










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.12 no.1 Lisboa mar. 2016
https://doi.org/10.1016/j.ancv.2015.10.001
CASE REPORT
Leiomyosarcoma of level II inferior vena cava- an original solution for bilateral renal vein reconstruction
Leiomiossarcoma do nível II da Veia Cava Inferior - uma solução original para a reconstrução das veias renais
Emanuel Silvaa,*, Luís Mendes Pedro a,c,d, Mariana Moutinhoa, Pedro Amorima, Ana Evangelista a,c,d, Santiago Ortizb, Dolores Lópezb, José Fernandes e Fernandes a,c,d
a Clínica Universitária de Cirurgia Vascular, Hospital de Santa Maria CHLN, Portugal
b Serviço de Anatomia Patológica, Hospital de Santa Maria, CHLN, Portugal
c Faculdade de Medicina da Universidade de Lisboa, Portugal
d Centro Académico de Medicina de Lisboa, Portugal
ABSTRACT
Introduction: The leiomyosarcoma of the inferior vena cava (IVC) is a rare clinical entity, although it represents the most common malignant tumor of the venous system. Level II IVC tumors (supra-renal) are the most frequent and those who have a better prognosis for the development of symptoms earlier.
Case report: The authors report a case of IVC leiomyosarcoma in a 59-year old woman, pre-senting with DVT of the right lower limb, subsequent to prolongued nonspecific abdominal pain. Computed tomography revealed a large retroperitoneal neoformation, centered to IVC, which extended above the renal veins (the left one patent and the right one involved in the mass).
The patient underwent en block resection of the tumor and reconstruction of the renal veins: construction of a new IVC bifurcation at the supra-renal level with a bifurcated PTFE graft, followed by graft extension to both renal veins using externally-supported 8 mm PTFE grafts. Histology revealed a high-grade leiomyosarcoma. The postoperative period was complicated by a type 2 MI and retroperitoneal hematoma, with occlusion of the right graft branch and partial infarction of the right kidney. The patient underwent surgery again and proceeded to partial resection of the thrombosed graft branch. The patient was discharged home under anticoagulation and is clinically well without edema of the lower limbs, normal renal function, and has begun adjunctive therapy.
Conclusion: The prognosis of these tumors is poor, with a high recurrence rate. An aggressive surgical approach combined with adjuvant therapy may not be curative, but is the best strategy to prolong survival.
Keywords: Inferior vena cava; Level II; Leiomyosarcoma; En block ressection; Vascular reconstruction; Adjuvant therapy
RESUMO
Introdução: O leiomiossarcoma da veia cava inferior (VCI) é uma entidade clinica rara, embora represente o tumor maligno mais comum do sistema venoso. Os tumores do segmento II da VCI (supra-renal) são os mais frequentes e aqueles que apresentam melhor prognóstico pelo desenvolvimento de sintomatologia mais precocemente.
Caso clínico: Os autores apresentam um caso de leiomiossarcoma da VCI numa doente de 59 anos, que se manifestou por TVP do membro inferior direito, subsequente a quadro de dor abdominal inespecífico arrastado. A tomografia computorizada revelou volumosa neoformação retroperitoneal, centrada à VCI, que se estendia acima das veias renais (a esquerda permeável e a direita envolvida na massa). A doente foi submetida a ressecção em bloco do tumor e reconstrução das veias renais: construção de neo-bifurcação da VCI com prótese de PTFE bifurcada seguido de reconstrução de ambas as veias renais com próteses aneladas (PTFE-8). A histologia revelou tratar-se de um leiomiossarcoma de alto grau. O pós-operatório foi complicado por EAM tipo 2 e por hematoma retroperitoneal com oclusão do ramo protésico direito e enfarte parcial do rim direito. Foi reintervencionada, tendo-se procedido à ressecção parcial do ramo protésico trombosado. A doente teve alta anticoagulada e encontra-se clinicamente bem, sem edema dos membros inferiores, com função renal normal, e iniciou terapêutiva adjuvante.
Conclusão: O prognóstico destes tumores é reservado, com elevada taxa de recorrência. Uma estratégia cirúrgica agressiva combinada com terapêutica adjuvante pode não ser curativa, mas constitui a melhor estratégia para prolongar a sobrevida.
