











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The success of endodontic treatment depends on the clinician’s effectiveness in accomplishing microbial load reduction within the root canal system (RCS).1 This is achieved by chemo-mechanical preparation and temporary intracanal medication.
Calcium hydroxide paste (Ca(OH)2) is the most commonly used intracanal medication due to its antimicrobial effect induced by increasing the pH inside the RCS, which compromises the integrity of the cytoplasmic membrane.2 Furthermore, Ca(OH)2 can hydrolyze the lipid portion of bacterial lipopolysaccharides and mitigate the periapical tissue’s inflammatory response.3 However, complete removal of the Ca(OH)2 paste before root canal filling is paramount to achieving adequate sealing of the RCS for a successful endodontic treatment.4 Current clinical protocols pose limitations to this goal, especially in the RCS’s apical third, where removal has been deemed difficult.5-9
Nowadays, the sodium hypochlorite solution (NaOCl) is considered the gold standard for irrigation,2 both in chemo- mechanical preparation and Ca(OH)2 removal, but correct delivery and agitation play a crucial role in its efficacy.10 Manual dynamic irrigation (MDI) is an accessible way to improve the distribution of irrigants throughout the RCS compared to conventional manual irrigation.11 Agitation can be further promoted with passive ultrasonic irrigation (PUI), which induces acoustic microstreaming (> 25 kHz) due to a transverse vibration,12 enhancing shear stress on RCS remnants.13 Another option is the machine-assisted device CanalBrush™ (Coltène Whaledent, Langenau, Germany), a small rotary brush made from polypropylene that is highly flexible and can displace debris.10 Lastly, the XP-endo Finisher® (FKG Dentaire, La Chaux-de-Fonds, Switzerland) was recently introduced as na enhancer of cleanliness and disinfection thanks to its extreme flexibility and capacity for expansion based on the principles of shape memory and the metallurgical phase transition of nickel-titanium alloys.14
Various irrigant activation systems have been tested in Ca(OH)2 removal from the RCS;8,14-17 however, which is the most appropriate protocol is still debatable. Therefore, the aim of this in vitro study is to evaluate the efficacy of CanalBrush™, E1® - Irrisonic tip (Helse Utrasonic, São Paulo, Brazil), XP-endo Finisher®, and MDI in the removal of Ca(OH)2, using radiographic and photographic methods. The following three null hypotheses were formulated: (I) none of the systems presents 100% efficacy in the removal of intracanal medication, (II) the performance of the several systems is similar, without significant differences between them, and (III) the results of the two evaluation methodologies are not comparable to each other.
Material and methods
The project was approved by the Institutional Ethics Committee of the University Fernando Pessoa. Based on previous studies,5,16-19sixty permanent single-root teeth previously extracted for orthodontic or periodontal reasons were selected. Exclusion criteria included teeth with immature apices, previous root canal filling, internal or external resorption, or vertical or horizontal fractures.
Preoperative mesiodistal and buccolingual radiographs were taken to verify exclusion criteria and analyze RCS diameters. Central and lateral maxillary incisors, canines, and premolars were included. The selected teeth exhibited apical curvatures of up to 15°, according to Schneider’s method,20 and had similar RCS mesiodistal and buccolingual diameters. A single investigator (GE) conducted all the procedures to eliminate interoperator variability.
Endodontic access cavities were prepared underwater using a round diamond bur and an Endo-Z bur (Dentsply Malleifer, Ballaigues, Switzerland) mounted on a high-speed handpiece. The working length (WL) was established by inserting an ISO 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) until its tip was visible at the apical foramen and then subtracting 1 mm.
Teeth were prepared using ProTaper Gold® rotary instruments (Dentsply Maillefer) up to F3 (30.09). Between each file, the RCS was irrigated with 2 mL of a 2.5% NaOCl solution using a syringe and a 27-G needle (Coltène/Whaledent©, Langenau, Germany) placed 1-mm short of the WL. Afterward, a final irrigation protocol was carried out with 10 mL of 17% EDTA and 10 mL of 2.5% NaOCl for 1 minute each, and 3 mL of 70% ethyl alcohol, after which the RCS was dried with ProTaper® paper points F3 (Dentsply Maillefer). Then, root molding was made with silicone cubes (Turboflex Putty R&S, Dentaleader, Tremblay-en-France, France).
