










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkActa Obstétrica e Ginecológica Portuguesa
versão impressa ISSN 1646-5830
Acta Obstet Ginecol Port vol.14 no.3 Coimbra set. 2020
ESTUDO ORIGINAL/ ORIGINAL STUDY
The impact of maternal working conditions on fetal weight: a risk factor for fetal growth restriction?
O impacto das condições de trabalho maternas no peso fetal: um fator de risco para restrição de crescimento fetal?
Vera Trocado1,2,3*, Carla Rodrigues1,4*, Paula Pinheiro3, Isabel Reis5, Cristina Nogueira Silva1,2,5
Serviço de Ginecologia e Obstetrícia - Unidade Local de Saúde do Alto Minho - Viana do Castelo
Serviço de Ginecologia e Obstetrícia - Hospital de Braga
*Estas autoras contribuíram de igual forma para a realização deste trabalho
1 Interna de Formação Específica em Ginecologia e Obstetrícia, Serviço de Ginecologia e Obstetrícia, Unidade Local de Saúde do Alto Minho, Viana do Castelo, Portugal; Assistente convidada na Escola de Medicina, Universidade do Minho, Braga, Portugal; Investigadora no Instituto de Investigação em Ciências da Vida e da Saúde/3B’s - Laboratório Associado do Governo Português, Braga/ Guimarães, Portugal
2 Interna de Formação Específica em Cardiologia, Serviço de Cardiologia, Hospital de Braga, Braga, Portugal
3 Diretora do Serviço de Ginecologia e Obstetrícia, Serviço de Ginecologia e Obstetrícia, Unidade Local de Saúde do Alto Minho, Viana do Castelo, Portugal
4 Diretora do Serviço de Ginecologia e Obstetrícia, Serviço de Ginecologia e Obstetrícia, Hospital de Braga, Braga, Portugal
5 Assistente Hospitalar de Ginecologia e Obstetrícia, Serviço de Ginecologia e Obstetrícia, Hospital de Braga, Braga, Portugal; Professor Auxiliar na Escola de Medicina, Universidade do Minho, Braga, Portugal. Investigadora no Instituto de Investigação em Ciências da Vida e da Saúde/3B’s - Laboratório Associado do Governo Português, Braga/ Guimarães, Portugal.
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Overview and aims: Several risk factors for fetal growth restriction (FGR) have been described, however the impact of maternal working conditions is still poorly understood. To evaluate the impact of type of transport used, travel time, weekly hours of work, shift work, posture, environmental conditions, physical load and occupational stress on fetal weight.
Study design and population: A case-control study was conducted. All professionally active pregnant woman that attended during 3rd trimester a pregnancy surveillance consultation at two Portuguese public hospitals during 4 months were included. The population was divided in two groups: FGR group - fetuses with estimated fetal weight (EFW) below the 10th percentile at 3rd trimester ultrasound; control group - fetuses with EFW equal to or higher than 10th percentile at 3rd trimester ultrasound.
Methods: Data about working conditions, anthropometric and sociodemographic characteristics were collected using a questionnaire and the occupational stress questionnaire-general version (QSO-VG). Data on obstetric characteristics was acquired from clinical records. Data analysis was performed using SPSS ®, version 22.0.
Results: There were 50 pregnant women in the FGR group and 295 in the control group. A predictive model of FGR was developed including 5 variables - sitting for at least 3 hours, high occupational stress levels, work by shifts, shifts with daytime and night rotation and load or lift weights greater than or equal to 25 Kg - with high specificity (98,5%), a positive predictive value of 85.7% and a negative predictive value of 74.2%, but with a low sensitivity (20.7%).
Conclusions: This study showed that maternal working conditions can be important predictors of FGR.
Keywords: Pregnancy; Maternal working conditions; Fetal weight; Fetal growth restriction.
Introduction
Fetal growth restriction (FGR) is defined by fetuses that have not reached their growth potential. This term is more commonly used to describe fetuses with a weight below the 10th percentile for gestational age1. Globally, in a multiethnic society, we could expect 10% of fetuses to be present impairment on fetal growth, which can have overlapping placental, maternal or fetal contributions2. The use of a percentile to define FGR difficults the distinction between FGR and small for gestational age fetus. FGR is associated with an increase in the risk of stillbirth, neonatal morbidity and mortality, neurocognitive impairment, as well as increased risk of metabolic disorders development such as obesity, diabetes or coronary heart disease in adulthood3,4. Being such a prevalent condition, FGR can pose an important public health burden, which makes it essential to study its predisposing factors.