Palavras-chave : Veia cava inferior; Nível II; Leiomiosarcoma; Resseção em bloco; Reconstrução vascular; Terapêutica adjuvante
Introduction
The IVC leiomyosarcoma is a rare clinical entity, with only 300 cases described in the literature and most of them refer to individual case reports or small series.1-5 Represents the tumor that most often affects the venous system and is associated with a poor prognosis.1,3,4
Most patients are asymptomatic, for it is a slow growth tumor and only manifests symptoms in advanced stages of the disease.4,6- 8 Its incidence is more common in women around the sixth decade of life.1 Abdominal pain is the most common symptom; edema of the lower limbs, back pain, weight loss, fever, palpable abdominal mass and, rarely, Budd-Chiari syndrome can also be part of the clinical presentation spectrum.5,9-11
The treatment of this tumor is still controversial. In this paper, we present a case report of a patient submitted to a complex vascular construction.
Case report
A 59-year-old woman presented to her attending physician with epigastric and lower back right pain, associated with constipation and weight of the lower limbs. The abdominal and renal ultrasound scan was normal. Six months later, she developed pain and asymmetrical edema of the right lower limb, with tenderness of leg muscle mass and positive Homan's sign. She maintained pain in the epigastric and right upper quadrant on deep palpation and no palpable masses were felt. The patient did not have fever, chest pain, gastrointestinal, urinary or respiratory changes, as well as recent weight loss. She was admitted to a local hospital with the diagnosis of iliofemoral deep vein thrombosis of the right lower limb.
Her past medical and surgical history included essential hypertension, past caesarean section and laparoscopic cholecystectomy; no known risk factors for venous thrombosis or relevant family history were present.
The venous Color-flow Duplex Scan revealed thrombus extension to the juxta-renal IVC and a nodular mass was observed at this level. An abdominal and pelvic CT scan was performed, revealing the presence of a solid heterogeneous mass in the topography of the duodenal arch, without clear cleavage plane with the duodenum, the uncinate process of the pancreas and the IVC. The examination was completed by ecoendoscopy, which was suggestive of GIST, and ultrasound-guided biopsy of the lesion, which was inconclusive. The analytic study was negative for both pro-thrombotic factors and tumor markers.
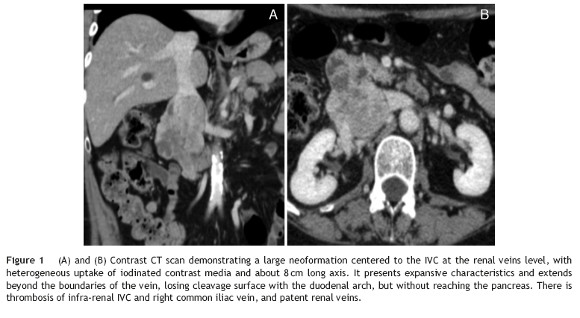
Given the improvement of the right lower limb edema, the anticoagulation therapy was interrupted after 3 months. Then, an abdominal and pelvic Angio-CT scan was requested which allowed a better characterization of a neoplasm centered to the IVC (Fig. 1A and 1B), suggestive of a IVC leiomyosarcoma and no other pathological findings were found.
The patient was then referred for surgery, after a multidisciplinary planning, involving Oncology, General Surgery and Vascular Surgery, and was admitted in the Vascular Surgery Department.
Pre-operatively, a flebogram was performed and showed occlusion of the infrarenal IVC and both common iliac veins.
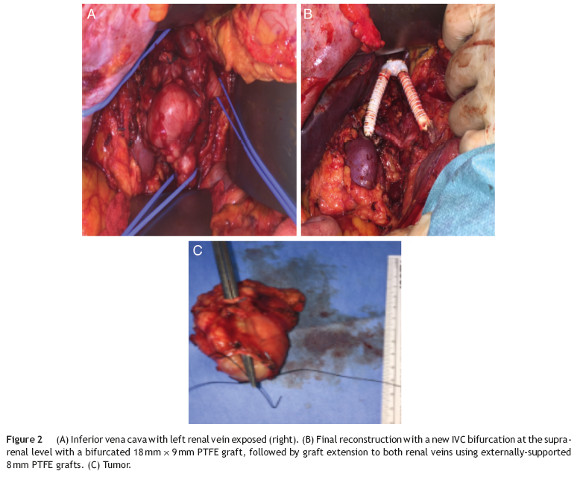
The surgical approach was conducted through a large right subcostal incision. The supra-renal IVC was identified and was free of disease, as well as the left renal vein. The lower segment of the IVC was occluded (fibrotic) and the mass was close to the right renal hilum. After section of the proximal and distal IVC and both renal veins, the en block resection of the tumor was carried on. The technique for renal veins reconstruction included the construction of a new IVC bifurcation at the supra-renal level with a bifurcated 18 mm × 9 mm PTFE graft, followed by graft extension to both renal veins using externally-supported 8 mm PTFE grafts (Fig. 2A - C).
