










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
versão impressa ISSN 1646-5830
Acta Obstet Ginecol Port vol.11 no.2 Coimbra jun. 2017
CASE REPORT/CASO CLÍNICO
Myeloid sarcoma involving the cervix - about a clinical case
Sarcoma mielóide do colo do útero - a propósito de um caso clínico
Cláudia Meneses Alves*, Nelson Domingues**, Mónica Cruz-Pires**, Diana Felizardo*, Maria Rosales**
Instituto Português de Oncologia do Porto FG, EPE
*Interna de Formação Específica
**Assistente Hospitalar
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Myeloid sarcoma is defined as a tumour of myeloblasts and immature myeloid cells that occurs in an extramedullary tissue. It is a rare form of presentation, which may arise in different locations and the cervix is one of the most unusual places. The available therapeutic options are chemotherapy and radiotherapy. The main prognostic factors are the response to initial treatment and cytogenetic abnormalities. This article describes the case of a woman presenting pelvic pain and vaginal discharge as chief complaints. After detection of a mass in the uterine cervix, the diagnosis was established by histology and immunophenotyping.
Keywords: Acute myeloid leukaemia; Myeloid sarcoma; Cervix
Introduction
Acute myeloid leukaemia (AML) may have different forms of presentation in extramedullary (EM) locations with or without bone marrow (BM) disease1. Myeloid sarcoma (MS) is a well established form of presentation of AML. It´s defined as a tumour of myeloblasts or immature myeloid cells that occurs in an EM place2-13. It can occur as infiltrates of myeloid blasts in any anatomic site of the body, however they are only classified as MS if they alter the architecture of the tissues involved2,4. The most common sites of involvement are subperiosteal bone structures, as well as skin, lymph nodes, soft tissue, central nervous system, gastrointestinal tract and orbit2,3,7,10,13-17. In the female population, the genital tract and the breasts are sites that may also be affected, although less frequently8.14. MS can be diagnosed as an isolated form, when there is no previous history of leukaemia, myelodysplastic or myeloproliferative syndrome and a normal BM aspirate. It can occur before the onset of AML, concurrently with the diagnosis, or as a post-treatment stage, as a form of recurrent disease with or without spinal cord involvement1-7,9,11-13.
Epidemiologically, MS has an incidence of 2/1.000.000 in the adult population7,17 and is described in approximately 2.5 to 9.1% of patients with AML1,3,11,14,15.
The case presented here intends to illustrate a rare form of MS presentation and its most relevant defining characteristics, in terms of pathology, epidemiology, management and prognosis.
Clinical case
Female patient, 53-year-old, caucasian, with the following past medical history: erythema nodosum, bilateral episcleritis, disc herniation, depressive syndrome, pericardial effusion history. Unremarkable social and family history. She had her menarche at the age of 12, gravida 3, para 2, abortion 1 and menopause at 49 years old. At the time of diagnosis, she was taking tibolone as hormonal replacement treatment and was applying topical vaginal oestrogen cream.
Present illness dates back from April 2015, when she had an episode of vaginal bleeding. The only anomaly reported then was an intramural pericentimetric myoma that the pelvic ultrasound exposed. In June 2015 the patient complained of yellow leucorrhoea associated with increasing pelvic pain. Gardnerella vaginallis was identified in the exsudate (treated with clindamycin). Due to persistent complaints, a colpocytology was undertaken in August and the result was negative for intraepithelial lesion (NILM) with inflammation. The finding of a hard cervix with easy bleeding led to colposcopy with biopsy of the cervix and curettage of the cervical canal. The anatomopathological examination showed MS, triggering the referral to our Institution. The physical examination was unremarkable, except for the gynaecological examination, that revealed a yellow leucorrhoea and an enlarged and hardened cervix with 5-6cm of diameter, although the superficial epithelium was smooth, without erosions or proliferative lesions. The digital rectal examination detected only an enlarged cervix with apparently spared parametria.
