











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
One of the main goals of the endodontic treatment is to shape and clean the entire root canal system; thus, knowledge of tooth morphology is a prerequisite for a successful outcome.1
The mandibular molar usually has two well-defined roots: a mesial root with two root canals and a distal root with one or two root canals.2,3 However, variations in this morphology may occur, such as a third distolingual root, isthmuses, and multiple root canals.2
A variation in the mesial root of the mandibular first molar has been reported in the literature as a third root canal, commonly called the middle mesial canal, with its incidence ranging from 0.26% to 46.15%, depending on the studied population.4 Some studies report a rarer configuration of mandibular first molars: four root canals in the mesial root, and one,5 two,6-9 three,10,11 and four12 root canals in the distal root. To overcome the challenges associated with anatomical complexity, the clinician must be able to distinguish and identify the topographic location of any additional canal orifices, which can be best achieved using a dental operating microscope.6,13
This report aims to present and describe the endodontic treatment of a mandibular first molar with six root canals - four in the mesial root and two in the distal root.
Case Report
A 20-year-old male patient presented at our private office with a chief complaint of pain and swelling in the left mandibular region. On clinical examination, the patient showed tenderness to percussion and palpation on tooth #36 and a negative response to the cold thermal pulp test. There was no mobility and no periodontal pocketing at probing. A preoperative radiograph (Figure 1) revealed that the root length of tooth #36 was shorter than its adjacent teeth, suggesting root resorption. It also showed a widening of the apical periodontal ligament and a radiolucency associated with the mesial and distal roots of the left mandibular first molar. Based on these findings, the diagnosis of symptomatic apical periodontitis was established.

The patient reported previous orthodontic treatment, and the medical history was noncontributory. He signed na informed consent form, and the non-surgical endodontic treatment was immediately initiated to relieve his pain. Local anesthesia was administered via inferior alveolar nerve block followed by buccal infiltration using 2% mepivacaine with 1:100,000 epinephrine (DFL, Rio de Janeiro, Brazil). The tooth was isolated with a rubber dam, and the access cavity was performed with a round diamond bur (1014, KG Sorensen, Cotia, Brazil) at high speed.
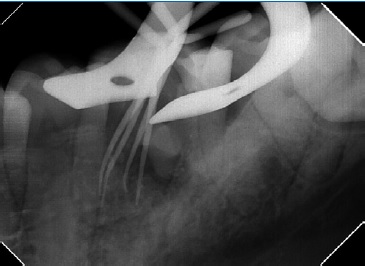
Initially, two root canals in the mesial root (Figure 2) and two in the distal root were located and negotiated with #10 and #15 C-Pilot hand files (VDW Dental, Munich, Germany) under an operating microscope (16x, Alliance Microscopia, São Carlos, Brazil). Clinically, the mesial root presented great flattening in the buccolingual direction; this was also observed in the periapical radiograph with the files in the two located canals (Figure 2), suggesting the presence of more canals. After further exploration, two more root canals were located in the mesial root (Figure 3). The working length was determined with na electronic apex locator (Root Zx II, Morita, Kyoto, Japan). The four mesial root canals were prepared with #25.08 and #40.06 Reciproc Blue files (VDW Dental, Munich, Germany) according to the manufacturer’s instructions. The distal canals were prepared with a #50.05 Reciproc Blue file (VDW Dental, Munich, Germany) and up to #60 hand files. After using each instrument, the root canals were irrigated with 3mL of 2.5% sodium hypochlorite (Danafarma, Curitiba, Brazil) with a 30-gauge irrigation needle (Navitip, Ultradent, South Jordan, USA).
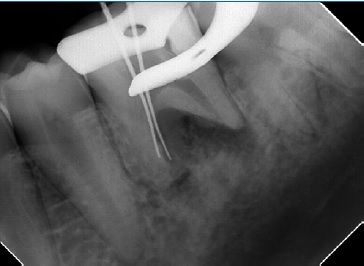
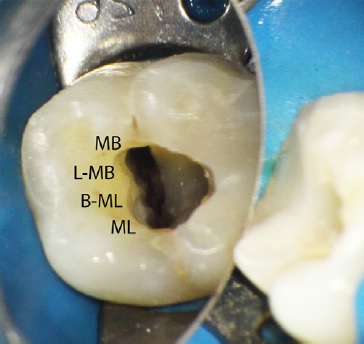
Figure 3 Mesial canals’ orifices after instrumentation: mesiobuccal (MB), linguo-mesiobuccal (L-MB), buccomesiolingual (B-ML), and mesiolingual (ML).
For the final rinse, it was not used alcohol. To enhance smear layer removal, 3 mL of 17.0% EDTA (Danafarma, Curitiba, Brazil) were used and agitated three times for 20 seconds each, using an Irrisonic ultrasonic tip (Helse Dental Technology, São Paulo, Brazil); the irrigating solution was renewed between the cycles. This same protocol was then used for the sodium hypochlorite solution. The ultrasonic tip was 18.0-mm long with a #20 tip diameter,.01 taper, and a smooth surface and was used at a power of 10% in the ultrasonic unit. The canals were dried with #30 matched paper points (VDW Dental, Munich, Germany) and dressed with calcium hydroxide paste (UltraCal XS, Ultradent, South Jordan, USA) using the syringe provided by the manufacturer and a 29-gauge needle (Navitip, Ultradent, South Jordan, USA). The access cavity was closed with a glass-ionomer cement (Ionofast, Biodinâmica, Ibiporã, Brazil).
On the second visit, one month later, the patient had no signs or symptoms. After local anesthesia and rubber dam placement, the temporary restoration was removed, and passive ultrasonic irrigation was again performed using the same protocol as in the first appointment to remove the intracanal dressing. The canals were dried with paper points. Root canal filling was performed using the single-cone technique with gutta-percha cones (Odous de Deus, Belo Horizonte, Brazil) Figures 4 and 5), previously disinfected by immersion in sodium hypochlorite for five minutes, and BioRootTM RCS sealer (Septodont, Saint-Maur-des-Fossés, France) (Figure 6). A temporary restoration was made with a glass-ionomer cement (Ionofast, Biodinâmica, Ibiporã, Brazil) to close the access cavity.


