











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Appendicular mucocele is a rare condition referring to a mucus filled, distended appendix, encountered in 0.2 to 0.3 percent of appendectomies. Pathogenesis is dependent on its etiology, that can range from benign to malignant findings.
We report a clinical case of a pregnant woman who underwent a caesarean section due to suspicion of cephalopelvic disproportion (CPD), one of the causes of abnormal labour progression. During surgery, it was detected diffuse intra-abdominal mucin originating from a ruptured appendicular mucocele. Appendectomy was performed and histopathological examination revealed a low-grade appendiceal mucinous neoplasm (LAMN) with peritoneal involvement.
Case report
A 28-year-old healthy woman, gravida 2, para 0 (2G 0P), with an uneventful pregnancy, was admitted for labour induction at 41 weeks’ gestation. Misoprostol was used for cervical ripening, and six hours after, oxytocin was initiated at 15 millilitres per hour. Amniotomy performed four hours after oxytocin initiation revealed clear amniotic fluid. Labour progression was normal until nine centimetres of dilatation, at which point an occiput posterior fetal position was detected. After four hours without any further progression despite corrective measures, a caesarean section was performed due to suspected CPD.
We performed a Pfannenstiel incision and opened the abdominal wall in layers. Copious amounts of yellow-tinged mucoid material were found in the peritoneal cavity. A male neonate (2755 grams) was delivered via Kiwi® vacuum-assisted extraction device due to significant insinuation on the maternal pelvis, with Apgar scores of 9, 10, and 10 at 1, 5, and 10 minutes, respectively. A meticulous pelvic inspection was performed, revealing a vesicular and friable pattern of uterine, annexal and small intestinal serosa and a ruptured tumoral mass at the appendix apex, suggesting a ruptured mucocele of the appendix. Appendectomy with invagination of colon wall was performed in collaboration with general surgeons. The specimen and mucin was sent to histopathological examination. Umbilical cord blood gas analysis was performed and was normal (Table I).
Histopathological examination of the specimen revealed an irregular, mucus-filled appendix (Figure 1). It had a serrated muco-secretory epithelium without atypia and a mucosa with multifocal ulceration and inflammatory reaction (Figure 2). Margins of surgical top of the specimen were clear. The examination of mucoid material revealed scattered muco-secretory epi-thelium cells (Figure 3). These histopathological findings suggested a LAMN, pT4a Nx M1b R0 (AJCC 8th Edition/UICC 2017)6, with peritoneal involvement, due to perforation and extravasation of mucinous content.
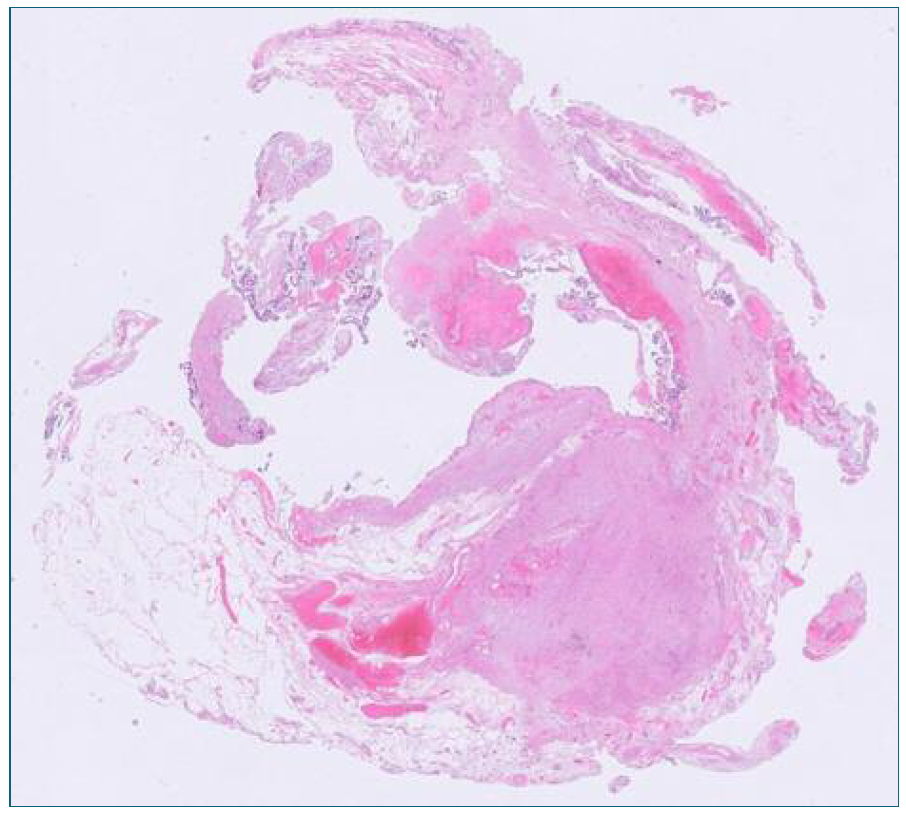
Figure 2 Low grade epithelial features in the absence of infiltrative growth (hematoxylin and eosin stain, 20x).
