











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
The intra‑osseous lesions that affect the maxillomandibular complex are mainly categorized into three groups: cysts, tumors, and bone‑related lesions.1 The latter are a group of lesions that share the same basic evolutionary mechanism and are characterized by the replacement of normal bone with a fibrous connective tissue that will gradually undergo mineralization. Although these lesions’ subtypes sometimes present similar microscopic characteristics, each group’s demographic, clinical, and radiological characteristics are unique.2
The World Health Organization (WHO) published the latest odontogenic and maxillofacial bone tumors classification in 2017. It referred to bone‑related lesions as the group of “bone tumors and related lesions,” which was subdivided into fibro‑and chondro‑osseous lesions, giant cell lesions, and bone cysts.3
The subgroup of fibrous and chondro‑osseous lesions includes ossifying fibroma, fibrous dysplasia, cemento‑osseous dysplasia, familial gigantiform cementoma, and osteochondroma.
These lesions present similar clinical characteristics, such as increased soft tissue volume and altered shape of the affected bones, leading to aesthetic and functional losses, like paresthesia and trismus. However, they can also be completely asymptomatic while being identifiable in radiographic examinations, where their appearance varies according to the stage of development. In the early stages, the lesions are radiolucent and well‑defined, while in advanced stages, they become radiopaque with poorly defined borders. Thus, they can be characterized as radiolucent, mixed, radiopaque, or with a ground‑glass appearance.4
The subgroups of giant cell lesions and bone cysts are composed of central giant cell granuloma, peripheral giant cell granuloma, cherubism, aneurysmal bone cyst, and simple bone cyst. Histologically, these subgroups’ lesions may present characteristics in common and sometimes disordered due to the presence of multinucleated giant cells. However, radiographic and clinical examinations are pathognomonic for the differential diagnosis of these lesions.5
A clinical‑pathological study on lesions affecting the jaws in the southern Iranian population carried out in 2017 found 1,121 intra‑ osseous lesions in the archive of the Department of Oral Pathology in a period of 22 years, comprising 25% of all cases. The group of lesions associated with the maxilla and mandible bones was the second most frequent (15.9% of all cases), with the highest prevalence for central giant cell granuloma (CGCG).1
Understanding bone‑related lesions that affect the jaws is fundamental for the dentist, who is responsible for the diagnosis and treatment of such diseases. When faced with the clinical characteristics of an injury and its epidemiological profile, the knowledgeable clinician will be capable of guiding their diagnosis toward the most frequent lesions. Thus, epidemiological data, besides contributing to the histopathological diagnosis, help with the prognosis, the therapeutic planning, and the patient’s follow‑up.
There has been a significant increase in epidemiological studies involving the classification of oral diseases, including demographic data. However, most of the studies available focus only on some groups of orofacial lesions, such as oral cancer and potentially malignant lesions, culminating in a lack of studies on intra‑osseous lesions, particularly bone‑relatedlesions.6
Unquestionably, epidemiological studies have significant relevance in understanding better the lesions that may occur in the stomatognathic system and the profile of the affected population. Therefore, this article intended to contribute to the literature on bone‑related lesions that may affect the jaws.
The current work aimed to identify the bone‑related lesions of the jaws biopsied in patients treated by the Reference Center for Oral Injuries of the State University of Feira de Santana (CRLB - UEFS) from 2006 to 2017, recognizing the three most frequent injuries and their clinical characteristics.
Material and methods
This cross‑sectional descriptive study used secondary data from the histopathological reports of patients living in Feira de Santana and proximities who sought assistance at the CRLB - UEFS spontaneously, from 2006 to 2017. The data was collected from conclusive histopathological reports of oral bone‑related lesions diagnosed by the CRLB - UEFS pathology laboratory between 2006 and 2017.
The CRLB - UEFS runs as a walk‑in clinic, receiving patients from Feira de Santana and all regional cities of the state of Bahia. All conclusive histopathological reports of any injury associated with the maxilla and the mandible recommended by the WHO (2017), from the 11‑year period, were included in the study. The exclusion criteria were descriptive histopathological reports with the same registry number (in cases where incisional biopsy of an extensive lesion was followed by total surgical removal of that lesion, the second report was considered) and with missing information on the variables studied.
