











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
In contemporary dentistry, the primary objective of restorative treatments is to maintain the chewing function, preserve tooth structure through a minimally invasive approach, and fulfill the aesthetic expectations of patients.1 The introduction of resin-based composites has marked significant advancements in restorative dentistry. These materials are increasingly favored by both clinicians and patients due to their numerous advantages, including aesthetic appeal, biocompatibility, mercury-free composition, low thermal conductivity, facilitation of conservative cavity preparation, and capacity to support the remaining dental tissues following caries removal.2
While the Academy of Operative Dentistry - European Section (AODES) accepts resin composites as the preferred restorative material in direct minimal interventions applied to posterior teeth, it reports that the structural properties of these materials are still insufficient.3 Restoration size is a potential confounder to the lifetime of resin composite restorations. It is more common for restorations to fail due to fracture, especially in teeth with excessive crown destruction.4 Therefore, with the developments in adhesive dentistry, fiber-reinforced resin composites have become popular.5 Fibers are used to strengthen remaining tooth tissue and existing large restorations against occlusal forces.6
Fiber-reinforced resin composites, which can be used as a dentin-replacing material, have been produced for use in áreas that experience high chewing forces, especially posterior teeth.7 Two important parameters for resin composites reinforced using random short fibers are fiber aspect ratio and fiber volume fraction.8 The fiber aspect ratio is the ratio of the fiber’s length to its diameter and affects the compressive and tensile strengths and the bending modulus of fiber-reinforced resin composites.9 Fiber-reinforced resin composites with a high length/diameter ratio have shown better flexural strength than those with a low length/diameter ratio. In addition, resin composites reinforced with short and very short fibers have better flexural strength than conventional resin composites.10
The role of fibers is to improve the physical properties of resin composites by acting as a fracture stopper-stress breaker.11
However, fibers are used as an infrastructure material and must be covered with a composite layer because they impair polishing processes.12
Fiber-reinforced resin composites, similar to conventional resin composites, consist of an organic matrix and an inorganic filler phase. However, the filler phase is composed of fibers in fiber-reinforced composites, as opposed to particles in conventional composites.13 The incorporation of fibers into the matrix is a highly effective method for enhancing the reinforcement of resin composites. By transferring the stresses from the matrix to the fibers, the occurrence of fractures in both the tooth and the restoration can be effectively mitigated.14 The mechanical properties of fiber-reinforced resin composites are influenced by several factors, including the arrangement, type, density, and saturation of the fibers, as well as the composition of the matrix and the bonding between the fibers and the matrix.15 The fibers’ favorable mechanical properties allow for the preparation of finer restorations. Moreover, due to their modulus of elasticity being comparable to that of dentin, they are less likely to induce damage to the tooth structure.16
A review of the literature reveals no studies that simultaneously compare the physical and mechanical properties of everX Flow™ (eXF), everX Posterior™ (eXP), Filtek™ Bulk Fill Flowable Restorative (FBFf), and Filtek™ One Bulk Fill Restorative (FBF). Research examining the surface roughness, flexural strength, and microtensile bond strength of the newly introduced fiber-reinforced bulk fill composite eXF is scarce. This in vitro study, conducted on primary teeth, seeks to fill this gap in the literature, particularly in the context of pediatric dentistry, where ease of application is extremely important.
The study aims to provide valuable insights into the physical and mechanical properties of eXF, thereby offering useful information for dental professionals.
The null hypotheses of the study were: H1) There is no difference in surface roughness values between fiber-reinforced resin composites and particulate-filler resin composites; H2) There is no difference in flexural strength values between fiber-reinforced resin composites and particulate-filler resin composites; H3) There is no difference in terms of bond strength values in primary teeth between fiber- reinforced resin composites and particulate-filler resin composites.
Material and methods
The experimental phase of the study was carried out in three parts: surface roughness, bending, and microtensile bond strength tests. In each test, the samples were divided into four groups corresponding to the material studied: eXF, eXP, FBFf, and FBF. The properties of the resin composites used in the study are listed in Table 1.
