











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
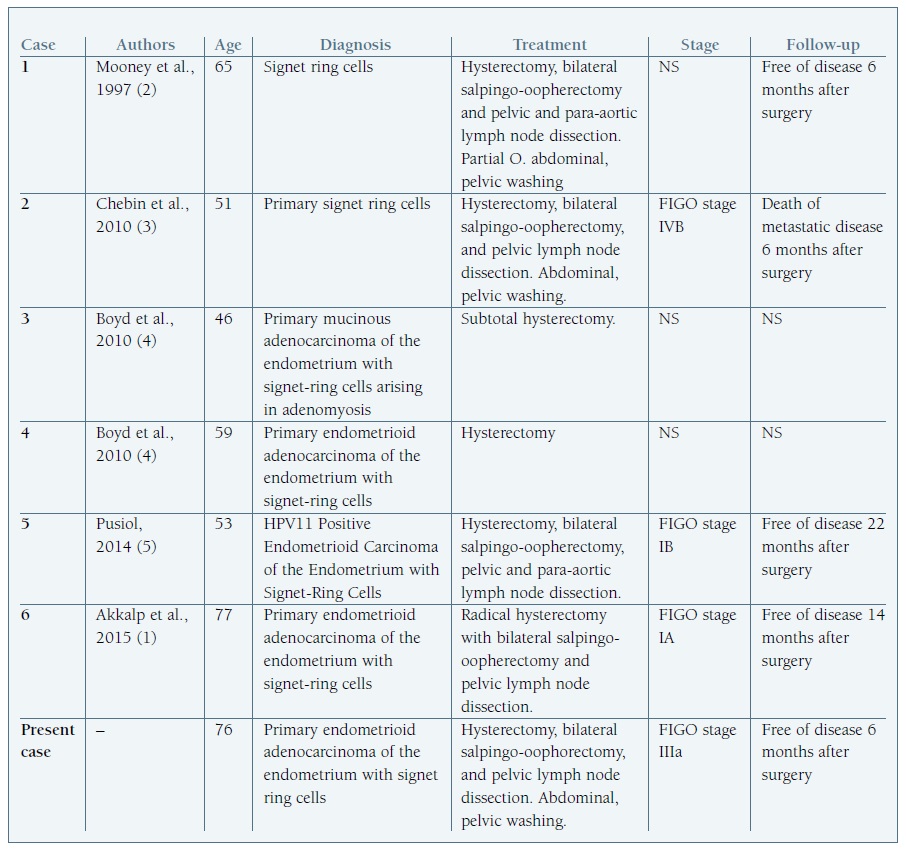
Signet ring cells are a common finding in endometrial metastatic adenocarcinoma with a non-genital primary tumour as the most probable diagnosis, namely, primary gastrointestinal or breast tumors. (1 However, despite being a rare condition, some cases of primary endometrial adenocarcinoma with signet ring cells have been reported in literature (Table I). (1), (2), (3), (4), (5), (6 This is, to our knowledge, the 7th case reported.
When this finding is present, primary non-genital origin of the tumour has to be excluded by extensive staging studies. Immunohistochemical staining may be helpful in confirming or ruling out endometrial origin. In fact, positive staining to cytokeratin 7 (CK7), vimentin and estrogen receptor (RE) support this diagnosis (Figure 1). (1), (7
Case report
A 76 year-old woman, G4P3 (vaginal deliveries), presented to the emergency department of Centro Materno Infantil do Norte, in Oporto, complaining of postmenopausal bleeding. She had no other complaints. She has the diagnosis of menopause since she was 50 years old and she did not take hormonal therapy. During evaluation, gynaecological examination showed to be normal and a vaginal ultrasound was done, revealing an endometrial thickness of 9,3 mm. An endometrial specimen was collected by endometrial biopsy performed with Novak system, whose anatomopathological examination was consistent with endometrial adenocarcinoma.