Currently, there are several well-known risk factors, such as low maternal birth weight, maternal malnutrition, low weight gain during pregnancy, extremes of maternal age, history of FGR in a previous pregnancy, hypertensive disorders, diabetes, antiphospholipid syndrome or acquired thrombophilias5-8. Nonetheless, impact of the maternal working conditions during pregnancy on fetal birth weight is still an understudied and particularly controversial subject in the literature9-15.
Given the drastic change of women's role in society, this issue is actually very important. Pregnant women are exposed to daily challenges associated with the profession and despite the lack of consistent evidence to support the recommendation of restriction of some professional activities, several worldwide working condition authorities recommend adjusting professional environment during the gestational period16-17. Therefore, the aim of this study is to evaluate the impact of maternal working conditions - type of transport used, travel time, weekly hours of work, shift work, posture, environmental conditions, physical load and occupational stress - on fetal weight. As a secondary objective, the authors intend to develop a predictive model of fetuses with FGR, according to maternal working conditions.
Methods
An observational, case-control study was developed. All professionally active pregnant woman that attended a pregnancy surveillance consultation during 3rd trimester at two portuguese public hospitals over the course of 4 months (between july and october 2016) were eligible. The population was divided in two groups: FGR group - fetuses with estimated fetal weight (EFW) below the 10th percentile at 3rd trimester ultrasound; control group - fetuses with EFW equal to or higher than 10th percentile. EFW was calculated with 4-parameter Hadlock formula, and percentiles were based on Yudkin et al. curves18-19. Exclusion criteria applied were: extremes of maternal age (less than 18 or more than 40 years of age), multiple pregnancy, exposure to teratogenic drugs, tobacco, alcohol or drug users, chronic or gestational hypertension, preeclampsia/eclampsia, previous diabetes, acquired thrombophilia, antiphospholipid syndrome, gestational body mass index inferior to 18,5 Kg/m2, previous diagnosis of malaria or TORCH group infections, chromosomal defects or incomplete information on clinical records. A questionnaire and the occupational stress questionnaire-general version (QSO-VG), developed and validated for Portuguese population, were applied to the target population20. The questionnaire was submitted as a pilot study with answers from 40 pregnant women. There were no suggestions of improvement. This instrument intended to obtain information about sociodemographic characteristics (date of birth, age, marital status, education, employment status), anthropometric data (pre-pregnancy weight, current weight and height), lifestyle during pregnancy and professional conditions. Regarding this, the evaluated conditions were: type of transport used to go to the work, travel time, number of weekly working hours, shift work, shifts alternating with daytime and night, posture (orthostatic posture, percentage of time in the same place in the standing posture, sitting, squatting), environmental conditions (perception of temperature, noise) and physical load (load or lift weights greater than or equal to 25 Kg). The QSO-VG evaluates 7 different categories of psychological stress: the relationship with users, managers or colleagues, work overload, concerns about the career and remuneration, family problems enhanced by occupation and working conditions. The application of the instruments occurred in a single contact with the subject, 10 minutes before the 3rd trimester pregnancy surveillance consultation. Additional information was collected through clinical records, including personal medical history and present and past obstetric data. The anonymity of participants and data confidentiality were guaranteed. The study was authorized by the Ethics Subcommittee for the Life Sciences and Health of University of Minho and by the Ethics Committees of both hospitals. The statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) ®, Chicago, Illinois, USA, version 22.0. A descriptive analysis, with measures of central tendency and dispersion, appropriate to the variables, was initially performed. In the quantitative variables normality was analyzed using the Kolmogorov-Smirnov test and when this was significant (p <0.05), normality was assessed by asymmetry and the kurtosis of the histogram plot. The asymmetry reference values and kurtosis used were from -2 to +2. Then, it was assured that there were no statistically significant differences in the sociodemographic, obstetric and anthropometric characteristics between the two groups, by t-test for independent samples (age, height), chi-square test (educational level, temporary sickness leave, pregnancy BMI) or Fisher's exact test (marital status, professional group, pre-pregnancy BMI, parity, fetal weight percentile < 10 in a previous pregnancy) according to the different variables. Secondly, it was performed an univariate analysis that evaluated the association between “professional standards and EFW by chi-square test or Fisher's exact test. Finally, a multivariate analysis was done applying a binary logistic regression, by the Enter method, being the dependent variable “FGR” (present or absent). Independent variables were selected according to professional parameters that showed a statistically significant association with EFW in the univariate analysis and professional standards outlined in the current literature. The inclusion of the variables found in the literature was supported by comparing the ROC curves of two models: with or without these variables. The drawing and comparison of ROC curves was performed using MedCalc Software®. The significance level was set at 0.05, with a 95% confidence interval.