Of the 2051 reports, including only 290 with a conclusive diagnosis, 65 were selected as fitting the criteria. All 65 conclusive histopathological reports of lesions associated with the jaws were evaluated, and the following data were extracted: histopathological diagnosis, patient’s gender and age, and anatomical location. The lesions had been diagnosed based on clinical and radiographic examination, as well as incisional biopsies of extensive lesions and excisional biopsies of smaller lesions, with the corresponding histopathological reports.
In surgical removal cases where a subsequent new histopathological report was performed with new analysis, the report’s numbering was maintained to avoid duplication.
Data were recorded in a specialized spreadsheet organized in columns. Only one examiner collected and recorded all data, after previous training and calibration by an experienced stomatologist based on reports analysis.
The variables considered in the study were the patients’ gender (female or male) and age, the lesion’s anatomical location (anterior mandible, posterior mandible, anterior maxilla, and posterior maxilla), and the histopathological diagnosis itself. Despite their relevance, variables like profession, smoking, and drinking were not considered due to not having been filled out on the report.
The data obtained were analyzed descriptively using Microsoft Office Excel Professional Plus Software, 2013. Frequency tables were used for qualitative variables, with their respective percentages. Regarding quantitative variables, the mean was adopted as a descriptive measure. The crude measure of association between the variables age (age group), gender, and anatomical location (maxilla versus mandible and anterior versus
posterior) was tested by bivariate analysis using the chi‑square, Cochran’s, and Mantel‑ Haenszel tests. The sample had to be dichotomized into two groups: bone‑related lesions and non‑bone‑related lesions (all intra‑osseous lesions - cysts, tumors, and periapical lesions).
Results
All 2,051 histopathological reports of oral lesions diagnosed by the pathology laboratory of the CRLB - UEFS between 2006 and 2017 were evaluated. Only 290 files had a conclusive histopathological diagnosis for some type of intra‑osseous lesion.
Of these, 65 were conclusive for bone‑related lesions of the jaws, representing 3.17% of the total lesions, with a ratio of 1:31.
These lesions occurred more frequently in female patients (81.54%) and affected mostly the posterior region of the mandible (53.85%) (Figure 1). The patients’ ages ranged from 10 to 77 years, with a mean age of 45.25 years. Within the female gender, the posterior mandible was still the most affected location, with 28 cases, followed by the posterior maxilla (12 cases), the anterior mandible (nine cases), and the anterior maxilla (four cases). The male gender, significantly less affected, showed slightly different frequencies considering locations: the posterior mandible was overall the most affected, with six cases, followed by the anterior mandible (three cases), the posterior maxilla (two cases), and the anterior maxilla (one case).
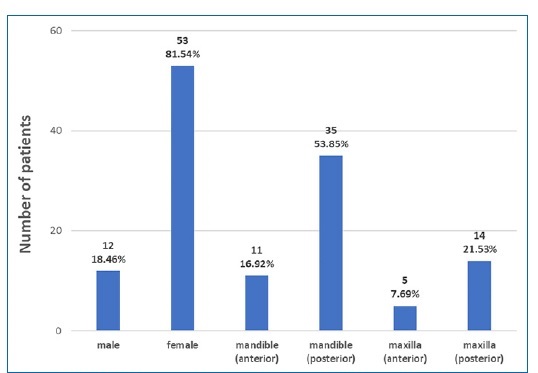
Figure 1 Absolute frequency of patients diagnosed with bone‑related lesions of the maxilla and the mandible, according to patients’ gender and lesions’ anatomical location. Feira de Santana, Bahia, Brazil, 2018 (n=65; 100%)
The bone‑related lesions of the jaws found in this study are described in Table 1. The most frequent were cemento‑osseous dysplasia, fibrous dysplasia, and ossifying fibroma, together representing 58 lesions of the total sample. Their clinical characteristics are described in Table 2 and Figure 2.
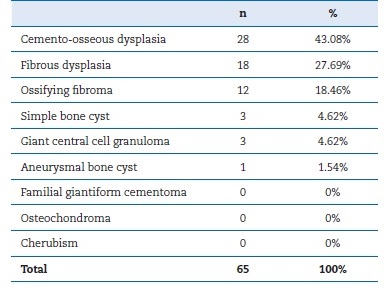
Table 1 Classification of bone‑related lesions of the maxilla by absolute and relative frequencies. Feira de Santana, Bahia, Brazil, 2018 (n=65).