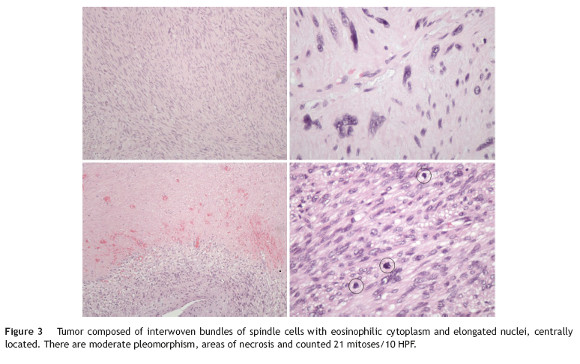
The pathology examination revealed a high-grade leiomyosarcoma, with clear margins (Fig. 3).
The postoperative period was complicated by a type II miocardial infarction (2 day PO) needing to start antiplatelet and anticoagulation therapy. Subsequently, by day 5 PO, the patient complained upper abdominal and back pain associated to an acute anemia of 6.6 g/dl. The emergency CT scan revealed an extensive right retroperitoneal hematoma, thrombosis of the right reno-caval limb graft and partial infarction of the ipsilateral kidney (Fig. 4A and B). The left kidney reconstruction was patent.
The patient was then submitted to laparotomy for hemostasis. As most of the right kidney surface did not appear ischemic, we did not proceed with nephrectomy, and ligation and removal of the right kidney venous graft (thrombosed) was performed.
The patient was discharged by the 20th day PO, under anticoagulation and is clinically well and with resolution of pain and edema of the lower limbs. The renal function is normal. She is now under adjunctive treatment at the Oncology Department.
Discussion
Anatomically, the IVC is divided into three levels, each one associated with different clinical manifestations and surgical considerations. Level I is the infra-renal IVC, level II is the para-renal, supra-renal and infra-hepatic IVC and Level III is the supra-hepatic.6
Level II tumors are the most frequent and those who have a better prognosis for the development of earlier symptoms. Approximately 50% of the cases present with metastasis.1,9
Level I tumors presentation includes back and abdominal pain, edema of lower limbs and, rarely, deep venous thrombosis.12 Lower limb edema occurs more frequently associated with deep vein thrombosis than with occlusion of the IVC by the tumor.4,13,14 In level I neoplasms, patients complains are pain in the right upper abdominal quadrant and, when reaching the renal veins, renovascular hypertension or kidney failure may be found. The Budd-Chiari syndrome is a typical expression of level III tumors, when there is thrombosis of the hepatic veins.12
With regard to diagnosis, contrast CT scan and MRI are the main diagnostic tools. They allow the characterization of the tumor origin, the inferior vena cava involvement and obstruction as well as the collateral circulation. They may demonstrate contiguous invasion, assess the resectability and exclude the existence of extra-abdominal metastases. The definitive histological diagnosis can be obtained by US or CT-guided biopsy.3,8 The use of PET also contributes to evaluate the existence of metastasis and flebography, presently less used, allows to assess the degree of IVC obstruction and its main branches, thus being important for surgical planning.5
Even with all these diagnostic modalities, in many cases it is not possible pre-operatively to determine precisely the origin of these tumors. Moreover, the anatomic location can make it difficult to perform a percutaneous biopsy. Often, the surgeon is faced with the challenge of making an exploratory laparotomy with a tumor of unknown origin and histology.2
The preferred surgical approach, particularly for tumors of level II, is through a subcostal incision, which can be improved by lumbotomy or controlateral extension. Level I tumors can also be approached by median laparotomy, while level III tumors require a thoraco-abdominal approach.
