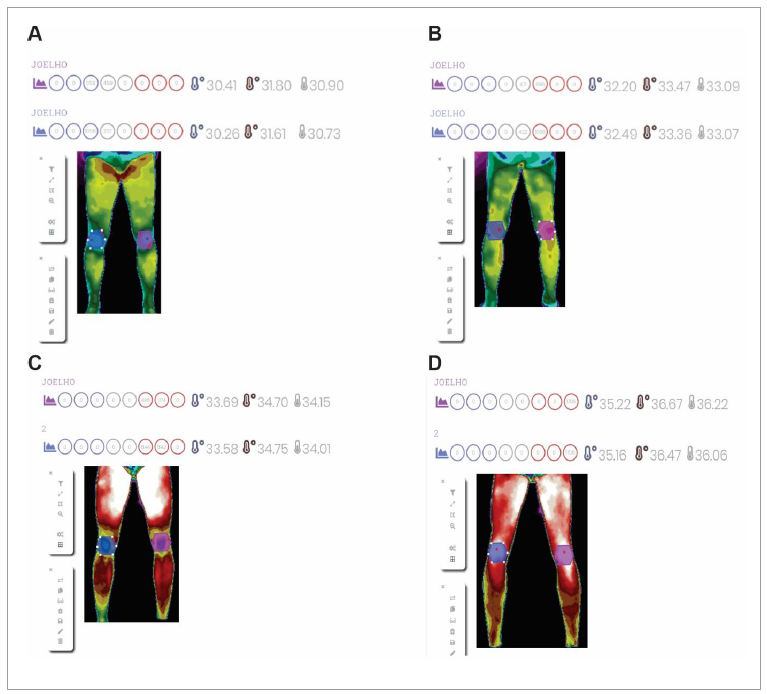
For the collection of thermographic images, the subjects were instructed not to perform vigorous activities in the 48 hours prior to the procedures, not to consume alcohol or caffeine, and not to use any type of skin cream in the 6 hours prior to the evaluation (Fernandes et al., 2017). Further instructions included avoiding sunbathing and physiotherapy treatments (e.g., massages or cryotherapy)- all recommendations aimed to minimise any influence on Tsk measurements (Moreira et al., 2017). To obtain the images, the volunteers remained at rest for 10 minutes inside an air-conditioned room to achieve thermal equilibrium (Marins et al., 2014). These images were captured by a FLIR T650sc camera (accuracy: ± 1.0°C, sensitivity: < 0.02°C; resolution: 640 × 480; temperature range: -40 to 2,000°C; spectral range: 7.5-14 μm; FLIR System Inc. Model, Sweden). Before the thermographic images were collected, the IRT camera was calibrated by entering ambient temperature (20-22°C), relative humidity (RH, 55-60%) and emissivity (ε = 0.98) (Fernández-Cuevas et al., 2015; Moreira et al., 2017). To analyse the images, the average values of the anterior and posterior regions of the knee (RCI) were considered, using APOLLO software (APOLLO®, v. 1.0, OMNI, Brazil). A representative example of how the analyses were conducted is shown in Figure 1.
Statistical analysis
Data normality was assessed using the Kolmogorov-Smirnov test. To compare the anterior and posterior regions within each group, a paired t-test was performed. For overall group comparisons of knee temperatures, one-way ANOVA was applied, followed by Tukey’s post hoc analysis. The effect size for paired comparisons was measured using partial eta squared (η²p), and for overall differences between groups, eta squared (η²) was used. The following cutoffs were considered: ≤ 0.10 (small), ≥ 0.25 (medium), and ≥ 0.40 (large) according to Cohen’s guidelines. All analyses were performed using GraphPad Prism software (GraphPad Software, San Diego, CA), version 10.4.1. A 5% significance level was established for all tests.
RESULTS
Table 1 presents the means and standard deviations of knee joint temperatures in athletes and sedentary individuals, highlighting the anterior and posterior regions on both the right and left sides. In sedentary individuals, the posterior region showed higher temperatures compared to the anterior region on the right side (p < .001; partial η² = .93) and the left side (p < .001; partial η² = .92). The same pattern was observed in athletes, with the posterior region displaying higher temperatures on the right side (p < .001; partial η² = .88) and the left side (p < .001; partial η² = .85). Additionally, the mean difference between the anterior and posterior regions was greater in sedentary individuals, with differences of 1.90°C on the right side and 1.72°C on the left side, compared to athletes, who showed differences of 1.51°C on the right side and 1.44°C on the left side.
Table 1. Temperature patterns of the anterior and posterior regions of the knee in athletes and sedentary individuals, with differences between the right and left sides.
| Sedentary | Athletes | |
|---|---|---|
| RKP | 32.18 ± 0.73* | 33.47 ± 1.05* |
| RKA | 30.28 ± 0.77 | 31.96 ± 1.07 |
| Difference | 1.90 | 1.51 |
| LKP | 32.28 ± 0.81# | 33.40 ± 0.89# |
| LKA | 30.56 ± 0.97 | 31.96 ± 1.10 |
| Difference | 1.72 | 1.44 |
RKA: Right knee anterior; RKP: Right knee posterior; LKA: Left knee anterior; LKP: Left knee posterior; *p < .05 vs. RKA; # p < .05 vs. LKA.