Teeth were cut into two halves: vestibular and palatine/lingual. To ensure that the precision saw cut would include the apical foramen and the saw arms would not cause tooth damage, bis-acrylic resin (Structur 3, Voco, Cuxhaven, Germany) was applied around the crown to support the precision saw arms. A longitudinal groove was created with a diamond band cutting system (EXAKT Pathology Precision Saw, EXAKT Technologies, Norderstedt, Germany) on the mesial and distal surfaces until RCS penetration occurred. The resin was then removed, and the halves were separated with a cement spatula.
To simulate the non-instrumented irregular portions of the RCS, the sample was then processed as described in previous studies:12-14,16longitudinal grooves of 0.5-mm deep, 0.2-mm wide, and 3-mm long were made with a diamond inverted cone drill HP807/023PF (Strauss Diamond Instruments, Inc.©, Palm Coast, USA).12,16,17 A graduated ruler was used to create a groove in each half: one in the apical portion of one half and another in the coronal portion of the other (Figure 1). Ca(OH)2 paste (Cerkamed©, Stalowa Wola, Poland) was applied inside all grooves with a dental excavator and an endodontic probe and then condensed with a moistened cotton pellet (Roeko Cotton Pellets #1, Coltène/Whaledent©, Langenau / Germany) to ensure uniform distribution.
The complete filling of the grooves was evaluated with a radiograph obtained using the CS 2100 Carestream Dental® device (Carestream Health, New York, USA) and a photograph captured by an SLT-A35 camera® (Sony Corporation, Tokyo, Japan) according to standardized image settings (manual mode, ISO 800, and 300 mm focal distance). Then, both halves were pooled in the silicone mold, and the access cavities were sealed with a sterilized cotton pellet ball and CavitTM (3M ESPE, Germany). The teeth were stored in an incubator (Binder Drying Oven ED 115, BINDER GmbH©, Tuttlingen, Germany) at 37°C and 100% humidity for 14 days to simulate a clinical situation between treatment sessions.
The teeth were divided into four groups (n=15), each consisting of three central maxillary incisors, three lateral maxillary incisors, three canines, and six premolars. The groups corresponded to the experimental irrigation device/method tested: the CanalBrush™ ISO 30.04 in Group 1, the E1 - Irrisonic tip coupled to an ultrasound unit (Advance 2 Digital Ultrasound, Microdont, São Paulo, Brazil) in Group 2, the MDI i Group 3, and an ISO #25 XP-endo Finisher® file coupled to na endodontic motor (Dentsply Maillefer®, Ballaigues, Switzerland) in Group 4. The corresponding procedures are described below. Before the testing irrigation procedures, a glide path was established in all teeth with an ISO K10 file placed at WL plus 1 mm after root canal irrigation with 2.5 mL of 2.5%

NaOCl using a syringe and a 27-G needle (Coltène/Whaledent ©, Langenau, Germany) placed 1-mm short of the WL. Then, 2.5 mL of 2.5% NaOCl at 20°C were delivered, interspersed with the application of the device tested. The procedure was repeated until a total of 10 mL of 2.5% NaOCl was reached in a total irrigation time of 1 minute.
In Group 1, a CanalBrush™ ISO 30.04 rotating clockwise at a speed of 600 rpm was applied with in-and-out movements up to 1-mm short of the WL for 20 seconds. In Group 2, the E1 - Irrisonic tip, coupled to an ultrasound unit, was operated at a power of 10 W and then inserted with in-and-out movements up to 1-mm short of the WL for 20 seconds. In Group 3, the irrigant solution was interspersed with manual agitation of a ProTaper® F3 gutta-percha point (Dentsply Maillefer®, Switzerland), with each point being inserted with shuttle movements up to 1-mm short of the WL for 20 seconds. Finally, in Group 4, the XP-endo Finisher® file coupled to an endodontic motor (Dentsply Maillefer®, Ballaigues, Switzerland) was operated at a speed of 800 rpm and a torque of 1 Ncm, inserting the file 1-mm short of the WL with smooth movements in a longitudinal direction for 20 seconds.
