











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Dental pain is the most frequent cause of orofacial pain.1 It can mimic other types of facial pain because the dental pathology may refer pain to other teeth or distant locations in the maxillofacial area or the neck, making the diagnosis challenging.2
Dental pathologies can favor the spread of infection to the maxillary sinus due to the proximity of the root apexes to the maxillary sinus floor, leading to the development of sinus pathologies such as odontogenic maxillary sinusitis (OMS).3-6
OMS is secondary to an adjacent infectious maxillary dental pathology or complications from dental procedures.7 It has a prevalence of 25% to 40%,7-10with studies reporting a higher rate of 86%.3 The clinical presentations of rhinosinusitis can overshadow odontogenic sources, and dental symptoms can overshadow sinusitis.7
OMS is a condition still underestimated and underdiagnosed,7,11 and its diagnosis often requires evaluation by otolaryngologists and dentists.7 This report aims to present and describe two cases of OMS in which the dental source was correctly identified, and the pathology was managed by nonsurgical endodontic treatment and retreatment.
Case reports
Case 1
A 52-year-old female patient complained of a sharp and stabbing pain in her left cheek. It had started one year earlier, lasting a few minutes, and then worsened to persistente pain. A neurologist diagnosed her with trigeminal neuralgia and prescribed carbamazepine 400 mg BID, but she did not respond to this treatment. She underwent another medical consultation, which ruled out the trigeminal neuralgia diagnosis and suggested an evaluation with a dentist specialized in orofacial pain for a possible diagnosis of odontalgia.
During the consultation with the dentist, the patient presented with pain to palpation and percussion, and tooth #27 was negative for the cold pulp test, suggesting pulp alteration.
A computed tomography scan of the maxillary sinuses showed tooth #27 with delimited apical hypodensity and thickening of the left maxillary sinus membrane (Figure 1), compatible with an inflammatory lesion.

Figure 1 Initial computed tomography image of th left maxillary region showing apical periodontitis associated with tooth #27 and mucosal thickening in the maxillary sinus.
The patient was referred to an endodontist for nonsurgical root canal treatment (Figure 2). Tooth #27 was anesthetized with submucosal infiltration using 1.8 mL of 2.0% mepivacaine with 1:100,000 epinephrine (DFL, Rio de Janeiro, Brazil), and rubber dam isolation was established. The access cavity was made using 1014 and 3080 diamond burs (KG Sorensen, Cotia, Brazil), and the root canals were identified with the aid of an endodontic explorer. The working length was determined with an electronic apex locator (Root Zx II, Morita, USA). The mesiobuccal and distobuccal root canals were prepared with a #35.04 Mtwo file (VDW Dental, Munich, Germany), and the palatal root canal up to a #50.05 Reciproc file (VDW Dental, Munich, Germany) at 350 rpm of speed and 3 N of torque. All instrumentation was performed under copious syringe irrigation with 2 mL of 2.5% sodium hypochlorite per canal after using each instrument.

The final rinse consisted of irrigation with 2 mL of 17.0% EDTA per canal, which remained for three minutes, followed by a final sodium hypochlorite rinse with 5 mL of solution per canal. The root canals were dried using matched paper points #30 (VDW Dental, Munich, Germany).
Then, an intracanal dressing with calcium hydroxide paste (UltraCal XS, Ultradent, USA) was applied, and a glass-ionomer cement (Ionofast, Biodinâmica, Brazil) was used for a provisional restoration.
In the second appointment, the intracanal dressing was removed using a #20 manual file up to the working length, and final irrigation was performed with 17.0% EDTA and 2.5% sodium hypochlorite, following the same protocol as the first appointment.
The canals were dried with paper points. Then, root canal filling was performed with gutta-percha cones (Odous de Deus, Belo Horizonte, Brazil) calibrated according to the tip of the last instrument used, using the single-cone technique and the BioRootTM RCS sealer (Septodont, Saint-Maur-des-Fossés, France) (Figure 3). The access cavity was temporarily restored with glass-ionomer cement, and the patient was referred for coronal rehabilitation.

After the endodontic treatment, the patient became completely asymptomatic. A 5-month cone-beam computed tomography (CBCT) scan showed the absence of maxillary sinus abnormalities (Figure 4). Another CBCT scan two years later confirmed it (Figure 5).

