










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.14 no.2 Lisboa jun. 2018
ARTIGO DE REVISÃO
Endovascular aneurysm repair: current status on device specifications and outcomes
Correção endovascular de aneurismas: status atual nas especificações e resultados das endopróteses
Filipa Cordeiro1, José Oliveira-Pinto1,2,3, Armando Mansilha1,2,3
1Departamento de Cirurgia e Fisiologia, Faculdade de Medicina da Universidade do Porto.
2Departamento de Angiologia e Cirurgia Vascular, Centro Hospitalar de São João.
3Serviço de Angiologia e Cirurgia Vascular, Hospital CUF, Porto.
Autor para correspondência
ABSTRACT
Introduction: Since its first introduction in 1991, endovascular aneurysm repair (EVAR) became the preferred modality for abdominal aortic aneurysms (AAA) repair. Several devices have been launched over the years addressing progressively more complex anatomies. The aim of this review is to provide an update on current endografts and compare their results.
Methods: MEDLINE databases were searched for endografts features and respective outcomes.
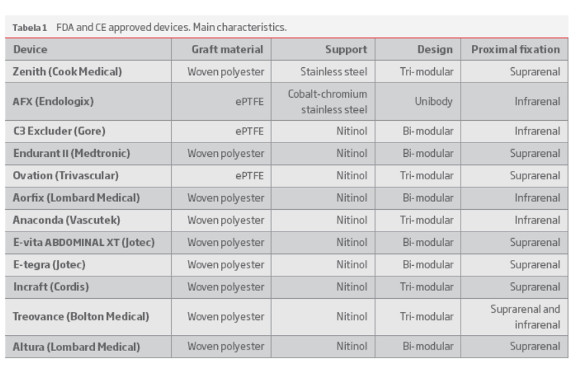
Results: Currently, a significant variety of grafts is approved for clinical use, targeting different anatomic properties. There are presently six CE and FDA approved devices: Zenith®, AFX®, C3 EXCLUDER®, Endurant® II, Ovation® and Aorfix™; while six more have only the CE mark: Anaconda™, E-vita ABDOMINAL XT®, E-tegra®, Incraft®, TREOVANCE® and Altura™.
Also, there are four fenestrated and branched endografts available for treating thoracoabdominal aneurysms: Zenith® Fenestrated, Fenestrated Anaconda™, Zenith® p-Branch® and Zenith® t-Branch®.
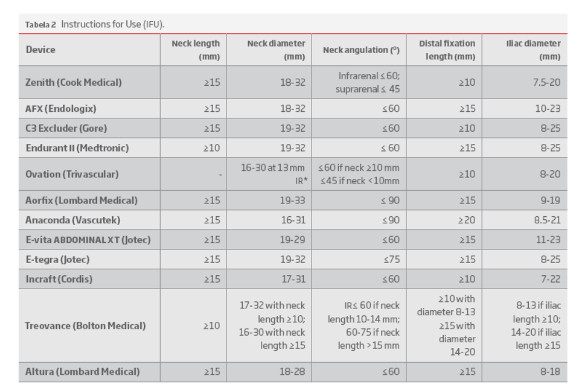
The Endurant II and Treovance stent grafts can accommodate neck lengths ≥10 mm; Aorfix and Anaconda are more liberal regarding neck angulation, extending of infrarenal neck angulation up to 90º. Finally, Zenith, C3 Excluder, Ovation and Incraft stent grafts can be used with distal fixation length ≥10 mm.
Conclusion: New-generation endografts perform better than the older ones, especially in challenging anatomies. Mid-term outcomes between contemporary stent-grafts seem to be similar for most of the outcomes. However, no randomized controlled trials exist comparing different contemporary stent grafts, making conclusions difficult to accomplish. Long-term follow-up reviews are required to assertively take assumptions about different stent grafts performance.
Keywords: Abdominal aortic aneurysm, Endovascular Aneurysm Repair, Endograft
RESUMO
Introdução: Desde a sua introdução, em 1991, o tratamento endovascular (EVAR) tornou-se o método de eleição na correção dos aneurismas da aorta abdominal (AAA). Inúmeros dispositivos foram produzidos, desde então, abrangendo anatomias cada vez mais complexas. O objetivo desta revisão é proporcionar uma atualização nas endopróteses disponíveis e comparar os seus resultados.