Table 1 Properties of the materials used in the study
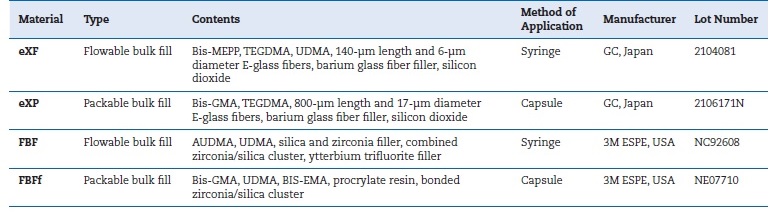
Bis-MEPP - bisphenol A methacryloxy ethoxy phenyl propane; TEGDMA - triethylene glycol dimethacrylate; UDMA - urethane dimethacrylate;
Bis-GMA - bisphenol A glycidyl methacrylate; AUDMA - high molecular weight aromatic dimethacrylate; Bis-EMA - bisphenol A ethoxylate dimethacrylate
For surface roughness tests,17 disc-shaped plexiglass molds with a 10-mm diameter and a 2-mm height were used to ensure standardization of the specimens. After positioning plexiglass molds on a glass surface using transparent tape, the restorative materials were applied to the mold in a single layer.
A Mylar matrix strip and glass were then placed over the mold. Following glass removal, the materials were polymerized according to the manufacturer’s instructions. A total of 40 specimens were prepared, with ten specimens in each group.
Finishing and polishing processes were carried out on both surfaces of the specimens with finishing and polishing discs containing aluminum oxide particles (Super-Snap Rainbow Technique Kit, Shofu, Japan). The specimens were kept in distilled water at 37 °C for 24 hours, and then a profilometer device (Mitutoyo Surftest/ SJ-301, Tokyo, Japan) was used to test their surface roughness. The average surface roughness (Ra) value was calculated by measuring three distinct random points on each specimen and determining the arithmetic mean of the obtained data.
For the flexural strength tests,17 metal molds with 25×2×2-mm cavities were used to obtain specimens compliant with the International Organization for Standardization (ISO) 4049:2019 standards. The composites were placed in stainless steel molds on a glass surface, which was positioned on a flat, horizontally aligned surface to ensure the absence of any air gaps. A transparent tape was applied to
secure the molds, and light was irradiated for 20 seconds from each of the three regions of the specimen. A total of 40 specimens were prepared, with ten specimens allocated to each group. Excess material formed at the specimens’ edges was smoothed using water-based sandpaper. The specimens were stored in distilled water at 37 °C in tightly sealed, light-protected containers for 24 hours. Afterwards, they underwent a three-point flexural test at a 1-mm/min speed using the universal testing device LF Plus (LLYOD Instruments, Amatek Inc., England). The device measured the maximum force required to fracture the specimens in Newtons (N) upon specimen failure. The flexural strengths of the specimens were calculated in MPa using the 𝜎 =3𝑃𝑙/2𝑏𝑑2 formula. (σ: flexural strength; 𝑙: distance between support points; b: specimen width; d: specimen thickness; P: maximum load at break).
For the microtensile bond strength tests,17 64 human primary molars, extracted for orthodontic purposes, physiological root resorption, or periodontal reasons, were collected.
The teeth were carefully examined for caries, fractures, cracks, or previous restorations in the crown area. Any problematic teeth were excluded from the study. The remaining teeth were randomly assigned to four groups, with 16 teeth allocated to each test group. The occlusal surfaces of the teeth were abraded using a low-speed, water-cooled Diamond bur to expose the superficial dentin tissue. The specimens were then embedded in autopolymerizing cold acrylic (Integra Dental, Ankara, Turkey) within L-shaped silicone molds. Silicon carbide papers with 600, 800, and 1200 grits were sequentially applied for 30 seconds each, under running water, to standardize the smear layer on the exposed dentin surfaces. A universal adhesive system (Single Bond Universal, 3M ESPE, Germany) in self-etch mode and each group’s restorative materials were applied to the prepared dentin surfaces, according to the manufacturer’s instructions.
