










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
versão impressa ISSN 1646-5830
Acta Obstet Ginecol Port vol.11 no.3 Coimbra set. 2017
CASE REPORT/CASO CLÍNICO
Posterior vaginal cyst: case report of an uncommon entity
Cisto da parede vaginal posterior: descrição de um caso com uma etiologia incomum
Pedro Viana Pinto*, Magda Magalhães**, Ana Rosa Costa***
Serviço de Ginecologia e Obstetrícia, Centro Hospitalar São João
*Interno de Formação Específica, Serviço de Ginecologia Obstetrícia, Centro Hospitalar São João; Unidade de Anatomia, Departamento de Biomedicina, Faculdade de Medicina, Universidade do Porto
**Interna Formação Específica, Serviço de de Ginecologia e Obstetrícia, Centro Hospitalar e Universitário de Coimbra
***Assistente Hospitalar Graduado, Serviço de Ginecologia Obstetrícia, Centro Hospitalar São João
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Vaginal cysts are uncommon and frequently diagnosed incidentally. A 20-year-old nulliparous woman, presented at her gynecologist for a routine appointment. An asymptomatic cystic mass on the posterior vaginal wall was found during physical examination. Surgical excision of the cyst was performed and pathological examination revealed a Mullerian cyst. These cysts usually arise at the level of cervix and extend anteriorly in relation to bladder, but very rarely they may also appear posteriorly. This paper illustrates a rare case of a posterior vaginal wall cyst of Mullerian origin.
Keywords: Mullerian Ducts; Vaginal wall; Immunohistochemistry.
Introduction
True cystic lesions of the vagina (excluding cysts arising from the urethra and surrounding tissues) are uncommon and they are usually an incidental finding during routine gynecological examination. Vaginal cysts are mainly classified according to their histology: 1) squamous inclusion cysts lined by stratified squamous epithelium more commonly located on the posterior wall, closer to an episiotomy repair or other surgical procedures; 2) mesonephric or Gartner's duct cysts lined by non-mucin-secreting low cuboidal cells usually located near the anterolateral wall of the vagina following the route of the mesonephric duct; 3) Mullerian or paramesonephric cysts lined by tall columnar mucin-secreting cells located anywhere in the vagina and grossly indistinguishable from mesonephric cysts; and 4) Bartholin's gland cysts arising from the Bartholin's gland duct located near the opening of the Bartholin's gland into the vestibule1,2. Among them, Mullerian cyst constitutes 30%, Bartholin duct cyst 27.5%, epidermal inclusion cyst 25% and remaining 17.5% is constituted by Gartner duct cyst, endometriotic cyst and unclassified type3. These cysts can vary in size and cause a variety of symptoms including a palpable mass, pain, dyspareunia, and voiding dysfunction. We describe a case of a woman with a vaginal cyst diagnosed during a routine gynecological examination.
Case report
A 20-year-old nulliparous woman presented at her gynecologist for a routine appointment. She had no relevant personal antecedents and denied any abnormal uterine bleeding, urinary or gastro-intestinal symptoms. At gynecological examination a soft, mobile cystic lesion with approximately 3 x 1,5 cm was found on the lower third of the posterior vaginal wall. There was no cough impulse on the mass and no pain was elicited by the examination. External genitalia was normal.
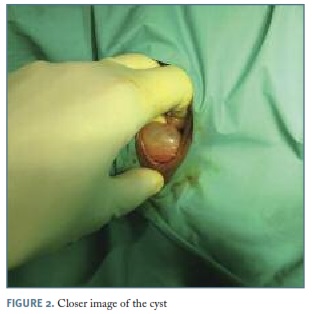
The patient underwent surgical excision of the cyst under general anesthesia (Figues 1 and 2). A small transverse incision was made on the posterior vaginal wall, which was separated from the cyst. During sharp and blunt dissection the cyst got accidentally ruptured and mucinous material drained out. The cyst wall was stripped away from vaginal wall and the cyst was totally removed, excess of vaginal mucosa was excised and the incision was closed with absorbable sutures. Patient had an uneventful post operative period and was discharged three hours after surgery.

Histological examination revealed a cyst lined by a single layer of tall columnar cells with mucin at the apex. The epithelium stained positive with mucicarmine and periodic acid-Schiff, confirming the clinical impression of a Mullerian cyst.
On her follow-up reviews, one month and 6 months after surgery, the woman had no complaints, with a normal gynecological examination.