In the end, to assess Ca(OH)2 removal, all RCSs were dried with ProTaper® F3 paper points (Dentsply Malleifer, Ballaigues, Switzerland). The tooth halves were immediately separated to be photographed and radiographed again as previously described. Two blinded and previously calibrated investigators (AMT, GE) assessed independently and qualitatively the amount of Ca(OH)2 residues in all grooves according to an ordinal scoring system where lower values represented better cleaning results (Figure 2).17
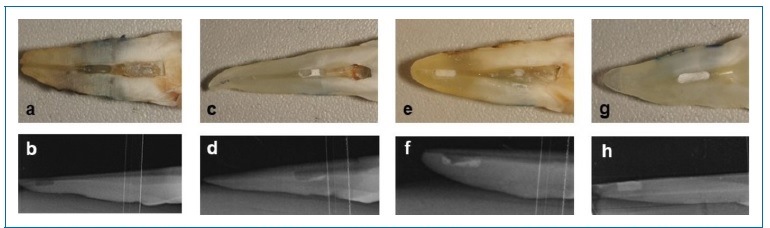
Figure 2 Representation of the scores used in the survey. (a,b) Score 0: Groove empty, without debris; (c,d) Score 1: Groove with debris in less than 50% of the total area; (e,f) Score 2: Groove with debris in more than 50% of the total area; (g,h) Score 3: Groove completely filled with debris
Data were analyzed using Cohen’s kappa. Values to determine the degree of inter-observer agreement for each method of observation. Non-parametric tests were chosen because of the Gaussian distribution first tested. The differences in scores between the different experimental groups were analyzed using the Kruskal-Wallis test. The Mann Whitney U test (with Bonferroni correction for multiple comparisons) was used for multiple comparisons between groups. A value of p<0.05 was considered statistically significant. The correlation between the radiographic and photographic analysis was determined using Spearman’s correlation coefficient. Statistical analysis was performed using the R system (version 3.4.2).21
Results
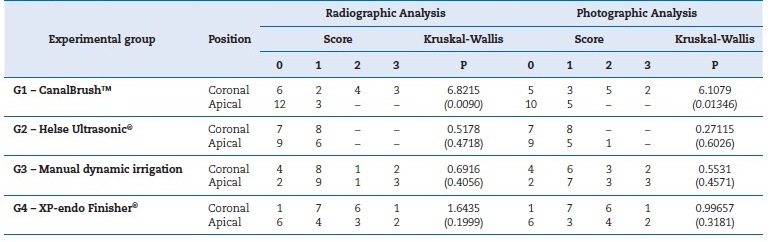
None of the tested irrigant activation systems removed the Ca(OH)2 completely from all the coronal and apical grooves (Table 1). Considering the position of the groove, none of the techniques demonstrated differences in the efficacy of Ca(OH)2 removal between the coronal and apical regions, except for CanalBrush™, which performed significantly better in the apical third (p<0.05). Therefore, the first null hypothesis was accepted, and the second was rejected.
Table 1 Scoring results and Kruskal-Wallis tests comparing the efficiency of calcium hydroxide removal on apical and coronal grooves by different irrigant activation techniques. The removal efficiency was evaluated by two distinct methods: photography and radiography. For each comparison between coronal and apical scores, the Kruskal-Wallis test’s statistics are provided (depicted in bold) with the respective p value within parenthesis (significant tests, with p<0.05, are depicted in italics).
The scores attributed independently by the two observers presented significant agreement, with kappa values of 0.91 and 0.92 for the radiographic and photographic methods, respectively.
Accordingly, only data from one of the evaluators were used for statistical analysis. The correlation between the radiographic and photographic analyses was significant (r=0.9547, p<0.05), suggesting a high degree of agreement between both methods. Thus, the third null hypothesis was rejected.