Surgical resection follows the principles of surgical oncology-en block resection with negative margins. Complete resection of the tumor is often difficult because of its location and the involvement of adjacent organs and vascular structures. Thus, 1/3 to half of the patients show locally recurrence or metastization.1,6,15 In general, efforts for venous reconstruction decrease the post-operative morbidity16 and the need and type of reconstruction are influenced by three major factors: (1) the level of IVC affected and the involvement of the renal veins; (2) the extent of the IVC resection (partial or circumferential); (3) the presence of colateral venous flow.8
In level I and II lesions, with chronic occlusion and developed colateral venous flow, IVC ligation without reconstruction is usually well tolerated.15-17 If the occlusion of the IVC occurs acutely, the lower limb edema may be a postoperative issue in 36-70% of the patients and about 1/3 will develop chronic edema or post-thrombotic syndrome.16
In level II tumors, when ligation of the right renal vein is needed, a right nephrectomy is also performed by most authors, even if the kidney is not directly involved, for the absence of adequate colateral venous outflow determining a high probability of ischemia.2 In the case reported we aimed flow with risk of developing renal failure or extreme lower at kidney salvage by bilateral venous reconstruction, as the limb edema.2,6 Kieffer et al. pointed out a cut-off value for tumor did not invade the renal hilum structures. In left sided the proximal pressure in the IVC of 30 mmHg; above this tumors, the left renal vein may be ligated after the emer-level, there is excessive venous pressure justifying recongence of the suprarenal and gonadal veins which are often struction. enough to maintain an adequate venous drainage. In level II tumors, the venous drainage of the kidneys
Techniques for IVC reconstruction include a direct suture is a main issue, especially in cases of poor renal function or patch angioplasty when there is <75% circumference and/or lack of adequate venous drainage of the left kid-involvement of the IVC, that enabling partial resection.14 ney. So, it can be appropriate to carry out bilateral venous Prosthetic reconstruction is more common, and must be reconstruction, whenever possible.7 Various techniques are performed in the absence of adequate collateral venous suggested in the literature including anastomosis of the left renal vein to the inferior mesenteric vein or right kidney auto-transplantation.2,6,7,11
In the present case we report an original technical solution for bilateral venous reconstruction.
Peri-operative mortality and morbidity range between 0-25% and 18-50%, respectively. These values are related to the magnitude of the vascular resection and to the reconstructions performed.4,6 Cardiopulmonary disease, liver and/or kidney failure, lower limb edema, graft occlusion and infection are reported as the major early complications.16 In the series presented by Fiore et al, there is no relationship between graft thrombosis and the type of graft with the subsequent development of renal failure.8 Graft occlusion varies between 7% and 28%4,8 and strategies to prevent thrombosis and improve patency include ringed PTFE grafts, oral anticoagulation and the construction of arteriovenous fistula in the femoral region.2,3
IVC leiomiosarcoma is an aggressive disease and complete surgical resection provides the only chance of cure or palliation of symptoms.16,18 Patients undergoing complete resection had free disease survival rates of 76% and 33% at 3 and 5 years, respectively. When the resection is incomplete, the survival rate is near zero at 3 years.4 In the international registry by Mingoli et al., predictors of increased mortality are level III tumors, Budd-Chiari's syndrome, edema of the lower limbs, intraluminal growth and occlusion of the IVC; level II tumors, the absence of palpable abdominal mass and abdominal pain are associated with better outcome and long-term survival.1
Histologically, leiomyosarcoma is a malignant neoplasm showing pure smooth-muscle differentiation. Macroscopy forms a gray to white to tan mass, with a whorled appearance; the tumor border appears well-circumscribed. The typical histological pattern is that of intersecting, sharply marginated fascicles of spindle cells.19--21 In this case, there are zones with coagulative tumor necrosis. The tumor-cell nuclei are characteristically elongated and blunt-ended; pleomorphisms are notable and mitotic figures are seen. The cytoplasm is eosinophilic to pale. Immunophenotype: smooth-muscle-actin (SMA), desmin and h-caldesmon are positive.
Adjuvant therapy was considered ineffective in the treatment of IVC leiomyosarcomas for many years. Currently, it is accepted that patients undergoing adjuvant chemotherapy and/or radiotherapy have better survival rates,2,7,16 even when local recurrence or distance metastasis are present. So, presently, aggressive surgical approach combined with adjuvant therapy provides the best treatment strategy for patients with IVC leiomyosarcoma.6,7
Close surveillance with regular CT scans searching local recurrence or distance metastasis is indicated. However, there are no defined follow up intervals, which should be requested according to the individual risk. Metastatic disease occurs more frequently in the lung.
Conclusion
The authors report a case of level II IVC leiomyosarcoma submitted to radical en bloc resection associated to an original technique for bilateral venous reconstruction.
Ethical responsibilities
Protection of people and animals. The authors state that for this investigation there has been no experience in humans and/or animals.
Confidentiality of data. The authors state that they followed the protocols of their work center on the publication of patient data.
Right to privacy and consent in writing
The authors declare having received written consent from patients and/or subjects mentioned in the article. The corresponding author must be in possession of this document.
Conflicts of interest
The authors have no conflicts of interest to declare.