Results
During the period of the study 402 women were sequentially recruited, of which 345 met the inclusion criteria. 295 (85.5%) had normal EFW and 50 (14.5%) had FGR. In order to respect a proportion of 2:1, the randomization of 100 of 295 pregnant women in the control group was performed, using SPSS®. Thus, the final sample consisted of 100 (66.7 %) pregnant women in the control group (normal EFW) and 50 (33.3 %) pregnant women in the study group (FGR).
Sociodemographic, anthropometric and obstetric characteristics are shown in Table I. There were no statistically significant differences between the two groups regarding these parameters, except temporary sickness leave. Indeed, the study group presents a higher frequency of sickness leave than the control group (52% vs. 32 %; p= 0.018). Moreover, the study group presents a higher frequency of previous pregnancy with a birth weight below the 10th percentile, but this difference was not statistically significant (12.5% vs. 4%; p= 0.32).
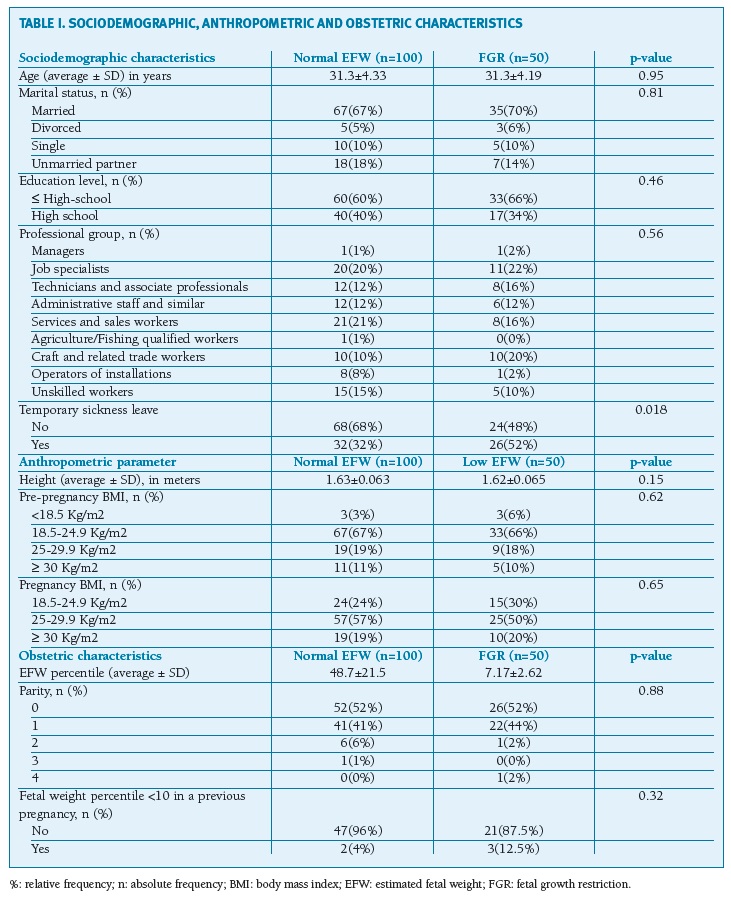
(clique para ampliar ! click to enlarge)
Regarding the relation between maternal professional parameters and EFW (Table II), a statistically significant association with the sitting position was found (p= 0.047). The study group had a higher frequency of pregnant women that are 3 or more hours in a sitting position (79.3%) compared to the control group (58.2 %). High occupational stress evaluated with QSO-VG also showed a statistically significant association with FGR, with the study group having a higher frequency of pregnant women that have high occupational stress levels (22% vs. 4%; p= 0.001). Furthermore, shifts with daytime and night rotation showed a possible association with FGR, although not statistically significant (p=0.073). There were no other statistically significant results regarding to other professional parameters.