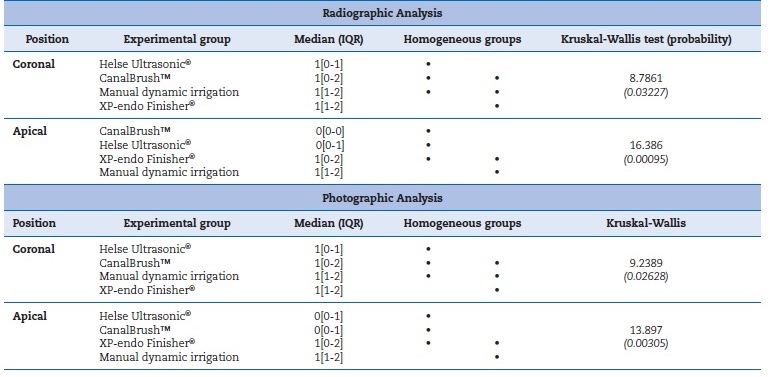
As shown in Table 2, the Kruskal-Wallis test revealed statistically significantly (p<0.05) superior efficacy of E1 - Irrisonic tip and CanalBrush™ compared to XP-endo Finisher® and MDI for both grooves. The two most effective techniques (CanalBrush™ and E1 - Irrisonic tip) in the apical region differed significantly and consistently from the least eficiente removal technique - MDI - in both radiographic and photographic analyses. Regarding the coronal region, E1 - Irrisonic tip was always statistically significantly better (p<0.05) than XP-endo Finisher® in both analyses. Qualitatively, the E1 - Irrisonic tip showed the best efficacy since its scores seldom exceeded one (Table 1).
Table 2 Multiple comparison tests for differences in calcium hydroxide removal between different irrigant activation techniques according to the paste’s position in the root canal system (apical and coronal). The removal efficiency was evaluated by two distinct methods: photography and radiography. For each position (apical or coronal), techniques yielding non-different results are denoted by dots in the same column (homogeneous subsets of medians).
Discussion
In the present study, the more routinely used photographic analysis was complemented by a radiographic technique, as suggested by Küçükkaya et al.,22 to better depict the outcome as both approaches are two-dimensional and, thus, any possible distortions depending on the position of the debris could be mitigated. Since there were no significant diferences between the methods, both confirmed the results and contributed to their validation. The micro-CT would be a more reliable method capable of distinguishing empty spaces and dental structures, allowing a high-precision quantitative and qualitative assessment of residues; however, this methodology could not be applied for financial reasons.
Nonetheless, the more classical methods adopted are valid and reliable, especially if combined, as they give greater credibility to the results. Even though the longitudinal groove model does not replicate the whole anatomical complexity of the RCS, it has a key advantage: the standardization of measurements and locations, as well as the application of an equivalent volume of Ca(OH)2, improving the internal validity of the study.5,16,17
Moreover, the scoring scale17 adopted is more reproducible when restricted to a groove than when applied to a wider area, such as the full extent of the RCS.16
The Ca(OH)2 condensation after application on the groove is not feasible in a clinical situation but was performed to improve the standardization and comparison between the techniques tested. With this procedure, we ensured that all grooves had the same quantity of the intracanal medication and, as in the pilot study where we compared the two options - condensed Ca(OH)2 vs. non-condensed - by a simple application without pressure, radiographically it seemed that all grooves were full and photographically it was possible to see empty spaces inside.
The inter-observer agreement and intra-observer reproducibility showed good results with no statistically significant differences between observers and results for cleanliness. No control groups were used, as in other literature,19 because they would only serve as a means of comparison between the complete filling or the absence of Ca(OH)2 within the groove.
The tooth’s crown was not removed to prevent tooth weakness. Each tooth’s root canal longitude was calculated, and its cross-section was assessed by the two different incidences of the preoperative radiographs. This methodology provided data for a similar teeth distribution in all test groups, thus assuring an accurate sample selection.
Our results agree with previous studies reporting that complete removal of Ca(OH)2 was not achieved with any of the available techniques.2,3,8,14,15,23,24Pabel and Hulsmann16 verified that CanalBrush™ and PUI using NaOCl significantly removed more Ca(OH)2 than conventional manual irrigation, with PUI being significantly superior in coronal and apical grooves. Another study23 that assessed the entire RCS and applied 2.5% NaOCl alone or with 17% EDTA using CanalBrush™, PUI, and a master apical file observed that the type of irrigant did not influence the amount removed, with CanalBrush™ and PUI being statistically better than the master apical file. A more recent study24 tested 17% EDTA combined with 2.5% NaOCl in oval RCSs with conventional manual irrigation, PUI, and Easy Clean® and concluded that conventional manual irrigation was the least efficient, while Easy Clean® and PUI were similar.
In the RCS thirds’ analysis, Easy Clean® was more eficiente than conventional manual irrigation in all of them, while PUI was superior only in the cervical third. Considering the removal of Ca(OH)2 as the primary goal, the choice between NaOCl alone or associated with a chelating agent may act as a minor variable, since, in clinical practice, before the filling stage, it is strongly recommended to perform a final flush with a chelating solution, such as EDTA, followed by NaOCl - a rational and simple protocol.25 Thus, the presente study used NaOCl alone. Future research could test whether the association of NaOCl with a 17% EDTA solution promotes different results.