Table 2 Distribution of mean age and absolute and relative frequency of gender of patients who had the three most frequent bone‑associated lesions of the jaws. Feira de Santana, Bahia, Brazil, 2018 (n=65).
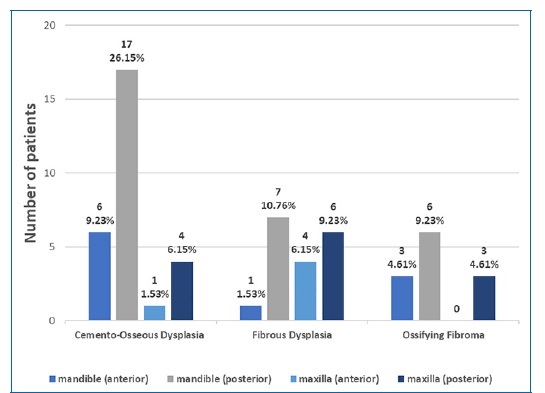
Figure 2 Absolute and relative frequency of the number of patients who had the most frequent bone‑associated lesions of the jaws, distributed according to the anatomical location. Feira de Santana, Bahia, Brazil, 2018 (n = 65)
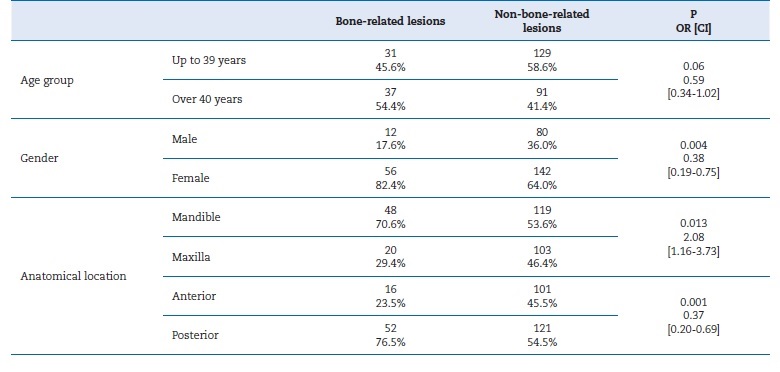
There was no association between the age group of the individuals investigated and the frequency of bone‑related lesions (p=0.06). The proportion of females was 82.4% in the group of individuals diagnosed with bone‑related lesions, against 64% in the group with other lesions; the measure of association showed that women were 62% more likely to have bone‑related lesions than other lesions (OR=0.38; CI [1.92‑0.75]). Bone‑related lesions were most frequent in the mandible (70.6% versus 29.4% in the maxilla) and the posterior region (73.5% versus 23.5% in the anterior region). The correlations between bone‑related lesions and the anatomical location regarding maxilla/mandible and anterior/posterior regions were statistically significant (p=0.013 and p=0.001, respectively). (Table 3).
Discussion
Bone‑related lesions in the maxillomandibular complex were present in 65 conclusive reports in this study, representing 3.17% of the total lesions biopsied in the CRLB - UEFS in this period, with an absolute frequency of 0.03. Jaafari and Akbari1 found a relative frequency of bone‑related lesions associated with jawbones of 15.9%, a value higher than that found in this study, which may be due to their collection period longer than 20 years.
The average age of patients was the variable with the greatest discrepancy within the literature. In this study, it was 45,23 years. Souto et al.,6 in a survey of 762 cases of maxillofacial lesions, had a patients’ mean age of 34 years. On the other hand, Jaafari and Akbari1 had an average age of 28 years. Thus, it is difficult to define a pattern among the average ages found by the studies. In the present study, the most prevalent cases were female patients with lesions in the posterior region of the mandible.
A higher frequency of females and mandibular involvement in patients with bone‑related lesions of the jaws were also described by Souto et al.6 and Jaafari and Akbari.1 This agreement can be justified not specifically due to it affecting more women, but possibly due to women being more aware of their health needs and possible alterations than men. This behavior causes women to seek healthcare more frequently, making these lesions more detectable and raising the number of cases in the female gender.