Discussion
The vast majority of vaginal cysts are asymptomatic and require no treatment. Symptoms may vary according to cyst size, nature and location - patients may complain of vaginal discomfort, vaginal pressure, cyclic pain, dyspareunia, vaginal bleeding, and urinary or rectal symptoms.
In our patient differential diagnosis of a rectocele and enterocele were considered and ruled out by rectal examination, cyst location and by absence of cough impulse. The location of the cyst also ruled out a Bartholin cyst and the absence of cyclic pain and nature of the cyst excluded an endometriotic cyst. Inclusion cysts were excluded by absence of previous perineal lacerations or pregnancies. Due to its location, the most probable diagnosis was of a Mullerian cyst although a Gartner duct cyst was still a possibility.
Mullerian cysts are congenital cysts of vagina, usually single but occasionally multifocal4,5. During replacement of Mullerian epithelium with squamous epithelium of the urogenital sinus, Mullerian epithelial tissue can persist anywhere in the vaginal wall. As a consequence cysts can be found almost anywhere within the vaginal walls, being more commonly found on the anterolateral vaginal wall6,7. Cysts derived from the Mullerian ducts may exhibit histological patterns corresponding to those of any of the tissues normally derived from this duct, principally endocervical (the most common), tubal, or endometrial2,8,9. Occasionally, a Mullerian cyst may become sufficiently large to be symptomatic and warrant excision.
Gartner's duct cysts are less common than Mullerian cysts, are almost always located along the anterolateral wall of the vagina and typically are small, with an average diameter of 2 cm. Gartner's duct cysts can also be associated with abnormalities of the metanephric urinary system such as an ectopic ureter, unilateral renal agenesis, and renal hypoplasia6,8.
Although clinically irrelevant, Gartner's duct cysts may be distinguished from Mullerian cysts histologically by the presence of a basement membrane and smooth muscle layer. However, clear distinction between the two can be made only on the basis of histochemical staining, with paramesonephric cysts being periodic acid-Schiff and mucin positive, whereas mesonephric cysts are devoid of cytoplasmic mucin or periodic acid-Schiff positive material6.
Vaginal cysts are treated via surgical excision. The technique is similar for all cysts and the entire cyst wall must be removed in order to prevent recurrence.
In conclusion, this is an unusual case of a posterior vaginal cyst, an uncommon location for a Müllerian cyst. When evaluating a vaginal cyst, assessment of the lesion via history and pelvic examination is important for the differential diagnosis and decision making regarding treatment. When symptomatic, excision of the cyst is a simple procedure with total relief of symptoms.
REFERENCES
1. Pradhan S, Tobon H. Vaginal cysts: a clinicopathological study of 41 cases. Int J Gynecol Pathol. 1986;5:35-46. [ Links ]
2. Rashmi, A. S, N. A, K. G, P. Y. Vaginal mullerian cyst presenting as enterocele. J Obstet Gynecol India. 2009;59:74-76. [ Links ]
3. Kondi-Pafiti A, Grapsa D, Papakonstantinou K, Kairi-Vassilatou E, Xasiakos D. Vaginal cysts: a common pathologic entity revisited. Clin Exp Obstet Gynecol. 2008;35:41-44. [ Links ]
4. Wai CY, Corton MM, Miller M, Sailors J, Schaffer JI. Multiple vaginal wall cysts: diagnosis and surgical management. Obstet Gynecol. 2004;103:1099-102. [ Links ]
5. Hwang JH, Oh MJ, Lee NW, Hur JY, Lee KW, Lee JK. Multiple vaginal mullerian cysts: a case report and review of literature. Arch Gynecol Obstet. 2009;280:137-139. [ Links ]
6. Eilber KS, Raz S. Benign cystic lesions of the vagina: a literature review. J Urol. 2003;170:717-722. [ Links ]
7. Fletcher SG, Lemack GE. Benign masses of the female periurethral tissues and anterior vaginal wall. Curr Urol Rep. 2008;9:389-396. [ Links ]
8. Montella JM. Vaginal mullerian cyst presenting as a cystocele. Obstet Gynecol. 2005;105:1182-1184. [ Links ]
9. Toz E, Sanci M, Cumurcu S, Ozcan A. Mullerian cyst of the vagina masquerading as a cystocele. Case Rep Obstet Gynecol. 2015;2015:376834. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Pedro Viana Pinto
Rua Padre Arnaldo Rebelo 32, Vermoim
4470-249 Maia
E-mail: pedrovianapinto@gmail.com
Recebido em: 15/08/2016
Aceite para publicação: 22/02/2017