Figure 4 5-month follow-up CBCT image of tooth #27 showing signs of repair of the apical periodontitis and maxillary sinus abnormalities.
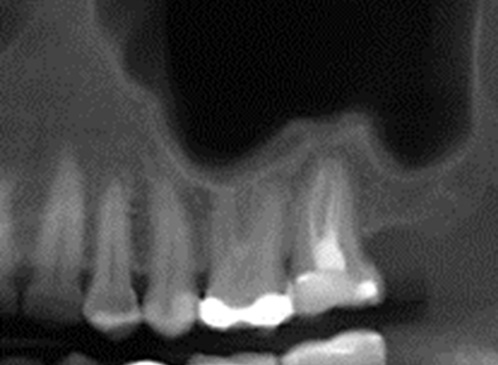
Figure 5 2-year follow-up CBCT image of tooth #27 showing absence of apical periodontitis related to tooth #27 and maxillary sinus abnormalities.
Case 2
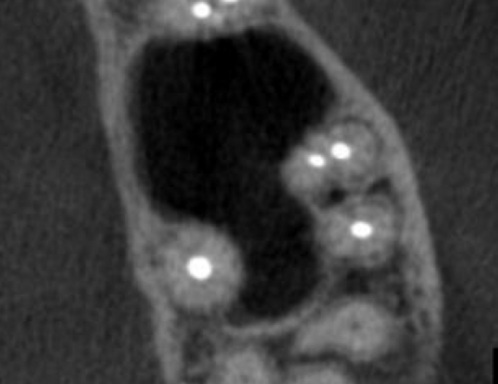
A 42-year-old female patient had a chief complaint of mild facial sensitivity in the left maxillary posterior region. On clinical examination, the patient presented with only slight discomfort in the molar teeth region during percussion, but teeth #23 and #27 were positive for the cold pulp test. Two months before, she had undergone endodontic treatment on tooth #26 due to irreversible pulpitis (Figure 6). The initial periapical radiography showed no changes in the premolars or molars (Figure 6), so a CBCT was requested. The CBCT revealed apical periodontitis in tooth #25, which had undergone previous endodontic treatment (Figure 7). It also showed thickening of the left maxillary sinus membrane and destruction of cortical bone (Figures 7 and 8). Thus, it was decided to perform nonsurgical endodontic retreatment.


Figure 7 Initial CBCT image (sagittal view) showing cortical bone destruction and mucosal thickening associated with tooth #25.

The access cavity was obtained with a round high-speed diamond bur (1014, KG Sorensen, Cotia, Brazil) under suitable anesthesia and rubber dam isolation. After locating the root canals, the filling material was removed using a #25 Reciproc Classic file (VDW Dental, Munich, Germany) without solvent. The working length was determined with an electronic apex locator (Root Zx II, Morita, USA). The root canals were instrumented with a #35.04 Mtwo file (VDW Dental, Munich, Germany), and the palatal root canal up to a #50.05 Reciproc Blue file (VDW Dental, Munich, Germany).
All instrumentation was performed under copious syringe irrigation with 2.5% sodium hypochlorite. The final rinse consisted of irrigation with 2 mL of 17.0% EDTA per canal, which remained for three minutes, followed by a final sodium hypochlorite rinse with 5 mL of solution per canal. The root canals were dried using matched paper points #30 (VDW Dental, Munich, Germany). Then, an intracanal dressing with calcium hydroxide paste (UltraCal XS, Ultradent, USA) was applied, and a glass-ionomer cement (Ionofast, Biodinâmica, Brazil) was used for a provisional restoration.
In the second appointment, the intracanal dressing was removed using a #20 manual file up to the working length, and final irrigation was performed with 17.0% EDTA and 2.5% sodium hypochlorite, following the same protocol as the first appointment.
The canals were dried with paper points. Then, root canal filling was performed with gutta-percha cones (Odous de Deus, Belo Horizonte, Brazil) calibrated according to the tip of the last instrument used, using the single-cone technique and the BioRootTM RCS sealer (Septodont, Saint-Maur-des-Fossés, France) (Figure 9). The access cavity was temporarily restored, and the patient was referred for coronal rehabilitation.