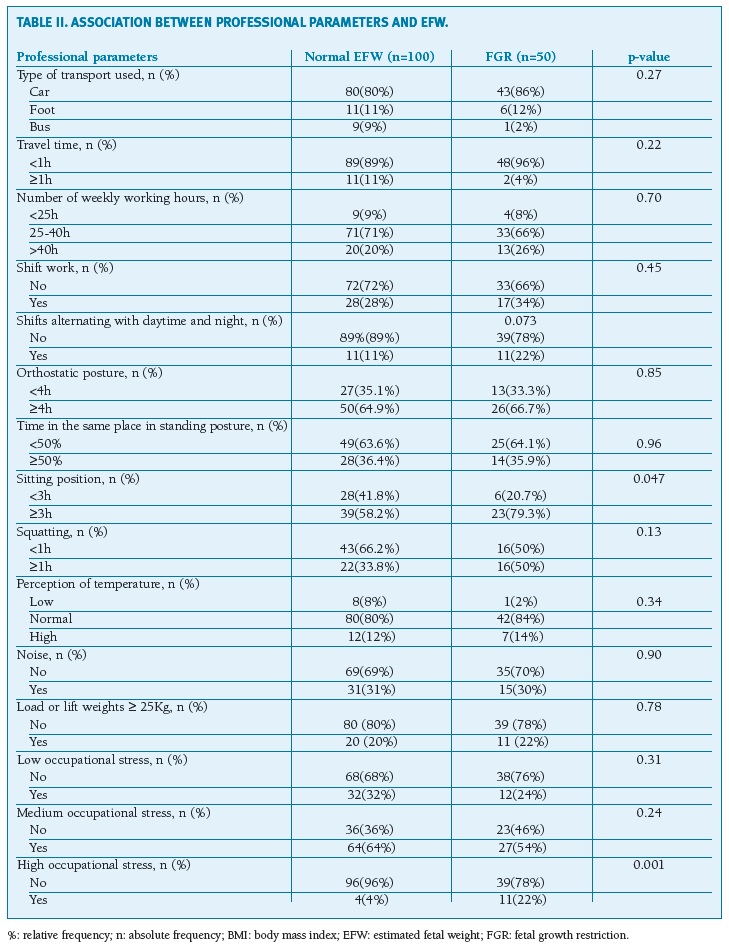
(clique para ampliar ! click to enlarge)
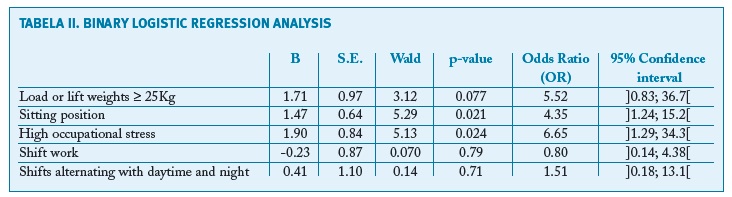
A binary logistic regression model was performed to evaluate the impact of professional standards in the probability of a pregnant woman to have a fetus with weight below the 10th percentile. Five independent variables were included - sitting position, high occupational stress, work by shifts, shifts with daytime and night rotation and load or lift weights greater than or equal to 25 Kg. In the selection of the independent variables were included the two variables that had a statistically significant association with EFW in the univariate analysis - sitting position and high occupational stress - and the professional standards outlined in the current literature - shift work, shifts with daytime and night switching and load or lift weights equal to or greater than 25 Kg. The obtained model is statistically significant (χ2 (5, N = 96) = 13.8; p= 0.017) and explained between 13.4% to 19% of the dependent variable variation. It has a low sensitivity (20.7%) and a high specificity (98.7%), classifying correctly 75% of the cases. The Hosmer and Lemeshow test showed a good data setting (χ2 (4) =0.56, p= 0.98).Table III shows that high occupational stress (B high occupational stress= 1.9; X2 Wald = 5.13, p = 0.024; OR = 6.65) and sitting position (Bsitting position= 1, 47; X2 Wald = 5.29; p = 0.021; OR = 4.35) had a statistically significant effect. The variable load or lift weights greater than or equal to 25 Kg (B load or lifting weights ≥ 25Kg = 1.71; X2 Wald= 3.12; p = 0.077; OR = 5.52) showed a possible association with FGR, although not statistically significant. The variables shiftwork and shifts with daytime and night switching did not show statistical significance. As an example, sitting position for 3 or more hours increased 4.35 times the risk of a pregnant woman having a fetus weighting below the 10th percentile. Additionally, high occupational stress increased 6.65 times the risk of a pregnant woman having a fetus weighting below the 10th percentile. Loading or lifting weights equal to or greater than 25 Kg increased 5.52 times the risk of a pregnant woman having a fetus with growth restriction.