Figure 2 compares temperatures between athletes and sedentary individuals in both the anterior and posterior regions of the knee. In the posterior region, the athlete group also showed significantly higher temperatures, with differences noted on both the right side (p = .0006; η² = .33) and the left side (p = .0035; η² = .33). In the anterior region, athletes exhibited significantly higher temperatures compared to sedentary individuals on both the right (p < .0001; η² = .40) and left sides (p = .0009; η² = .40). These results highlight the influence of physical training on the elevation of knee temperatures, particularly in the posterior region.
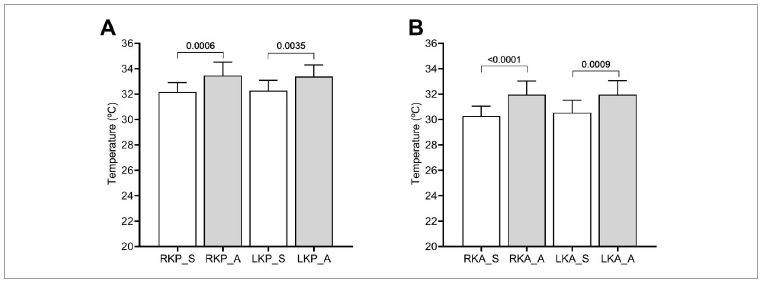
Figure 2. Comparison of knee temperatures between sedentary individuals and athletes. (A) Posterior knee region: Right knee posterior sedentary (RKP_S), Right knee posterior athlete (RKP_A), Left knee posterior sedentary (LKP_S), and Left knee posterior athlete (LKP_A). (B) Anterior knee region: Right knee anterior sedentary (RKA_S), Right knee anterior athlete (RKA_A), Left knee anterior sedentary (LKA_S), and Left knee anterior athlete (LKA_A). The p-values represent the statistical significance of the differences between groups.
DISCUSSION
The present study aimed to understand the thermal patterns associated with physical activity and training adaptations by analysing and comparing the average skin temperature in the knee region between athletes and sedentary individuals. It also sought to evaluate thermal differences between the anterior and posterior knee regions in both groups. The results demonstrated that the posterior knee region exhibited higher temperatures compared to the anterior region, in both groups analysed. Additionally, it was found that athletes displayed significantly higher average knee temperatures than sedentary individuals.
When assessing thermal symmetry, this study did not identify significant differences between knees or between the examined areas. The observed thermal asymmetry was classified as normal and acceptable, as the recorded differences were below .5°C. This value is widely recognised in the literature as a criterion to distinguish clinically relevant asymmetries, confirming the absence of pathological alterations in the evaluated sample (Rezende et al., 2024; Selfe et al., 2008; Vardasca et al., 2012).
The differences observed between the anterior and posterior regions of the knee can be explained by the specific anatomical and functional characteristics of each area. The higher temperature in the posterior region, identified in both groups, is associated with its more extensive vascularisation, particularly due to the proximity of the popliteal artery, whose thermal radiation is directly conducted to the skin. On the other hand, the anterior region is predominantly composed of the patellar bone structure, which acts as a thermal barrier, resulting in lower temperatures in this area (Rezende et al., 2024; Selfe et al., 2008). This thermal distribution pattern reflects normal conditions of the knee’s anatomical structures and can be considered an indicator of their good functional state. Moreover, the thermal difference between the anterior and posterior regions is consistent with findings reported in preliminary studies on female soccer players, which also observed lower temperatures in the anterior region due to the presence of the patella (Stroppa et al., 2017).
The results indicated that athletes exhibited significantly higher average skin temperatures in the knee region compared to sedentary individuals. This difference can be explained by physiological adaptations resulting from training, such as increased vascularisation in tissues frequently engaged during sports practice (Di Francescomarino et al., 2009; Roseguini & Laughlin, 2019). Additionally, intense muscular activity and microlesions caused by training may trigger mild inflammatory processes that increase local heat release (Cerqueira et al., 2020). These changes reflect the body’s adaptive capacity to the continuous physical demands and mechanical impact of athletic activities.
Finally, this study presents some limitations. First, the small sample size, comprising only 32 participants, limits the generalisability of the results to broader populations or those with different characteristics, such as women and elite athletes. Additionally, the thermography method, although practical and non-invasive, is sensitive to external factors such as the participants’ hydration status and basal temperature, which were not rigorously controlled and may have influenced the results. Furthermore, the decision to evaluate athletes during the pre-season, a period characterised by increased training loads and potential inflammation, may have accentuated the observed effects. Future studies should consider assessing athletes in different training phases to better generalise findings across various contexts. Lastly, the study’s cross-sectional design prevents the analysis of thermal changes over time and their relationships with training adaptation or inactivity, highlighting the need for future longitudinal investigations.
PRACTICAL APPLICATIONS
The findings of this study highlight the potential of infrared thermography as a practical tool in both sports and clinical contexts. In sports, it can be used to monitor training loads, detect early signs of overtraining or inflammation, and optimise recovery protocols by identifying localised thermal changes. Clinically, thermography may assist in assessing knee joint health, guiding rehabilitation strategies, and identifying abnormal thermal patterns that could indicate injury risks or underlying pathologies. These applications reinforce the value of this non-invasive technique in promoting performance and joint health.
CONCLUSIONS
In conclusion, the study revealed that athletes exhibited significantly higher average skin temperatures in the knee region compared to sedentary individuals. Furthermore, temperature differences were observed between the anterior and posterior regions of the knee in both groups, with the posterior region consistently showing higher values.