The most frequent lesions in this study were cemento‑osseous dysplasia, fibrous dysplasia, and ossifying fibroma.
The higher frequency of cemento‑osseous dysplasia can be explained by the significant demographic density of black women in the state of Bahia, Brazil, especially in the regions of Feira de Santana and Reconcavo Baiano, which have been influenced by slavery and afro‑descendants since the colonization of the country.7 Socio‑demographic aspects confirmed in the literature report the higher frequency of these cemento‑osseous dysplasias in black women.5,7
The most frequent bone‑related lesion associated with mandibular and maxillary bones differs among studies. In a study of intra‑osseous lesions detected in maxillary biopsies between 1998 and 2010, Jamshidi et al.8 found 52 bone‑related lesions associated with maxillary bones, of which CGCG was the most frequent (42.3%). Peker et al.,9 in a 5‑year retrospective study of biopsies of mandible lesions, reported that the most frequent bone‑related lesion was the ossifying fibroma. On the other hand, Jaafari and Akbari,1 in their clinicopathological study of intra‑osseous lesions in the southern Iranian population, found that CGCG was the most frequent, corresponding to 35.3% of the lesions associated with maxillary bones.
The clinical features of cemento‑osseous dysplasia found in this study were similar to the findings of Peker et al.,9 who reported a predominance of the female gender and posterior mandible regions in patients with this type of dysplasia. However, the age of patients with cemento‑osseous dysplasia varied considerably in most studies, as Muwazi and Kamulegeya,10 when investigating the prevalence of maxillofacial fibro‑osseous lesions in Uganda, found a mean age of 49 years, Raubenheimer, Noffke and Boy11 reported 35 years, and Peker et al.9 45 years.
The variables of the second most frequent lesion in this study, fibrous dysplasia, differed significantly from most articles available in the literature.1,4,8,12‑14However, Santos Neto et al.,2 when describing clinicopathological characteristics of 143 cases diagnosed with fibro‑osseous lesions, obtained results very close to those found in this study: mean age of 34 years and higher frequency in females and the posterior region of the mandible. On the other hand, Phattarataratip et al.,12 when performing a clinicopathological analysis of 207 cases of benign fibro‑osseous lesions of the jaw, reported a mean age of patients with fibrous dysplasia slightly lower than that of this study (25 years) and the posterior maxilla as the most affected location, but also found a higher occurrence in females.
The ossifying fibroma, the third most frequent lesion in this study, presented clinical characteristics similar to those found by Jaafari and Akbari,1 where females and the mandible were the most affected. These results differ from those by Mohanty et al.,15 who, when performing a retrospective analysis of the ossifying fibroma of the mandibular‑maxillary bones, reported a patients’ mean age of 24 years and males as the most affected gender. The posterior mandible region was the most affected in most of the studies found.2,4,9,10,12,14,15
According to the literature, few retrospective epidemiological studies have evaluated all lesions associated with the maxilla and mandible bones simultaneously. Generally, studies include only some of these lesions, such as bone dysplasia,11,13fibro‑osseous lesions,4,10,12 or ossifying fibromas.15In addition, most of the data on bone‑related lesions of the jaws come from retrospective studies, which are usually performed with data from histopathology laboratories; thus, some of these lesions are underreported.
Epidemiological surveys are a great indicator of the needs of a specific population (in this case, the Bahian population, mostly composed of brown or black individuals); thus, preventive and therapeutic actions derived from these should not be ignored by health professionals and government guidelines.
The inclusion of these oral lesions in the Health Department’s epidemiological bulletins, for example, can promote the implementation of preventive measures, as well as the training of professionals for an early and effective diagnosis and treatment, which can culminate in the reduction of costs and necessary health supplies.
Conclusions
Bone‑related lesions of the jaws biopsied in the CRLB - UEFS between 2006 and 2017 had a ratio of 1:31. The lesions studied affected mostly women and the posterior region of the mandible, and patients had a mean age of 45.2 years. The most common histopathological diagnosis was cemento‑osseous dysplasia, followed by fibrous dysplasia and ossifying fibroma.