The patient and her baby had an unremarkable postoperative course and were discharged home on the fourth post-caesarean day.
The woman was referenced for a General Surgery consultation at our hospital. A postoperative thoraco-abdominopelvic computed tomography (CT) scan revealed no locoregional or distant disease. She was subsequently transferred to the Peritoneal Disease Group of the Portuguese National Oncology Center and was considered to cytoreductive surgery (CRS) and heated intraperitoneal chemotherapy (HIPEC). The patient declined fertility preservation, stating no desire for future pregnancies.
At the time of this report, after six months of follow-up, the woman is asymptomatic.
Discussion
Appendicular mucocele is a mucus-filled, distended appendix, encountered in approximately 0.2 to 0.3 percent of appendectomies, with a higher prevalence among females in their 50s and 60s. This condition can be either benign, including simple mucoceles or retention cysts, or malignant, encompassing serrated polyps, mucinous appendiceal neoplasms, and mucinous adenocarcinomas of the appendix.
Appendiceal mucinous neoplasms are characterized by low-grade, non-invasive epithelial proliferation, which, if the appendix ruptures, can lead to pseudomyxoma peritonei (PMP). A rarer and more aggressive variant, high-grade appendiceal mucinous neoplasm (HAMN), demonstrates high-grade dysplasia.
The clinical manifestations of LAMN are typically nonspecific and may include abdominal pain, particularly in the right lower quadrant, a palpable mass, gastrointestinal symptoms such as nausea, vomiting, and bleeding, as well as signs of intestinal intussusception5. However, most cases are discovered incidentally during diagnostic or therapeutic procedures. In pregnant women, uterine contractions can obscure clinical symptoms, further complicating diagnosis.
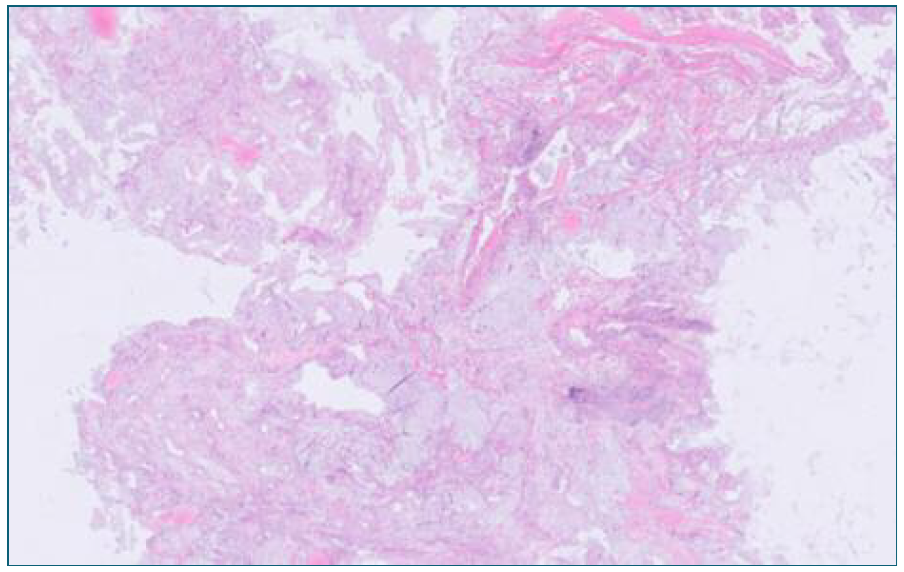
To date, only five cases of LAMN detected during cesarean section have been reported in the literature1-4,11. Bowles et al. documented a case in which a 10.2 × 3.6 × 5.2 centimetres cystic structure in the right iliac fossa was incidentally diagnosed via first-trimester ultrasound11. Other reported cases involved asymptomatic women diagnosed intraoperatively1-4. Additionally, Yohannes et al. and Baron et al. described two cases in which LAMN was identified during cesarean section due to abnormal labor progression2-3.
