











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkLeiomyomas are benign monoclonal neoplasm that originate from the smooth muscle cells and fibroblasts of the myometrium. They represent the most common benign tumors in premenopausal women. (1 Incidence increases with age during pre-menopausal years, with a lifetime risk > 80% in black women.2 Development and growth of fibroids is estrogen and progesterone dependent. Aromatase in fibroids tissue leads to the endogenous production of estradiol and overexpression of hormonal receptors that facilitate the expanding of these tumors.1 Therefore, situations inducing prolonged exposure to high levels of estrogens and/or progesterone, such as obesity, polycystic ovarian syndrome, early menarche, or late pregnancy increase the risk of uterine fibroids.2,3 The rate of growth varies widely, even for a single individual. (4
Most commonly, patients present with abnormal uterine bleeding. Other symptoms include abdominal distention, pelvic pain or symptoms related with pressure on adjacent organs, like bowel dysfunction or urinary symptoms. Symptoms are related to the size, location, and number of tumors. (1 Based on the International Federation of Gynecology and Obstetrics, leiomyomas may be classified in eight subtypes: 0-2, submucosal; 3-4, intersticial; 5-7, subserosal; and 8, extrauterine. (4
Pathological evaluation is necessary to distinguish between benign and malignant forms. Risk factors for malignant forms include increasing age, radiation of the pelvis and use of tamoxifen. (1 Assessment of tumor vascularization by dUS or MRI is useful for preoperative differential diagnosis. (3
Treatment options should be individualized, considering not only the size and location of the fibroid, but also patient’s age, pregnancy desire, symptoms, and medical experience. (1
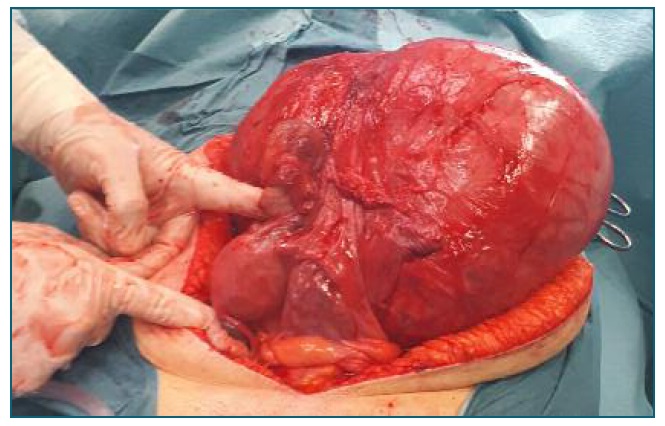
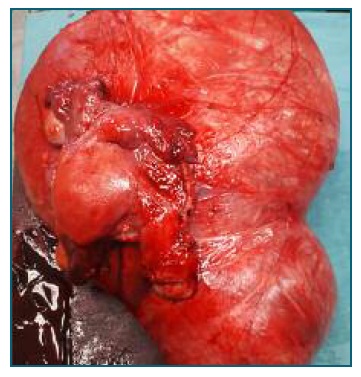
The authors present a case illustrating a huge subserous leiomyoma originating from the uterine cervix. The patient was a caucasian, 50 years-old, premenopausal, with no gynecological surveillance for the past 6 years. She presented with abdominal distention, pelvic pain, and dysmenorrhea for the past year. Clinical evaluation revealed a mass that occupied the entire pelvic cavity and extended into the abdominal cavity. MRI showed normal vascularization, suggesting a benign etiology. Due to the fibroid size and patient desire, an abdominal hysterectomy with bilateral adnexectomy was performed. Histopathological analysis revealed a benign leiomyoma with 16 cm and 855g of weight.
Cervical myomas are extremely rare, with a reported incidence <1%5. Hysterectomy remains the first line treatment in postmenopausal women as it eliminates the risk of recurrence. Management of premenopausal patients is more challenging if there is a desire for fertility preservation. Laparotomic/laparoscopic myomectomy and radical trachelectomy5 have been described to treat giant cervical myomas and may be an option for younger patients.
Patient informed consent was obtained for publication.