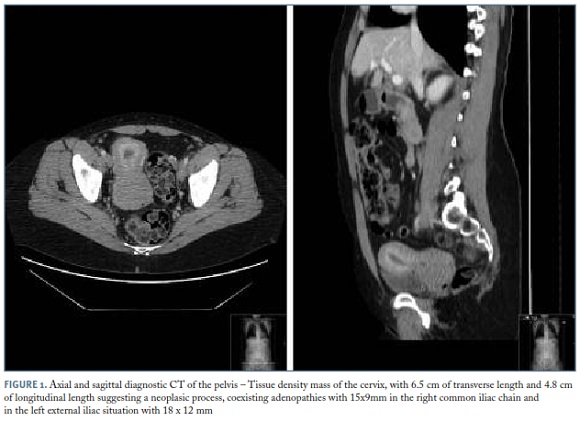
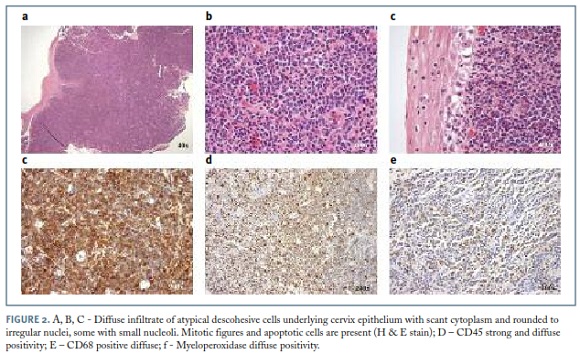
The blood count, serum biochemistry, chest x-ray and electrocardiogram were normal. The BM aspirate for myelogram and the immunophenotype study by cytometry revealed no abnormalities. A computed tomography (CT) scan of the thorax, abdominal and pelvis found “a tissue density mass on the cervix, with 6.5 cm of transverse length and 4.8 cm of longitudinal length, suggesting a neoplasic process, coexisting adenopathies with 15x9mm in the right common iliac chain and in the left external iliac situation with 18 x 12 mm” (Figure 1). A review of the biopsy slides and a new biopsy of the cervix were performed and both confirmed the diagnosis. Immunohistochemistry confirmed the result (immunophenotype: CD45 +, CD68 +, MPO +, CD34-, CD20-, CD3-) (Figure 2).
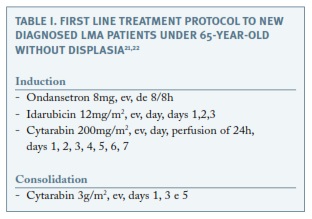
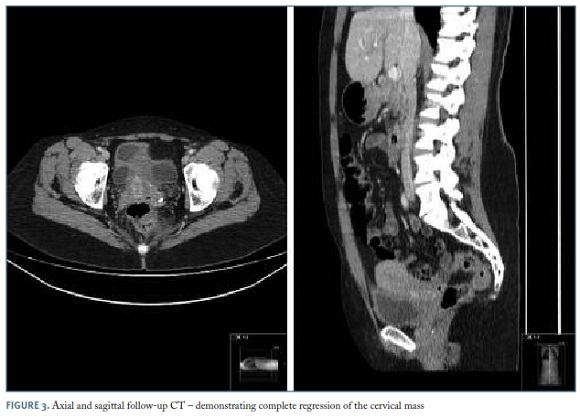
The treatment was set in a joint meeting between onco-hematology and radio-oncology units. Initially, the patient started with a chemotherapy “7+3” protocol (idarubicin and cytarabine), followed by consolidation with cytarabine in high dose according to the Institution protocol for AML (Table I) and concluded with pelvic external radiotherapy for a total of 30Gy. The hospitalization period for receiving induction chemotherapy and to allow hematologic recovery was 31 days. The most relevant complications of the induction chemotherapy were an episode of neutropenic enterocolitis with need for parenteral nutrition and a severe transfusion reaction, both resolved without sequelae. The assessment of the response by clinical examination and CT scan after treatment, showed regression of the cervical and ganglionary changes observed initially, remaining only a discrete thickening of the cervix (Figure 3). Based on this assessment, we consider that the patient had a complete response to the treatment. Currently, she is asymptomatic and maintains follow-up visits in onco-hematology and gynecology units, with a 3 months’ interval between them with focus in blood count and gynaecological examination.
Discussion
The granulocytic sarcoma (GS), also called chloroma, myeloblastoma, extramedullary myeloid tumour and monocytic sarcoma, was first described in 1911 by Burns. In 1953, King renamed it chloroma because of its yellowish green appearance, secondary to high levels of myeloperoxidase. Dock and Warthin recognized its association with the LMA in 1904. In 1966, Rappaport established the nomenclature of GS and described it as a destructive solid tumour composed by immature cells of the granulocytic lineage. Later, in 1988, this nomenclature had been amended by Davey to extramedullary myeloid tumour cells. In 2001, the World Health Organization (WHO) set a new nomenclature for this entity, renaming the myeloid sarcoma and classifying it into two categories: the granulocytic sarcoma and monoblastic sarcoma6,14.
According to the literature, the female genital tract, is an unusual place for MS7-9,14. In this anatomical area, the ovary is the most affected organ (about 36.4%)7 followed by the cervix and body of the uterus (about 10%)14.