The teeth embedded in the acrylic blocks were placed in a low-speed precision cutting device (Isomet 1000, Buehler, USA) to obtain approximately 1x1-mm2 wide and 7-8-mm long rod-shaped specimens.
Microtensile bond strength testing was performed using the universal testing device LF Plus (LLOYD Instruments, Ametek Inc., England). The specimens were subjected to stress by applying a 100-N tensile force at a speed of 0.5 mm/min.
The units of microtensile bond strength values of the four composite groups were converted from N to MPa, and statistical evaluations were made. The fractured specimens were carefully removed from the test apparatus in the microtensile test device, and their surfaces were subsequently examined using a stereomicroscope (SMZ 800, Nikon, Tokyo, Japan) at 40x magnification. The fracture modes were then categorized into three types: adhesive, cohesive, and mixed. One specimen from each group, representative of the diferente fracture types, was selected for analysis using a scanning electron microscope (SEM; TESCAN MIRA3 XMU, Brno, Czechia) to assess the bonding interfaces. The specimens were mounted on holders using double-sided carbon tape and then gold-coated using a coating device (Quorum Q150R ES, Quorum Technologies, England). Then, each was examined under various magnifications using the SEM to evaluate the binding surfaces.
The statistical analysis of the data collected from the study was performed using the SPSS 22.0 software. As the assumptions for parametric testing were met, the one-way analysis of variance (ANOVA) was employed to compare the measurements obtained from more than two independent groups. In the presence of significant differences in the ANOVA results, the Tukey post-hoc test was applied to determine which group(s) contributed to the differences. The significance level was set at 0.05.
Results
The mean values of the restorative materials tested for surface roughness, flexural strength, and microtensile bond strength are shown in Table 2 with their standard deviations. The highest values in the surface roughness tests were 0.78±0.22 μm for eXP, 0.61±0.08 μm for eXF, 0.47±0.18 μm for FBF, and 0.42±0.11 μm for FBFf. While there were statistically
Table 2 Average and standard deviation (± SD) values of surface roughness (SR), flexural strength (FS), and microtensile bond strength (μTBS).
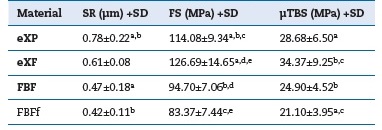
Shear bond strength values are shown as mean ± SD. The same lowercase letter represents a statistically significant difference within each column significant differences between eXP, FBF, and FBFf (p<0.05), there was no statistically significant difference between the other resin composites.
In the flexural strength test results, the highest values were 126.69±14.65 MPa for eXF, 114.08±9.34 MPa for eXP, 94.70±7.06 MPa for FBF, and 83.37±7.44 MPa for FBFf. eXF and eXP showed a statistically significant difference compared to the other resin composites (p<0.05).
In the analysis of μTBS tests, the highest binding values were 34.37±9.25 MPa for eXF, 28.68±6.50 MPa for eXP, 24.90±4.52 MPa for FBF, and 21.10±3.95 MPa for FBFf. eXP showed a statistically significant difference compared to FBFf (p<0.05). eXF showed a statistically significant difference compared to FBF and FBFf (p<0.05).
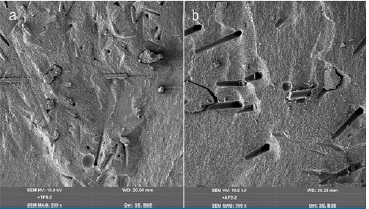
In the analysis of failure types, fractured surfaces were analyzed with a SEM and stereomicroscope (Figure 1). The most frequent failure type was adhesive (68.75%) (Figure 2), followed by mixed (26.57%) (Figure 3), and then cohesive (4.68%) (Figure 4).