(clique para ampliar ! click to enlarge)
The ROC curve of the binary logistic regression model provided an adequate quality model adjustment (AUC= 0.70, SE= 0.053, p< 0.001, CI= 0.59 to 0.79). (Figure 1)

Discussion
The main results of this study suggest that the risk of FGR increases if, in the employment context, pregnant women remain seated for 3 or more hours (OR= 4.35, p= 0.021) or demonstrate high occupational stress levels (OR= 6.65, p= 0.024). Carrying or lifting weights equal to or greater than 25 Kg showed a possible association with FGR (OR= 5.52, p= 0.077), however this effect is not statistically significant. The obtained regression model had a sensitivity of 20.7%, specificity of 98.5%, a positive predictive value of 85.7% and a negative predictive value of 74.2%. Therefore, it is not adequate as a screening tool of FGR, but deserves attention.
The regression model included two variables that had a statistically significant association with EFW in the univariate analysis - sitting position and high occupational stress - and three other variables that were not associated with FGR in the univariate analysis, probably due to the small sample size. As they have an important role described in the literature, the authors considered important factors to include in the regression model.
The impact of professional work condition in fetal weight is a very controversial subject in literature. In 1996, Spinillo et al analyzed the impact of the number of working hours, prolonged orthostatic posture and physical activity on fetal weight, concluding that the high physical exertion potentiated an increased risk of low birth weight9. This was corroborated by a meta-analysis written by Mozurkewich et al in 200010. Additionally in 2005, Takito et al stated that psychological stress associated to work can have an impact on fetal weight11. More recently, in 2016, Lee et al demonstrated that high levels of occupational physical activity were significantly associated with small for gestational-age babies and were also associated with preterm birth12. The present results are in line with these studies. However, there is also some evidence pointing in the opposite way. In 2009, Bonzini et al described the lack of association between fetuses with FGR and prolonged orthostatic posture, shift work or the number of working hours13. Even so, the same author in 2011, in a systematic review of the impact of shift work on several obstetric complications, highlighted that this variable may be associated with an increased risk of fetuses with low estimated weight14. In 2010, Burdorf et al assessed the impact of carrying weights of more than 5 Kg or more than 25 Kg, of sitting or standing positions and exposure to toxic agents, concluding that carrying weights over 5 Kg decreased the risk and exposure to pesticides increased the risk of low birth weight15. The pathophysiological mechanisms behind the proposed associations are not fully understood. Prolonged sitting position promotes a decrease in cardiac output with consequent reduction of uteroplacental circulation and fetal nutrition. The decrease in cardiac output can be explained by compression of inferior vena cava by the gravid uterus in the sitting position21. High stress levels resulting from fatigue, physical load or psychological stress, enhance a reduction in gestational time and fetal weight, with the main mediators being the sympathetic nervous system and the hypothalamic-pituitary-adrenal (HPA) maternal axis. Thus, at short term there is activation of the maternal sympathetic nervous system which causes the release of catecholamines22. At long term, there is activation of the maternal HPA axis and increase of corticotropin releasing hormone (CRH), which leads to the release of oxytocin and prostaglandins F2α and E2 in human placental tissue cultures contributing to the occurrence of preterm labor23. Additionally, CRH increases glucocorticoid levels, that synergistically with catecholamines, decrease uteroplacental blood flow and fetal nutrition24. Regarding to the effect of shift work on fetal weight, disturbances in the circadian rhythm and the change in amplitude of serum melatonin are proposed mechanisms25. Moreover, sleep deprivation has negative effects on pregnancy through neuroendocrine, immune, vascular or behavioral mechanisms24.
In this study, carrying or lifting weights equal or greater to 25 Kg has some association with FGR, although the results are not statistically significant, probably due to reduced sample size. As previously described, it may be explained by increased catecholamine production, which enhance uterine contractility and vasoconstriction, reducing the uteroplacental blood flow25,26. It is essential to note that more clinical and molecular studies are necessary in order to clarify the underlying mechanism between these associations.