The clinical presentation of this condition can be diverse and related to the affected site and the size of the mass. Therefore, the symptoms are caused by compression with pain, bleeding and, sometimes, systemic symptoms possibly occurring1,4,6,14. In our case, we found local symptoms and growing abdominal pain but absence of systemic symptoms.
For the diagnosis, the imaging studies such as CT scan and ultrasound are useful but not specific and, in most cases, only confirming the presence of a mass14. The diagnosis is made by histology and by immunohistochemical and immunophenotyping studies. Morphologically, MS is characterized by diffuse proliferation of primitive myeloid cells with oval, irregular, reniform or folded nuclei, fine chromatin, distinct to proeminent nucleoli and scant to moderate cytoplasm1,8,20. The diagnostic accuracy is aided by immunohistochemical and immunophenotypic studies. According to the WHO classification of 2008, cytochemical colorations include chloroacetate esterase, myeloperoxidase and nonspecific esterase. The immunophenotypic panel may comprise CD68/KP1, MPO, CD117, CD99, CD68/PG-M1, lysozyme, CD34, TdT, CD56, CD61, CD30, glycophorin and CD4. This study can be performed in paraffin sections or by fluorescence activated cell sorting (FACS). The panel must be added with B and T lineage markers for differential diagnosis4,5,7. In the present case, we highlight the importance of obtaining a definitive diagnosis before any treatment procedures, in order to apply the most adequate systemic treatment and avoid inappropriate surgery which could cause disease dissemination7. In addition to these diagnostic elements, literature describes cytogenetic changes associated with MS in about 50% of the cases. The most frequent changes are inv(16) and involving chromosome 8 in particular, t(8; 21) (q22; q22), suggesting that the genomic changes are more frequent than previously characterized. The prevalence of MS in patients with t(8; 21) is about 9-35%. On the other hand, t(8; 21) is detected in 3.3-43% of patients with MS4,14. The cytogenetic study was inconclusive by lack of metaphasis.
The recommended treatment regimen in patients with isolated MS or concomitant with AML is the conventional AML chemotherapy protocols, based on evidence of a higher rate of progression to AML in isolated MS patients receiving localized treatment (88-100%), when comparing with patients given systemic chemotherapy (42%)4. Although, it is widely established that systemic treatment used to treat AML patients should be given to isolated MS patients, the optimal therapeutic option is still unclear7. Other therapeutic approaches such as post-remission treatment with external radiotherapy, as well as, hematopoietic cell transplantation, are, however, controversial1,4,7.
Due to the fact that MS is a rare disease, it is difficult to establish prognostic factors4. The data on the initial AML remission rate for patients aged 45-65 years is about 60%18. The isolated form of MS, appears to have a better prognosis than when it arises in association with AML or as relapse4. Cytogenetic abnormalities, such as t(8; 21), inv(16) and a good response to the initial treatment, both influence the prognosis positively14,19. Delay of the appropriate treatment has negative impacts on prognosis. If left untreated, on average, more than 50% of patients will develop AML in a short time period (5-11 months)6,7. In the present case, we expected a favourable prognosis because it was an isolated form of MS and it showed a favourable initial response to the therapy.
In conclusion, with this case report, the authors aim to highlight a rare form of AML presentation and its diagnostic process, where it was essential the gynaecological examination together with the laboratory and imaging studies, in order to make an accurate clinical judgement and define a diagnosis, as well as the correct treatment to improve the life of this patient.
REFERENCES
1. Bakst RL, Tallman MS, Douer D, Yahalom J. How I treat extramedullary acute myeloid leukaemia. Blood. 2011 Oct; 118, 3785-3794.
2. Vecchio R, Intagliata E, Fiumara PF, Villari L, Marchese S, Cacciola E. A rare case of myeloid sarcoma presenting the anal fissure. G Chir. 2015 Sep-Oct; 36, 222-224.
3. Alexiev BA, Wang W, Ning Y, Chumsri S, Gojo I, Rodgers WH, et al. Myeloid sarcomas: a histologic, immunohistochemical, and cytogenetic study. Diagnostic Pathology. 2007 Oct; 2, 42. [ Links ]
4. Avni B, Koren-Michowitz M. Myeloid sarcoma: current approach and therapeutic options. Ther Adv Hematol. 2011 Oct; 2(5), 309-316. [ Links ]
5. Campidelli C, Agostinelli C, Stitson R, Pileri SA. Myeloid sarcoma: extramedullary manifestation of myeloid disorders. Am J Clin Pathol. 2009 Sep; 132, 426-437. [ Links ]
6. Esper RC, Sánchez PE, Bermejo JM. Sarcoma granulocítico en una paciente con leucemia mieloide crónica. Revista de la Facultad de Medicina de la UNAM. 2012 Ene-Feb; 55(1), 22-28.