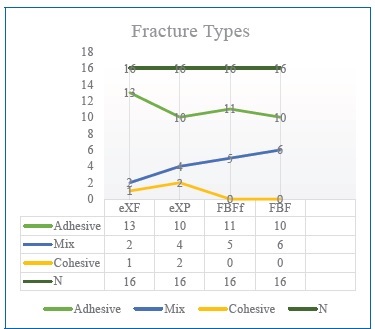
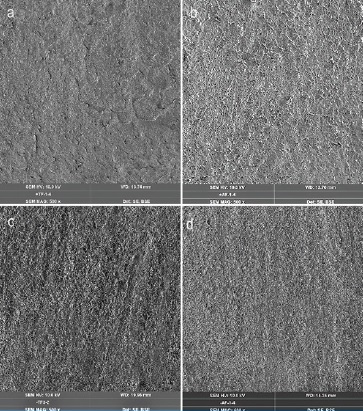
Figure 2 SEM images of the adhesive fracture type. (a) everX Posterior, (b) everX Flow, (c) Filtek One Bulk Fill Restorative, (d) Filtek Bulk Fill Flowable Restorative
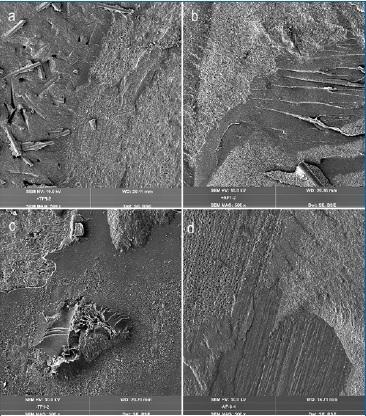
Figure 3 SEM images of the mixed fracture type. (a) everX Posterior, (b) everX Flow, (c) Filtek One Bulk Fill Restorative, (d) Filtek Bulk Fill Flowable Restorative
Discussion
For many years, research has focused on identifying the most suitable materials and methods to restore tissue lost due to factors such as caries, fractures, or wear in the hard dental tissues.18 In recent years, one of the alternative methods used to support the remaining dental tissues in tooth restoration is the fiber reinforcement of resin composite restorations.18,19 Due to its high flexural strength, fiber-reinforced resin has suitable mechanical properties as a restoration infrastructure material. The fiber-reinforced resin infrastructure not only imparts hardness and durability to the material but also increases the resistance of teeth to mechanical stresses through its elastic, stretchable structure. Thus, the substructure’s durability and rigidity combine with the superstructure’s aesthetics.20 Research has demonstrated that the disadvantages of resin composites can be mitigated to acceptable levels through the use of fibers in the restoration of teeth with significant material loss. This approach enhances the fracture strength of weakened cusps, acts as a stress breaker in composite restorations, and reduces polymerization shrinkage.21-23
The null hypothesis H1, which stated “there is no difference in surface roughness values between fiber-reinforced resin and particulate-filler resin composites,” was partially rejected. While eXP demonstrated statistically significantly higher surface roughness values than particulate-filler resin composites, eXF did not show a statistically significant difference in surface roughness compared to the particulate-filler resin composites. Although the packable bulk-fill composite FBF (74.2% by weight) and the fiber-reinforced bulk-fill composite eXP (76.5% by weight) exhibit nearly identical filler ratios, the disparity in surface roughness is likely due to differences in the size and type of the inorganic fillers, as well as the processes involved in the remediation of the resin matrix.
In their study, Ruivo et al.24 stated that resin composites containing irregularly shaped inorganic fillers will be exposed to more frictional forces by abrasive materials, and surface roughness will increase compared to resin composites containing spherical-shaped inorganic fillers. In addition, they reported that resin composites containing zirconia- based inorganic fillers would show lower surface roughness values due to the high wear resistance and hardness of zirconium. In this study, FBFf and FBF containing zirconia- based inorganic filler also showed lower average surfasse roughness values than eXF and eXP reinforced with shortclipped fiber. In their research, Jafarnia et al.25 compared the surface roughness of fiber-reinforced resin (eXP) and particulate-filler bulk-fill resin composites (FBF and Beautifil-Bulk), reporting that eXP exhibited the highest surface roughness values after polishing. The results of their study, which assessed the surface roughness of eXP and FBF, are consistente with the present study’s findings.