The patient was referred for tooth coronal rehabilitation, and after one week, the referring professional performed a definitive composite resin restoration. At the 12-month follow-up, a periapical radiograph showed bone repair in the periradicular region (Figure 7).

Discussion and conclusions
The mandibular first molar is among the first permanente teeth to erupt and often requires endodontic procedures.14 It usually has two roots and two to three root canals, and while the mesial root is flattened, the distal root is straight.2 In this case report, the mandibular first molar had four root canals in the mesial root and two in the distal root. The mesial canals were named mesiobuccal (MB), linguo-mesiobuccal (L-MB), bucco-mesiolingual (B-ML), and mesiolingual (ML) to consider the anatomical relation of roots and their root canals.8,15
The presence of a fourth canal in the mesial root of the mandibular molar represents a rarer morphology.5 In these cases of four root canals in the mesial root, the total number of root canals may vary up to eight depending on the distal root. In mandibular first molars, one report found one canal in the distal root,5 four found two canals in the distal root6-9(the same morphology as the present case), two found three canals in the distal root,10,11 and one found four canals in the distal root.12
The frequency of untreated canals is high in mandibular molars, second only to maxillary molars.16 Untreated canals are related to a higher probability of developing apical periodontitis16,17 and treatment failure.1 Before starting any treatment, it is important to consider morphological variations and carefully examine the tooth clinically and radiographically.6
Although cone-beam computer tomography provides undistorted 3D images of the root canal anatomy,10 periapical radiographs were the only aid used in most reported cases found with four canals in the mesial root.6,7,9,11,12,18 In the presente case, only periapical radiographs at different horizontal angles were taken, which provides information that gets even more accurate when combined with clinical findings.1
One of the etiological factors for root resorptions with reduced root length is the force applied during orthodontic treatment.19 In the present case, it could explain the shorter root length of the tooth compared to the adjacent ones, as the patient had undergone orthodontic treatment previously.
Magnification may enhance the detection of root canal orifices. Three reports used loupes,7,12,18 and three used operating microscopes.6,8,9The present case used an operating microscope, which helps locate and negotiate canals with great precision1,20 and has shown to be significantly better than the naked eye or surgical loupes.20
In mandibular molars, additional canals are usually hidden by a dentinal projection lighter than the color of the pulp chamber floor.12 Ultrasonic tips can be used to remove this dentin; these are safe tools that enhance visual access and allow better control to work in the pulp chamber.21 The presente case did not use them because there was no dentinal projection.
Another application of ultrasonic tips is to increase the action of irrigating solutions, as they act in the mechanical flushing and chemical ability of solutions to dissolve tissues.21
In the present case, the irrigating solutions were activated with an ultrasonic tip after the negotiation of the root canals to enhance the smear layer removal.
The present case used calcium-hydroxide paste as an intracana dressing. Its use between sessions enhances the disinfection of the root canal system,22 mainly in more complex canal systems,23 as it has wide-spectrum antibacterial activity24 and reduces bacterial lipopolysaccharide from infected root canals.25
After shaping and cleaning the root canal system, it is necessary to seal it properly. Bioceramic endodontic sealers have been widely used mainly due to their bioactive property of inducing proliferation and binding of cells close to cement and their potential to induce angiogenesis and osteogenesis, which are prerequisites for periapical tissue regeneration.26 In this case, a bioceramic endodontic sealer was used to fill the root canals, associating the single-cone technique with greater tapered gutta-percha cones to make the obturation a faster and simpler procedure, minimize the forces applied to the root canal walls by the spreaders, and not decrease the quality of the apical sealing.27,28
After one year, the patient presented no symptoms, and bone repair was observed radiographically. A longer follow-up time would be better to evaluate success, but the main objective of this case report was to present this rare anatomical variation.
The complexity of the root canal system is a challenge in endodontic treatment. Knowing the root morphology and its possible variations is essential to achieve a successful outcome in endodontic treatments. The presence of a fourth canal in the mesial root of the mandibular molar represents a complex anatomy that, when not considered, may lead to treatment failure. Aids such as an operating microscope, ultrasonically activated irrigation, and bioceramic endodontic sealers may contribute to endodontic management, as they enhance the visualization and negotiation of the root canals, improve the disinfection of the root canal system, and favor the boné repair, respectively.

