











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Approximately 80% of the breast tumors are benign1. Tubular adenomas are rare proliferative benign breast lesions (0.3-1.7% of all benign breast tumors2) and, only a few cases have been reported in the literature. They are more common among young women (15-49 years old3) and typically affect the upper outer quadrant of the breast3. Histologically, in contrast to fibroadenomas, which are the most common benign mass of young women, tubular adenomas have sparse stromal components.
Preoperatively, tubular adenomas can be difficult to differentiate from fibroadenoma, phyllodes, and tubular carcinoma, even by clinical and radiologic examinations. Histopathology examination is necessary to achieve the correct diagnosis. In addition, surgical excision is usually recommended also for symptomatic relief and avoidance of continuing growth.
We report a case of a 15-year-old girl with a palpable breast mass. Clinical presentation and management are discussed. The patient and her legal tutor have given written consent.
Case-report
A 15-year-old girl has presented with a painless lump in the right breast identified approximately two weeks before. She denied nipple discharge or cyclical mastalgia. Her menstrual cycles were irregular, and she had never used hormonal contraception. She reported hypothyroidism medicated with levothyroxine. No family history of breast disease was known.
On physical examination, there was a nontender, painless, nodular lump in the transition of the inferior quadrants of the right breast. This mass was firm in consistency and mobile. The skin overlying the lump was normal. There were no other palpable masses on the left or right breast and no palpable axillary or supraclavicular lymph nodes. The breast ultrasound (Figure 1) showed a lobulated mass in the right breast with irregular borders, with both echogenic and anechoic components, showing posterior enhancement due to the cystic component. The lump measured 43x16.5 mm. Left breast evaluation was normal. Due to progressive growth and non-conclusive radiologic characteristics of the mass, she gave consent to undergo a lumpectomy of the right breast. The intervention and postoperative recovery were uneventful.
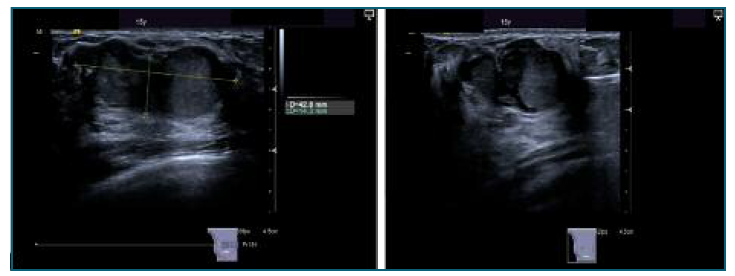
Figure 1 Ultrasound images of breast tubular adenoma, described as a mass with irregular borders, both echogenic and anechoic components, showing posterior acoustic enhancement.
Pathological features: one encapsulated fibro-fatty mass measuring 4.9x3.6x2 cm, with lobulated and irregular borders and rubbery consistency was excised. On pathologic evaluation, it showed grayish white solid areas and the histopathology diagnosis was a tubular adenoma.
Discussion
Breast tubular adenomas, also known as pure adenomas, are rare benign tumors. It is interesting to note that there are few reported cases in the literature, with extremely rare cases reported in juvenile women3,4 and a few cases reported after the age of 405.
Clinically and radiologically, tubular adenomas are almost impossible to differentiate from other benign breast masses, namely, fibroadenomas. Both these benign breast masses are similar even in their age-related incidence.
Performing a biopsy or lumpectomy is essential to provide sufficient tissue to allow a correct histopathology diagnosis, as demonstrated by Sengupta et al6, where only 2.38% preoperative biopsies were diagnosed as tubular adenoma. In our case, an ultrasound-guided breast biopsy was performed preoperatively and the diagnose was a fibroadenoma.
On physical examination, tubular adenomas usually present as a palpable, well circumscribed nodule, mobile, with size varying from 1 to 7.5 cm5, non-tender and more frequently located in the outer and upper quadrants of the breast. Usually, they are not associated with any skin or nipple alterations5. It can be painful in 25% of the cases7.
Imaging, namely ultrasound, usually depicts a well-circumscribed and unencapsulated lesion6, unless they are less than 1 cm, in which case they can be encapsulated, as reported by Tavassoli, et al2. Tubular breast adenomas usually have no calcifications. Despite suspicious radiologic patterns being rarely reported in the literature2,8, they can be found especially in older women. In our case, the first ultrasound performed was considered suspicious (BIRADS 4a- Breast Imaging-Reporting and Data System), because of irregular borders, with both echogenic and anechoic components, showing posterior enhancement due to the cystic component. Macroscopically, they appear as well circumscribed nodules, homogeneous, whitish to tan colored and firm in consistency, although they tend to be softer than fibroadenoma8. Microscopically, breast tubular adenomas are characterized by a homogeneously packed tubular or acinar epithelial component, surrounded by sparse connective tissue, whereas fibroadenomas present with abundant stromal components2.
Tubular adenoma development is not related to oral contraception6. It is a completely benign tumor and has not been associated with an increased risk of breast cancer development9. However, there have been case reports of a synchronous tubular adenoma with breast carcinoma10.
This case is being reported because of the rarity of tubular adenoma of the breast in this age and with the dimensions of this mass. To our knowledge, there is only one case reported4 of a tubular adenoma diagnosed in an adolescent as young as our patient.
Breast tubular adenoma is a rare benign breast condition, mostly diagnosed in young women of reproductive age, but rarely as young as in our case. Clinical and imaging signs are non-pathognomonic making the diagnosis defiant and requiring excisional surgery to confirm it.

