










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
versão impressa ISSN 1646-5830
Acta Obstet Ginecol Port vol.14 no.1 Coimbra mar. 2020
CASE REPORT/ CASO CLÍNICO
Abdominal pregnancy with a live fetus - a case report
Gravidez abdominal evolutiva - um caso clínico
Ana Edral1, Fernanda Vilela1, Ângela Ferreira2
Centro Hospitalar Universitário do Algarve - Faro
1 Interno de Formação Específica de Ginecologia e Obstetrícia
2 Assistente Hospitalar de Ginecologia e Obstetrícia
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Abdominal pregnancy is a rare condition defined by the implantation of the embryo in the peritoneal cavity, exclusive of tubal, ovarian or intraligamentary pregnancy. It is a rare event with high maternal morbidity and mortality. The authors report the case of a secondary abdominal pregnancy with a live fetus at 10 weeks of pregnancy.
Keywords: Abdominal pregnancy; Ectopic pregnancy.
Introduction
Ectopic pregnancy occurs when the embryo implants outside the endometrial cavity. The most common implantation site is the fallopian tube (98%). Less frequent sites of implantation are the ovary, cervix, cesarean section scar, abdominal cavity and interstitial portion of the fallopian tube1.
Abdominal pregnancy (AP) is a rare obstetric condition, occurring in only 1% of ectopic pregnancies, and it has a reported incidence of 1:10000 to 1:30000 pregnancies2. Abdominal pregnancies are further classified as primary or secondary, with the latter being the most common type. Risk factors for AP are the same as for other types of ectopic pregnancy: previous ectopic pregnancy, smoking, history of sexually transmitted diseases, prior pelvic infection, spontaneous abortion, advanced maternal age, assisted reproduction techniques and intra-uterine device1.
The access to medical care and the generalized use of ultrasonography have allowed the early diagnosis of these pregnancies, avoiding the serious risks it represents to the pregnant woman. Yet there are cases of late diagnosis of AP, which pose a risk of maternal and fetal morbidity and mortality. Reported maternal mortality rate is 0.5-8% and the perinatal mortality, 40-95%3.
The authors report a case of a secondary abdominal pregnancy diagnosed at 10 weeks.
Thirty-six-year-old caucasian woman, healthy, with a previous right salpingectomy due to a tubal pregnancy, gravida 2, para 0, reporting a 11 weeks amenorrhea, complained of intermittent vaginal bleeding.
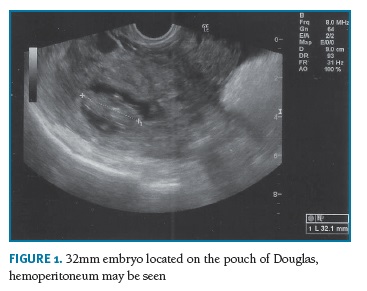
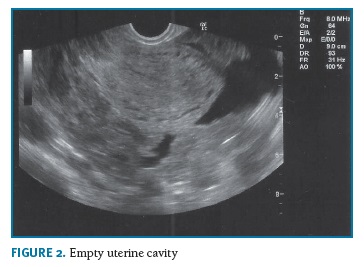
When she reached the obstetrics emergency service, pallor and dehydration were observed, but the vital signs were stable. She had a scant hematic vaginal discharge and she mentioned pain on bimanual examination, no masses were palpated. On the ultrasound, the uterus had a regular endometrial lining with an empty endometrial cavity and there was a moderate hemoperitoneum and blood clots on the pouch of Douglas. A live 32mm embryo was identified in the pouch of Douglas (Figures 1 and 2), with no identifiable myometrium seen around it. One normal appearing ovary was clearly identified on the ultrasonography. Hemoglobin was 9.8g/L (normocytic, normochromic anemia), platelets and coagulation profile were within normal limits.
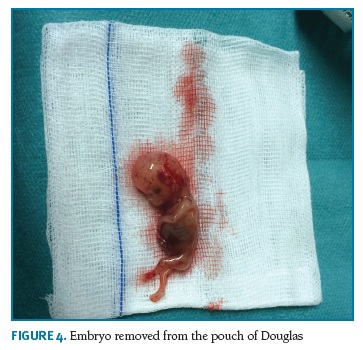
An emergent laparotomy was performed. During the surgery, an abundant hemoperitoneum was present. Uterus was of normal size and the right fallopian tube was not identified (previous salpingectomy), on the left tube, a placenta was attached to its distal extremity with an embryo floating on the pouch of Douglas. A left salpingectomy (Figures 3 and 4) was performed. During the procedure, the patient needed blood transfusions due to a severe anemia (hemoglobin = 5.4g/L). There were no complications on the post-surgery recovery. The patient was discharged two days later.

Histopathological examination confirmed the diagnosis of tubal ruptured ectopic pregnancy.