References
1. Mingoli A, Cavallaro A, Sapienza P, et al. International registry of inferior vena cava leiomyosarcoma: analysis of a world series on 218 patients. Anticancer Res. 1996;16:3201-6. [ Links ]
2. Kyriazi MA, Stafyla VK, Chatzinikolaou I, et al. Surgical challenges in the treatment of leiomyosarcoma of the inferior vena cava: analysis of two cases and brief review of the literature. Ann Vasc Surg. 2010;24:826.e13-7. [ Links ]
3. Mastoraki A, Leotsakos G, Mastoraki S, et al. Challenging diagnostic and therapeutic modalities for leiomyosarcoma of inferior vena cava. Int J Surg. 2015;13:92-5. [ Links ]
4. Hollenbeck ST, Grobmyer SR, Kent KC, et al. Surgical treatment and outcomes of patients with primary inferior vena cava leiomyosarcoma. Am Coll Surg. 2003;197:575-9. [ Links ]
5. Kim JT, Kwon T, Cho Y, et al. Multidisciplinary treatment and long-term outcomes in six patients with leiomyosarcoma of the inferior vena cava. J Korean Surg Soc. 2012;82:101-9. [ Links ]
6. Kieffer E, Alaoui M, Piette JC, et al. Leiomyo-sarcoma of the inferior vena cava: experience in 22 cases. Ann Surg. 2006;244:289-95. [ Links ]
7. Hines OJ, Nelson S, Quinones-Baldrich WJ, et al. Leiomyosarcoma of the inferior vena cava: prognosis and comparison with leiomyosarcoma of other anatomic sites. Cancer. 1999;85:1077-83. [ Links ]
8. Fiore M, Colombo C, Locati P, et al. Surgical technique, morbidity, and outcome of primary retroperitoneal sarcoma involving inferior vena cava. Ann Surg Oncol. 2012;19:511-8. [ Links ]
9. Ramponi F, Kench J, Simring D, et al. Early diagnosis of an asymptomatic leiomyosarcoma of the inferior vena cava prior to caval obstruction. J Vasc Surg. 2012;55:525-8. [ Links ]
10. Gowda RM, Gowda MR, Mehta NJ, et al. Right atrial extension of primary venous leiomyosarcoma: pulmonary embolism syndrome and Budd-Chiari at presentation and case report. Angiology. 2004;55:213-6. [ Links ]
11. Wang Q, Jiang J, Wang C, et al. Leiomyosarcoma of the inferior vena cava level II Involvement: curative resection and reconstruction of renal veins. World J Surg Oncol. 2012;10:120. [ Links ]
12. Liu C, Zheng Y, Yang X, et al. Surgical resection of inferior vena cava for leiomyosarcoma. Ann Vasc Surg. 2010;24:812e11-22e15. [ Links ]
13. Ito H, Hornick J, Bertagnolli M, et al. Leiomyosarcoma of the inferior vena cava: survival after aggressive management. Ann Surg Oncol. 2007;14:3534-41. [ Links ]
14. Dull B, Smith B, Tefera G, et al. Surgical management of retroperitoneal leiomyosarcoma arising from the inferior vena cava. J Gastrointest Surg. 2013;17:2166-71. [ Links ]
15. Mingoli A, Sapienza P, Cavallaro A, et al. The effect of extent of caval resection in the treatment of inferior vena cava leiomyosarcoma. Anticancer Res. 1997;17:3877-81. [ Links ]
16. Bower T, Nagorney D, Cherry K Jr, et al. Replacement of IVC for malignancy: an update. J Vasc Surg. 2000;31:270-81. [ Links ]
17. Daylami R, Amiri A, Goldsmith B, et al. Inferior vena cava leiomyosarcoma: is reconstruction necessary after resection? J Am Coll Surg. 2010;210:185-90. [ Links ]
18. Spinelli F, Stilo F, La Spada M, et al. Surgical treatment of tumors involving the inferior vena cava. Personal experience. J Cardiovasc Surg. 2008;49:323-8. [ Links ]
19. Fletcher C, Bridge J, Hogendoorn P, et al. WHO classification of tumours of soft tissue and bone. International Agency for Research on Cancer; 2013. [ Links ]
20. Goldblum J, Folpe A, Weiss S. Enzinger and Weiss's soft tissue tumors. 6th ed. Elsevier Saunders; 2014. [ Links ]
21. Hornick J. Practical soft tissue pathology: a diagnostic approach. 1st ed. Elsevier Saunders; 2013. [ Links ]
E-mail address: emanueljsilva@gmail.com (E. Silva).
Received 5 June 2015;
Accepted 5 October 2015
Available online 24 November 2015.