7. Yu Y, Qin X, Yan S, Wang W, Sun Y, Zhang M. Non-leukemic myeloid sarcoma Involving the vulva, vagina, and cervix: a case report and literature review. Onco Targets and Ther. 2015 Dec; 8, 3707-3713. [ Links ]
8. Garcia MG, Deavers MT, Knoblock RJ, Chen W, Tsimberidou AM, Manning JT, et al. Myeloid sarcoma involving the gynecologic - a report of 11 cases and review of the literature. Am J Clin Pathol 2006 May; 125, 783-790. [ Links ]
9. Gill H, Loong F, Mak V, Chan K, Au WY, Kwong YL. Myeloid sarcoma of the uterine cervix presenting as missed abortion. Arch Gynecol Obstet. 2012 Jul; 286, 1339-1341. [ Links ]
10. Ding J, Li H, Qi YK, Wu J, Liu ZB, Huang BC, et al. Ovarian granulocytic sarcoma of the primary manifestation of acute myelogenous leukaemia. Int. J Clin Exp Pathol. 2015 Oct; 8(10), 13552-13556. [ Links ]
11. Silva HF, Benevides VM, Ribeiro RM, Franck G; Castro AJM, Filho FDR, et al. Granulocytic sarcoma with skin and lymph node initial presentation. Rev Bras Hematol Hemoter. 2008 Feb; 30(1), 61-69. [ Links ]
12. Ruiz MAC, Oca AVM, Rubia MJB, Martín AAL. Disfonía y lumbalgia como presentación de sarcoma granulocítico. Primera manifestación de Leucemia Mieloide Aguda. Rev Clín Med Fam. 2009 Jun; 2(7), 368-370. [ Links ]
13. Seo IS, Hull MT, Pak HY. Granulocytic sarcoma of the cervix as a primary manifestation. Cancer. 1977 Dec; 40, 3030-3037. [ Links ]
14. Soto GG, Rincón JJP, Castaño JA, Torres JD, Gómez EI. Leucemia mieloide extramedular con compromiso endometrial: reporte de un caso y revisión de la literatura. Rev Colomb Obstet Gynecol. 2007 Jul-Sep; 58 (3), 245-248.
15. Hagen PA, Singh C, Hart M, Blaes AH. Differential diagnosis of isolated myeloid sarcoma: a case report and review of the Literature. Hematol Rep. 2015 Jun;7, 27-30. [ Links ]
16. Aguiar TGS, Oliveira IFL, Guimarães CVN, Adad, SJ, Moraes-Souza H. Sarcoma granulocítico multicêntrico como recidiva de leucemia mieloide aguda. Rev bras Hematol Hemoter. 2009 Jun; 31, 207-210. [ Links ]
17. Wang H, Wang H, Ma Q, Chen Y. Intracranial granulocytic sarcoma: two cases and literature review. Int J Clin Exp Med. 2015 Oct; 8(10), 19586-19590. [ Links ]
18. Hoffbrand AV, Moss PAH. Fundamentos em Hematologia. 6ª edição. Artmed. 2013. [ Links ]
19. Lichtman MA, Kaushansky K, Kipps TJ, Prchal JT, Levi MM. Williams Manual of Hematology, 8th edition. McGraw-Hill. 2010. [ Links ]
20. Kurman RJ, Carcangiu ML, Herrington CS, Young RH. WHO Classification of Tumours of Female Reproductive Organs. 4th edition. WHO. 2014. [ Links ]
21. Mayer RJ, Davis RB, Schiffer CA, Berg DT, Powell BL, Schulman P, et al. Intensive Postremission Chemotherapy in Adults with Acute Myeloid Leukaemia for The Cancer and Leukemia Group B. N Engl J M. 1994; 331, 896-903. [ Links ]
22. Wiernik PH, Banks PLC, Case Jr DC, Arlin ZA, Periman PO, Todd MB, et al. Cytarabine Plus Idarubicin or Daunorubicin as Induction and Consolidation Therapy for Previously Untreated Adult Patients With Acute Myeloid Leukaemia. Blood. 1992 January; 79, No 2, 313-319.
Endereço para correspondência | Dirección para correspondencia | Correspondence
Cláudia Meneses Alves
E-mail: menesesclaudia@gmail.com
Acknowledgements
The authors would like to thank Dra. Fernanda Caiano (gynaecologist), the first doctor to examine the patient and suspect the diagnostic, Dra. Isabel Macedo Pinto (pathologist) who, firstly, defined the anathomopathological diagnostic and Dra. Susana Félix (radiologist) for advising on some of the CT scan figures.
Recebido em: 12/05/2016
Aceite para publicação: 06/01/2017