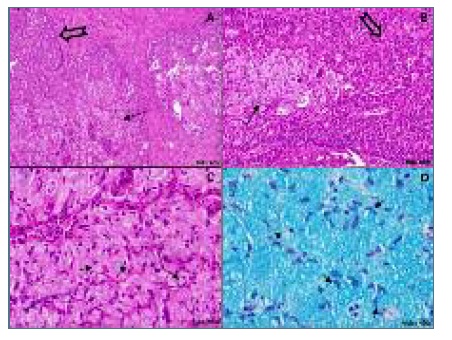
Radiologic and endoscopic evaluation did not showed any other tumour. The patient underwent abdominal total hysterectomy with bilateral adnexectomy. During the surgery, an extemporaneous anatomopathological evaluation showed more than 50% myometrium invasion justifying peri-aortic and peri-iliac lymph node dissection and peritoneal washing. The hysterectomy specimen consisted of uterus and cervix measuring 9x2,3 cm and weighting 70g, with attached bilateral adnexa. It was identified at the anterior surface of the endometrium a protruding plaque-like neoplasia measuring 3 cm in diameter that appeared to infiltrate the inner half of the myometrium wall in transverse section. Endocervix contained a pediculated polypoid mass of 1,5 cm and was not involved by the tumour. Adnexa were normal. Microscopic evaluation showed an endometrioid endometrial adenocarcinoma with signet ring cells and positive immunohistochemical staining for CK7, ER (focally), PAX-8 and vimentine. No endometrial hyperplasia was detected. An Alcian Blue staining highlighted the signet ring cells containing mucin (Figure 2). Pelvic wash was negative for malignant cells. Two of the 25 dissected lymph nodes showed metastasis. Final staging was consistent with a FIGO 3c1 stage and additional chemotherapy (carboplatine and paclitacel) and radiotherapy were proposed. The patient underwent 3 cycles of chemo-the-rapy and was doing well until the writing of this report. No recurrences have been reported.
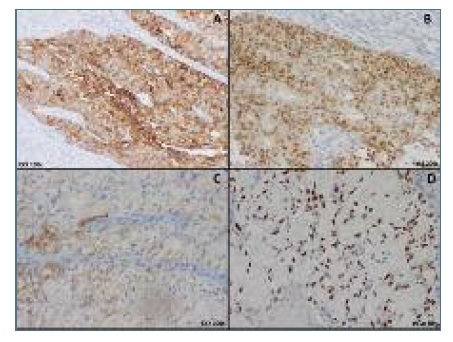
Figure 2 (A & B): Endometrioid adenocarcinoma with cribriform pattern, showing immunohistochemical positive staining for CK7 (cytoplasm) and Pax8 (nuclear); (C & D): Endometroid adenocarcinoma with signet ring cells showing immunohistochemical positive staining for CK7 (cytoplasm periphery) and for Pax8 (nuclear).
Discussion
Endometrium is rarely affected by metastasis of non-gynaecological malignancies. The first case of endometrial metastasis was reported in 1878 by Legg et al. (1), (2 Since then more cases have been exposed and they most frequently arise from breast or gastrointestinal tract (namely, colon or stomach). Histological characteristics consistent with an endometrial metastasis are absence of premalignant lesions, high degree of myometrium infiltration, sparing of benign endometrial areas and the presence of signet ring cells. Although, subsequently some cases of signet ring cells in endometrial malignancy were found with no other primary tumours detected. The first case of endometrial primary adenocarcinoma was reported by Mooney et al in 1997. (2 Primary endometrial adenocarcinoma with signet ring cells is, in fact, a rare entity.
We believe our case is in line with the diagnosis of a primary endometrial endometrioid adenocarcinoma with mucin-containing signet ring cells and this hypothesis is based on the following facts: first, additional imaging and endoscopic studies did not found any other tumour or metastasis; second, classic endometrioid carcinoma coexists with signet ring cells pattern; third, immunohistochemical pattern was similar between signet ring cells and endometrioid carcinoma. This diagnose is one of exclusion and when this histological pattern is detected, breast imaging and endoscopic examination of stomach and colon are of paramount importance to rule out these primary, most frequent tumours.