In addition to the ratio and size of the inorganic particles, the extent of bonding between the inorganic particles and the organic matrix, and the structure of the organic matrix als significantly influence the surface roughness of the composites.26 The presence of TEGDMA in the organic matrix of eXP and the incorporation of UDMA and Bis-EMA monomers in the organic matrix of FBF may explain the lower surface roughness observed in FBF compared to eXP.
A literature review revealed only one study evaluating the surface roughness of the recently introduced eXF resin composite. Mangoush et al.27 reported that Cerasmart 270 exhibited the lowest surface roughness values among the tested composites in their study, which aimed to compare the specific surface properties and microstructure of an experimental short fiber-reinforced CAD/CAM composite block with comercial composites produced by different methods. However, due to significant differences in both the materials and methodologies used in their study and the present research, it was not possible to directly compare their findings with ours. This study is the first to compare the surface roughness of eXP and eXF. In the current study, the average surface roughness of eXF was lower than eXP’s. This difference may be attributed to the smaller size of the filler particles and glass fibers in eXF, as well as the incorporation of UDMA monomers, which enhance the structural integrity of eXF compared to the organic matrix structure of eXP.
Studies on the mechanical properties of fibers have indicated that glass fiber exhibits superior durability compared to polyethylene fiber. The primary reason for this enhanced durability is attributed to the saturation of glass fibers during the production process. It has also been reported that pre-saturation increases the flexural strength of the fiber by 2-3 times.28,29
The widespread use of glass fibers in dentistry and its clinical success depends not only on its good mechanical strength, but also on its biocompatibility, superior aesthetic properties, and easy manipulation. Good adhesion of glass fibers with the resin matrix contributes positively to the mechanical properties of the future restoration.30
Many studies have been conducted to test the resistance of fibers used in dentistry, which stand out with their superior mechanical properties, against fluctuation. The results of this study are consistent with the literature reporting that fiber-reinforced resin has high flexural strength.14,31-35 The null hypothesis H2, which stated “there is no difference in flexural strength values between fiber-reinforced resin and particulate-filler resin composites,” was fully rejected because eXP and eXF demonstrated statistically significantly higher flexural strength values than the particulate-filler resin composite.
In their study, Lassila et al.9 reported that no direct correlation was observed between the volumetric content of inorganic particles and fracture resistance parameters. Specifically, an experimental fiber-reinforced resin with a lower volume of inorganic filler demonstrated superior flexural strength and fracture toughness values than other composites with higher volumes of inorganic filler. The findings of
Lassila et al. are consistent with the results of this study. eXF, which contains a lower percentage of glass filler (45-52%), exhibited higher flexural strength than eXP (60-70%), which has a higher filler content. In addition to the filler phase, it is well-established that the fibers incorporated into resin composites contribute to increased flexural strength. The fiber content in eXF (25%) is significantly higher than in eXP (5-15%). Therefore, it is hypothesized that the higher fiber contente by volume in eXF may contribute to its superior flexural strength values relative to eXP. eXP contains fibers longer than the critical fiber length, effectively transferring stress from the matrix. It also has a semi-IPN matrix type where the presence of thermoplastic PMMA chains reduces the stiffness of the Bis-GMA monomer.36 Studies have shown that these specific features can improve the flexural properties of the composite material and increase its resistance to fracture.12,36,37 In contrast, although the aspect ratio of the glass fibers in eXF is lower than that in eXP, the enhanced wetting of the fibers in eXF and their improved adhesion to the organic matrix may contribute to the higher flexural strength values observed in eXF compared to eXP.*
Lassila et al.,38 in their in vitro study evaluating the physical properties of various commercial fiber-reinforced resins (eXF, eXP, Alert, NovaPro-Flow, and NovaPro-Fill), observed that eXF and NovaPro-Fill exhibited the highest flexural strength values. Notably, eXF demonstrated higher flexural strength values than eXP, a finding consistent with the present study’s results.