The symptoms showed improvement after the first appointment, in which the filling material was removed and the root canals were disinfected and filled with the intracanal dressing. They completely disappeared after 15 days of treatment. After 16 months, a CBCT scan showed signs of normality (Figures 10 and 11).

Figure 10 16-month follow-up CBCT image (sagital view) of tooth #25 showing cortical bone repair and absence of maxillary sinus abnormalities.
Discussion and conclusions
A pulpal infectious process in maxillary posterior teeth can affect the integrity of the maxillary sinus floor and lead to inflammatory changes in the sinus mucosa, such as its thickening.6,12The maxillary sinus mucosa can be considered normal when there is no thickening or a uniform thickening of up to 2 mm,11-13 or up to 3 mm.14
Teeth-related mucosal thickening in the sinus was observed in both reported cases. This sign is the most common abnormality of the maxillary sinus, with a prevalence ranging from 36% to 58.5%.3,4,9,11,14Special attention must be given to the involvement of one or both sinuses, as unilateral involvement is considered a sign to investigate dental etiology.15 Also, mucosal thickening is ten times more common in individuals with apical periodontitis,15 reaching a prevalence of 70% in those with mild and moderate apical periodontitis and 100% in those with severe apical periodontitis.3
In the first case reported, the sinus pathology was related to the second molar, which had its roots located below the maxillary sinus floor. This finding agrees with a previous study that reported that the mesiobuccal root is the closest to the sinus floor.16 In the second case reported, the affected tooth was the second premolar, which, compared to the first premolar, is closer to the maxillary sinus floor,16,17 and is usually located below it.15,16
However, studies evaluating the relationship between the sinus mucosal thickening and the anatomical relationship of the root apexes reported that the proximity of the root apex
to the floor of the maxillary sinus alone did not influence the development of mucosal thickening,3,11only when associated with other factors, such as the presence of apical periodontitis.3,11 Likewise, one study indicated that the presence of endodontic treatment alone did not increase the degree of mucosal thickening.11 Adequate length, homogeneity of the filling, and coronal sealing have been related to the absence of sinus abnormalities (63.98%, 74.19%, and 89.78% of cases, respectively) and higher rates of an absence of periapical lesions (68.71%, 78.7 8%, and 89.93% of cases, respectively).4
The clinical symptoms of OMS alone are not sufficient for its diagnosis since this condition may be asymptomatic.7 In both reported cases, the patients only reported pain or discomfort in the maxillary area. However, common symptoms ofOMS are foul smell, purulence, and dental pain.7
Imaging exams are important tools for diagnosing OMS. Panoramic radiographs are limited due to the overlap of anatomical structures and the impossibility of cross-sectional analysis. In turn, CBCT provides three-dimensional images, showing the size and location of periapical lesions and the proximity of root apices to other structures.3,5,12,13A study comparing these two types of imaging exams reported that panoramic radiography provided smaller distances and a greater relationship of apices within the maxillary sinus.13 In our second case, apical periodontitis or sinus abnormalities were not observed in the initial periapical radiography, but the CBCT showed changes in the maxillary sinus and its association with the affected teeth. Periapical radiographs can provide high-quality images but have the same limitation as panoramic radiographs: the superimposition of anatomical structures.15
The treatment for OMS typically includes nonsurgical root canal treatment, periradicular surgery, or even tooth extraction.6 In both reported cases, nonsurgical root canal treatment or retreatment was the choice, and no antibiotics were required. For the successful management of OMS, the primary goal is to control the root canal infection rather than using systemic antibiotics, as these will not treat the cause of the pathology.6
The cases reported demonstrate the importance of a correct diagnosis to provide the best management for the patient and avoid unnecessary interventions. It often requires a multidisciplinar approach involving otorhinolaryngologists and diverse specialties within dentistry.7,10,11 The cold pulp test and the CBCT scan are important to help in the differential diagnosis.6,7,15 When there is an endodontic origin, the tooth must have a necrotic pulp or a failing root canal treatment.6
Dental pathologies of endodontic origin may spread infections to the maxillary sinus. Clinicians must be knowledgeable about OMS and be able to determine whether the symptoms reported by the patient have a truly odontogenic origin. It is important to incorporate CBCT images into the diagnostic process to determine if there is a relationship between the dental source and maxillary sinus abnormalities.