This study has some limitations that should be pointed out: the incidence of FGR was slightly greater (14,5%) than the described in the literature (10%), probably due to the fact that it is a small sample, limited to a short period of time (4 months). The curves used (Yudkin et al.) are not adjusted to the population, also contributing to this point. The use of curves adjusted to the Portuguese population could help to obviate this limitation27. Some confounding factors, such as maternal prematurity, low maternal weight at birth and maternal obstetrical history of perinatal death were not adjusted. In addition, these findings are also hampered by the simplistic evaluation of maternal professional parameters, since for instance the duration, frequency and posture while carrying or lifting loads were not evaluated. Also in this study we didn’t evaluate the impact of the physical activity performed outside the workplace. Recently, there are a few recommendations of international societies (FIGO, ACOG) about policies to reduce occupational exposure to chemicals/toxics during pregnancy16,17. However, there is limited counseling or policy about working conditions, particularly those explored in this article, probably due to the lack of clear and consistent scientific results. Moreover, the scarce recommendations are mostly based on the association between working conditions and the risk of miscarriage or preterm delivery and not the impact on fetal weight28-32. In this respect, this study is a warning to employers and working condition authorities and a tip-off to conduct studies on a larger scale and with a more complex assessment of professional standards, that could support the legal regulation about this issue.
REFERENCES
1. Battaglia FC, Lubchenco LO. A practical classification of newborn infants by weight and gestational age. J Pediatr 1967; 71:159 [ Links ]
2. Lee AC, Kozuki N, Cousens S, et al. Estimates of burden and consequences of infants born small for gestational age in low and middle income countries with INTERGROWTH-21st standard: analysis of CHERG datasets. BMJ. 2017;358:j3677. [ Links ]
3. Pallotto E, Kilbride H. Perinatal Outcome and Later Implications of Intrauterine Growth Restriction. Clin Obstet 2006; 49(2): 257-269. [ Links ]
4. Barker D. Adult Consequences of Fetal Growth Restriction. Clin Obstet Gynecol 2006; 49(2): 270-283. [ Links ]
5. Kramer M. Determinants of low birth weight: methodological assessment and meta-analysis. Bull World Health Organ 2987; 65(5): 663-737. [ Links ]
6. Yunis K, Beydoun H, Tamim H. Maternal predictors of small-for-gestational age in uncomplicated births. Int J Gynaecol Obstet 2002; 79(1): 33-35. [ Links ]
7. Valero J, Soriano T, Albaladejo R, et al. Risk factors for low birth weight: a review. Eur J Obstet Gynecol Reprod Biol 2004;116(1): 3-15. [ Links ]
8. ACOG Practice Bulletin No.134. Fetal Growth Restriction. Obstet Gynecol 2013;121:1122-1133.
9. Spinillo A, Camusso E, Altar F, et al. The effect of work activity in pregnancy on the risk of fetal growth retardation. Acta Obstet Gynecol Scand 1996; 75(6): 531-536. [ Links ]
10. Mozurkewich E. Working conditions and adverse pregnancy outcome: a meta-analysis. Obstet Gynecol 2000; 95(4): 623-635. [ Links ]
11. Takito M, Benício M, Latorre, M. Postura materna durante a gestação e sua influência sobre o peso ao nascer. Revista De Saude Publica 2005; 39(3):325-332. [ Links ]
12. Lee L, Symansky E, Lupo P, et al. Role of maternal occupational physical activity and psychosocial stressors on adverse birth outcomes. Occupy Environ Med 2017; 74(3):192-199. [ Links ]
13. Bonzini M, Coggon D, Godfrey K, et al. Occupational physical activities, working hours and outcome of pregnancy: findings from the Southampton Women's Survey. Occup Environ Med 2009; 66(10):685-690. [ Links ]
14. Bonzini M, Palmer K, Coggon D, et al. Shift work and pregnancy outcomes: a systematic review with meta-analysis of currently available epidemiological studies. BJOG 2011;118(12): 1429-1437. [ Links ]
15. Burdorf A, Brand T, Jaddoe V, et al. The effects of work-related maternal risk factors on time to pregnancy, preterm birth and birth weight: the Generation R Study. Occup Environ Med 2010; 68(3):197-204. [ Links ]
16. Di Renzo G, Conry J, Blake J, et al. International Federation of Gynecology and Obstetrics opinion on reproductive health impacts of exposure to toxic environmental chemicals. Int J Gynaecol Obstet 2015;131:219-225. [ Links ]