A literature review indicates that most studies on the bond strength of restorative materials in dentistry have focused on permanent teeth, with relatively few studies on primary teeth.39-47 Therefore, the efficacy of adhesive systems in primary teeth should be assessed independently. While limited studies exist in the literature examining the microtensile bond strength of eXP,48,49 there is only one study, to the authors’ knowledge, that investigates the microtensile bond strength of eXF.50 Upon reviewing these studies, it was observed that they were conducted using permanent teeth. This study is the first to compare eXF and eXP in primary teeth, offering a novel perspective on their performance in this context.
In their study, Harp et al.50 compared fiber-reinforced resin and particulate-filler flowable bulk-fill resin composites in terms of microtensile bond strength in Class I cavities with a high configuration factor. They found that eXF exhibited similar bonding effectiveness to dentin as other flowable composites, with no statistically significant difference observed in the microtensile bond strength values between eXF and the other composites. In this study, the eXF group exhibited the highest microtensile bond strength values among the four bulk-fill composite groups. When eXF was compared to the other composites, the differences were statistically significant, except for eXP. SEM analysis of the fracture surfaces in the eXF group revealed several notable observations: few open dentin tubules, inorganic structures firmly adhered to the dense organic matrix on the dentin tubules, an irregular polymer structure with crater-shaped indentations on the composite surfaces, and the presence of minimal macro-resin tags detached from the dentin surfaces. These findings collectively support the conclusion that eXF demonstrates a strong bond between the composite and dentin.
A literature review indicates that some studies report no significant difference in bond strength between fiber-reinforced resins and other resin composites.51-55 In contrast, other research suggests that fiber reinforcement may impact the bond strength values of resin composites.56-58 The null hypothesis H3, which stated “There is no difference in bond strength values between fiber-reinforced resin and particulate-filler resin composites in primary teeth,” was partially rejected. Although a statistically significant difference in bonding values was observed between eXF and FBFf, the absence of a statistically significant difference between eXP and FBF does not conclusively suggest that fiber reinforcement has a definitive effect on bond strength. It is hypothesized that the higher bonding values observed in fiber-containing groups may be attributed to the presence of short fibers with a protruding structure in these composites, which likely enhance bonding by facilitating micromechanical interlocking with the dentin tissue.
The fiber-reinforced resin groups are microhybrid composites, while FBF is a nanofilled resin, and FBFf is a nanohybrid resin composite. Nanocomposites offer several advantages, including enhanced durability, reduced polymerization shrinkage, improved polishability, and superior aesthetic properties.59 Despite these positive properties of nanocomposites, some negative properties have also been reported in the literature.
Namely, adding nanoparticles to resin composites, which show an extensive surface area in these materials, causes an agglomeration problem during polymerization. This situation can cause brittleness and undesired problems, such as cracks and fractures after polymerization.60 Moreover, because aggregation causes a decrease in the active surface area, there is a decrease in the catalytic effect. It has also been reported that nanocomposites’ repair bond strength lags behind the composite material’s cohesive strength.59 Considering this information, the lower bond strength values observed for FBF and FBFf compared to eXF and eXP may not be solely attributed to the absence of fiber. It is also suggested that the agglomeration of nanosized inorganic fillers in these materials may negatively affect bonding by reducing the active surface área energy.
Conclusions
Within the limitations of the in vitro tests performed in the study, it was concluded that fiber-reinforced resin composites increased the flexural strength and bond strength to dentin, but the surface roughness was higher. Since this study is the first in some aspects, more in vitro and in vivo studies are needed.