Discussion
Abdominal ectopic pregnancy is classified as primary, when the blastocyst implants directly in the peritoneal cavity. Primary abdominal pregnancy is very rare. Studdiford established three criteria for the diagnosis of primary peritoneal pregnancy: (1) normal bilateral fallopian tubes and ovaries, (2) the absence of uteroperitoneal fistula and (3) a pregnancy related exclusively to the peritoneal surface, early enough to discard the possibility of secondary implantation4. Secondary abdominal pregnancies occur when the blastocyst implants in the fallopian tube, ovary or uterus and, following rupture, the embryo or fetus continues to grow in the abdominal cavity5. The most frequent type of EP is secondary to a previous tubal pregnancy6.
The reported case suggests a primary tubal pregnancy which progressed to an abdominal pregnancy due to the rupture of the tube. The embryo survived in the pouch of Douglas and fetal heart frequency was still positive until the surgery was performed.
The clinical presentation apparently with no abdominal pain is rare, particularly if taken in consideration the large hemoperitoneum. In secondary EP, since they are a consequence of the rupture of a tubal pregnancy, there may be an history of spotting and irregular bleeding, with abdominal pain. Other symptoms of EP are gastro-intestinal symptoms such as nausea, vomiting, flatulence or constipation6. Advanced pregnancy may present with fetal malpresentation, cervix displacement, failure of spontaneous onset of labor. Maternal death may ensue due to acute hemorrhage and hemorrhagic shock3. Later in pregnancy, small fetal parts may be palpated on the vaginal fornices or identified outside the uterus3.
The clinical presentation and severity of symptoms depend on the pregnancy location and evolution time7. Ultrasonography, magnetic resonance imaging or computed tomography may help in the diagnosis of EP and to differentiate a primary from a secondary EP. Approximately 50% of diagnosis are missed on ultrasound3,6. On early pregnancy ultrasonography it is possible to identify an empty endometrial cavity, eventually with a pseudosac, signs of hemoperitoneum and a fetus or embryo within the abdominal cavity. On later stages of pregnancy, the diagnosis of AP requires a high index of suspicion. The ultrasonographic examination may not be enough to clarify this diagnosis and, in these cases, MRI or CT should be done.
A precocious diagnosis is essential to avoid risks and treat the patient with fewer dismal consequences. Proper pre-operative evaluation can help with the diagnosis and to choose the best approach to minimize maternal complications. Treatment is defying since there are multiple possible implantation sites. Surgery is the most frequent choice; however, intervention radiology or pharmacological methods may be necessary, especially in the case of a primary EP when the complete removal of the placenta may be impossible during the surgery.
Expectant management is contra-indicated. When there is a diagnosis of EP, immediate surgery is required to remove the embryo and to reduce associated morbimortality6. In this case, the surgeons decided for a laparotomic approach due to the large hemoperitoneum. The diagnosis was confirmed during the surgery and on the histological examination. The main maternal complication was the anemia, needing blood transfusion, one of the well-known complications of this pregnancy described in medical literature. In this case, rapid surgery avoided maternal death due to hemorrhagic shock.
Abdominal pregnancy is a rare condition but in the presence of atypical complains in a pregnant woman there should be a high suspicion for pregnancy complications as this one. The precocious and adequate treatment make the difference on maternal outcomes.
REFERENCES
1. Panelli DM, Phillips CH, Brady PC. Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies: a review. Fertil Res Pract. 2015;1:15. [ Links ]
2. Nagamuthu EA, Fatima SS. Secondary abdominal pregnancy: a case report. Int J Res Med Sci. 2014;2(2):779-781 [ Links ]
3. Sharma E, Khateja R, Agarwal R, Suneja A, Sharma A. Secondary Abdominal Pregnancy: A Rare Presentation. Journal of South Asian Federation of Obstetrics and Gynaecology. 2015;7(3):243-244. [ Links ]
4. Studdiford WE. Primary peritoneal pregnancy. Am J Obstet Gynecol. 1942;44(3).
5. Shanbhag A, Singh A. Secondary Intra-Abdominal Pregnancy: A Case Report. Nepal Journal of Obstetrics and Gynaecology. 2011;6(2):44-46. [ Links ]
6. Gupta P, Sehgal A, Huria A, Mehra R. Secondary abdominal pregnancy and its associated diagnostic and operative dilemma: three case reports. J Med Case Rep. 2009; 3:7382. [ Links ]
7. Leite TS, Almeida DC, Viseu O, Dias J. Is it really an adnexal ectopic pregnancy? An atypical presentation. Acta Obstétrica e Ginecológica Portuguesa. 2018;12(3):220-223. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Ana Edral
E-Mail: edral.ana@gmail.com
Recebido em: 28/08/2019
Aceite para publicação: 13/03/2020