LAMN is characterized by the production of abundant mucin and an expansile growth confined to the muscularis propria. Appendectomy is typically sufficient when the lesion is localized. Both Inubashiri et al. and Ribeiro et al. reported cases of LAMN confined to the muscularis propria without mucosal fluid leakage, successfully treated with appendectomy, followed by five years of surveillance using CT, ultrasound, and tumor marker assessments1,4.
However, LAMN growth can thin the appendiceal wall, increasing the risk of rupture and subsequent mucin spillage, leading to PMP. The mucin can induce fibrosis and obstruction, resulting in complications such as intussusception, volvulus, small bowel obstruction, and ureteral obstruction2,5. PMP is associated with a high recurrence rate (33 to 78 percent) and significant morbidity7-10. Despite previous concerns, right hemicolectomy does not appear to confer additional benefit over appendectomy alone7. Patients with PMP should be referred to specialized centers for peritoneal surface malignancy management, where CRS and HIPEC may be considered. Fertility preservation should also be discussed in affected individuals.
Histopathological examination in our case revealed LAMN with pT4a Nx M1b R0 staging, indicating cellular mucin involvement of the appendiceal serosa (pT4a), mucin deposits confined to the peritoneum (M1b), and clear surgical margins (R0) 6. Postoperative imaging detected no locoregional or distant disease, and CRS/HIPEC was proposed due to peritoneal involvement.
Only one case of LAMN with PMP has been reported in the literature. Baron et al. documented a case where abundant mucin was observed adherent to pelvic organs during cesarean section, originating from the appendix tip. This patient underwent oocyte retrieval for cryopreservation before CRS/HIPEC and successfully conceived a second child using a frozen embryo three years post-treatment3. Conversely, Bowles et al. reported a case in which histopathological examination revealed extracellular mucin with inflammatory cells but no evidence of malignancy, leading to a decision for right hemicolectomy, which subsequently confirmed the absence of malignant or free mucin11.
The overall three-year and five-year survival rates for LAMN with extra-appendiceal disease range from 91 to 100 percent and 79 to 86 percent, respectively. Patients require long-term follow-up, including routine imaging (abdominopelvic CT, magnetic resonance imaging, and/or ultrasound) and tumor marker evaluations (carcinoembryonic antigen [CEA] and carbohydrate antigens CA 125 and CA 19.9).
In conclusion, LAMN is a rare clinical entity, often detected incidentally. Even when associated with symptoms or identified as a cystic structure on imaging, suspicion remains low due to the higher prevalence of appendicitis and adnexal pathology. Early and accurate diagnosis is crucial for appropriate management. Thorough examination of abdominal and pelvic viscera during cesarean section should be a standard practice when abnormal findings are encountered, as timely identification of tumors such as LAMN can significantly impact patient outcomes.
Authors’ contributions
Joana Torres Silva: Conception, design, writing, reviewing and final editing of the article. Mariana Leal, Carla Duarte, Ana Maçães: Critical review of article content and final approval of the version to be published. Filomena Barreto: Provision and description of the images from the histopathological study.