17. ACOG Committee Opinion No. 575. Exposure to toxic environmental agents. Obstet Gynecol 2013;122(4):931-935.
18. Hadlock FP, Harrist RB, Carpenter RJ, Deter RL, Park SK. Sonographic estimation of fetal weight. The value of femur length in addition to head and abdomen measurements. Radiology 1984;150:535-540. [ Links ]
19. Yudkin PL, Aboualfa M, Eyre JA, Redman CWG, Wilkinson AR. New birthweight and head circumference centiles for gestational ages 24 to 42 weeks. Early Hum Dev 1987;15:45-52. [ Links ]
20. https://www.psi.uminho.pt/pt/CIPsi/Unidades_Investigacao/ARDH-GI/PublishingImages/Paginas/Stress_Ocupacional/Question%C3%A1rio%20de%20Stress%20Ocupacional%20%E2%80%93%20Vers%C3%A3o%20Geral.pdf. Accessed January 2015 [ Links ]
21. Blackburn S. Maternal, Fetal & Neonatal Physiology 4thedition. Elsevier Saunders 2012: 252-297. [ Links ]
22. Ventura T, Neto M, Simões M. Efeitos do Stress durante a gravidez na morfologia cerebral do feto e da criança. Uma revisão. Progr Diag Trat Prenat 2009; 21(2):77-84. [ Links ]
23. Reis F. Putative role of placental corticotropin-releasing factor in the mechanisms of human parturition. J Soc Gynecol Investig 1999; 6(3):109-119. [ Links ]
24. Romero R, Espinoza J, Gotsch F, et al. The use of high-dimensional biology (genomics, transcriptomics, proteomics, and metabolomics) to understand the preterm parturition syndrome. BJOG 2006;113:118-135. [ Links ]
25. Tamura H, Nakamura Y, Terron M, et al. Melatonin and pregnancy in the human. Reprod Toxicol 2008;25(3):291-303. [ Links ]
26. Palmer K, Bonzini M, Bonde J. Pregnancy: occupational aspects of management: concise guidance. Clin Med (Lond) 2013;13(1):75-79. [ Links ]
27. Sousa-Santos R, Miguelote R, Cruz-Correia RJ, et al. Development of a birthweight standard and comparison with currently used standards. What is a 10th centile?. Eur J Obstet Gynecol Reprod Biol. 2016;206:184-193. DOI: 10.1016/j.ejogrb.2016.09.028. [ Links ]
28. Teixeira J, Fisk N, Glover V. Association Between Maternal Anxiety in Pregnancy and Increased Uterine Artery Resistance Index: cohort based study. BMJ 1999; 318(7177):153-157. [ Links ]
29. Florack E, Zielhuis G, Pellegrino J, et al. Occupational physical activity and the occurrence of spontaneous abortion. Int J Epidemiol 1993;22:878-884. [ Links ]
30. Whelan E, Lawson C, Grajewski B, et al. Work schedule during pregnancy and spontaneous abortion. Epidemiology 2007;18:350-355. [ Links ]
31 Beukering M, Van Melick M, Mol B, et al. Physically demanding work and preterm delivery: a systematic review and meta-analysis. Int Arch Occup Environ Health 2014;87:809-834. [ Links ]
32. Grajewski B, Rocheleau CM, Lawson CC, et al. “Will my work affect my pregnancy?”Resources for anticipating and answering patient’ questions. Am J Obstet Gynecol 2016; 214(5):597-602. [ Links ]
Endereço para correspondência | Dirección para correspondencia | Correspondence
Vera Trocado
Escola de Medicina da Universidade do Minho. Unidade Local de Saúde do Alto Minho
E-mail: veratrocado@med.uminho.pt
Conflicts of interest
The authors have no conflicts of interest.
Authors Contributions
CR and VT contributed to the conception and design of the study, the screening of articles identified in the literature search, data collection and analysis, and writing the manuscript. PP, IR and CNS contributed to the writing and revising of the manuscript.
Recebido em: 19/04/2020. Aceite para publicação: 16/06/2020