The present study showed that, though none of the methods completely removed all Ca(OH)2 from all grooves, CanalBrush™ or E1 - Irrisonic tip performed better. In contrast, one study that applied Ca(OH)2 into the whole RCS verified that CanalBrush™ was ineffective in the apical zone because it induced the detachment of residues into it and their consequente impaction.4 Similarly to the present study, another one concluded that CanalBrush™ and the Vibringe® system (Vibringe BV Corp, Amsterdam, Netherlands) exhibited lower scores than MDI, but the difference was not statistically significant.19 However, unlike our study, they found a significant difference between sections of the RCS, with Ca(OH)2 removal being most difficult in the apical region, except for the CanalBrush™ group. Ultrasonic irrigation’s efficacy is undeniable,21,24 through the effects of cavitation and acoustic vibration produced in the irrigation solution from the apical to the coronal sections.1,18
Regarding the apical groove, PUI was significantly more effective than XP-endo Finisher®, but there were no significant diferences in the coronal groove.5,26 This study’s results showed statistically significant diferences between E1 - Irrisonic tip and XP-endo Finisher® in both regions, with E1 - Irrisonic tip performing better. This finding disagrees with a previous study.27 In fact, the published results concerning the efficacy of XP-endo Finisher® in intracanal medication removal are controversial. The specific technical characteristics of this file, namely, the potential influence of the irrigant and experimental setting temperature on the NiTi alloy phase, may explain the different findings. Although these instruments are relatively straight in their M phase (martensitic state) at room temperature, they change to a curved shape when exposed to intracanal temperature because of a phase transformation to the A phase (austenitic state).28 Similar to the present study, another one26 attempted to standardize experimental conditions, using all irrigation solutions at a temperature of 20°C. Based on the obtained results, it might be interesting to re-evaluate the dressing removal capacity of XP-endo Finisher® files using the irrigant at higher temperatures since its manufacturer recommends a temperature of 36°C.28
In this study, the coronal region demonstrated a greater amount of residual Ca(OH)2 than the apical region in the CanalBrush™ group, confirming previously published results.16 However, contrary to Gokturk et al.,19 no statistically significant differences were observed between the coronal and apical regions of the other groups tested.
The effect of various techniques has been evaluated, including laser-activated irrigation using photon-initiated photoacoustic streaming (PIPS), ultrasonic, sonic, and conventional irrigation, with promising results for PIPS.29 This technique seems to be a sophisticated approach with better results that deserves further assessment.
The present study reinforces the previous evidence26 that, in the apical third, MDI is the least effective technique in Ca(OH)2 removal compared to the E1 - Irrisonic tip and CanalBrush™. This finding may result from the lowest capacity of MDI to improve irrigant entrance into RCS irregularities.12
In the literature review, as far as we know, no papers directly evaluate the application of the E1 - Irrisonic tip in the removal of Ca(OH)2 from round RCSs using the methodology applied in this study. One study24 evaluated the Ca(OH)2 removal from an oval RCS with micro-CT using this same PUI device; nevertheless, contrary to the present study, it evaluated RCSs with similar round diameters by radiographic and photographic methods and, so, the results are not comparable.
The differences found between this study’s results and those obtained in other studies6,16,19may be related to some variables inherent to the experimental designs: the concentration of the irrigation solution - NaOCl, its association with chelating agents, its temperature, and the method of accommodation and cutting of teeth, among others. Future studies could improve the standardization of the variables inherent to the experimental design and the evaluation/measurement of the parameters to be tested to sustain the clinical reference of an efficient method for intracanal medication removal.
Conclusions
Complete removal of Ca(OH)2 from the coronal and apical grooves was not achieved with any of the tested techniques. Within the conditions of this study, globally, 2.5% NaOCl activation with CanalBrush™ and E1 - Irrisonic tip was more effective in Ca(OH)2 removal than XP-endo Finisher® and MDI. CanalBrush™ and E1 - Irrisonic tip had no statistically significant differences between them. Considering the position of the groove, none of the techniques demonstrated differences in the efficacy of Ca(OH)2 removal between the coronal and apical region, except for Canal-Brush™, which performed significantly better in the apical third.