Materiais e Métodos: Foi realizada uma pesquisa, nas bases de dados da MEDLINE, sobre características das endopróteses e respetivos resultados.
Resultados: Atualmente, existe uma grande variedade de endopróteses aprovada com propriedades anatómicas distintas. Existem seis próteses com aprovação CE e FDA: Zenith®, AFX®, C3 EXCLUDER®, Endurant® II, Ovation® e Aorfix™; e seis com a aprovação CE: Anaconda™, E-vita ABDOMINAL XT®, E-tegra®, Incraft®, TREOVANCE® e Altura™.
Existem, ainda, quatro próteses fenestradas e ramificadas disponíveis para o tratamento de aneurismas toracoabdominais: Zenith® Fenestrated, Fenestrated Anaconda™, Zenith® p-Branch® and Zenith® t-Branch®.
As endopróteses Endurant II e Treovance acomodam colos aórticos ≥10 mm; Aorfix e Anaconda são mais flexíveis no que respeita à angulação, permitindo que o ângulo aórtico se estenda até 90º. Por fim, as próteses Zenith, C3 Excluder, Ovation e Incraft podem ser usadas em locais de fixação distal com comprimento ≥10 mm.
Conclusão: As próteses de nova geração têm um melhor desempenho que as mais ancestrais, especialmente no que diz respeito a anatomias complicadas. Os resultados a médio prazo entre as próteses contemporâneas assemelham-se para a maioria das variáveis. Contudo, não existem estudos controlados randomizados comparativos entre as diferentes endopróteses, dificultando a obtenção de conclusões. São necessárias revisões de longo prazo para assumir, assertivamente, pressupostos acerca do desempenho das diferentes próteses.
Palavras-chave: Aneurisma da aorta abdominal; Correção endovascular de aneurismas da aorta abdominal; endoprótese
INTRODUCTION
Endovascular aneurysm repair (EVAR) was first introduced in 1991 by Parodi et al.(1) and is currently the preferred method for AAA repair due to its minimal invasive profile.(2)(3)
The landmark randomized clinical trials have emphasized the short-term survival benefits confirmed by large US registries on Medicare beneficiaries.(4)(6)
Still, anatomic restraints remain the Achilles Heel of its full applicability. EVAR results are affected by the different anatomic features and, therefore, they constitute a serious concern both for physicians and for stent graft manufacturers. Several Instructions for Use (IFU) have been designed based on anatomic characteristics, in order to maximize EVAR outcomes.(7)(8)
The need to exclude progressively more complex AAA, translated in stent graft technological evolution, with introduction of innovative devices widening the eligibility to EVAR.(2)
Despite the wide range of endografts available, a detailed overview of stent graft particularities and comparison of results are scarcely described.
This review aims to present an update on the current endografts available for aortic abdominal and thoracoabdominal aneurysms repair.
METHODS
Study design and literature search
A literature search on the MEDLINE databases was performed, to identify studies describing endografts properties and outcomes Studies were included if they met the next criteria: data on human implantations, published since 2010 and in English language.
FDA and CE approved stent grafts
Zenith® (Cook Medical Technologies, Bloomington, IN, USA)
The Zenith graft was firstly introduced in 1993 and FDA approved in 2003. Since then, this device underwent several modifications, and is now able to accommodate aortic neck and iliac artery diameters up to 32 and 20 mm, respectively.
It is a three-piece modular, bifurcated graft made of woven polyester sutured to a stainless-steel stent frame with proximal active fixation with barbs.(2)(9)(10)
The main body is designed to bifurcate right above the aortic bifurcation for added stability. It comes in diameters that vary from 22-36 mm. The main body can be delivered through introducer sheaths measuring from 20-24F. The iliac limb extensions come in a variety of working lengths (37-122 mm), which are introduced through sheaths ranging between 14F and 16F. The major advantage of Zenith is the fact that allows the treatment of a wide range of aortic and iliac arteries diameters.(10)
The Zenith stent graft is indicated for treatment of patients with infrarenal neck ≤60º and suprarenal neck ≤45º. Regarding neck length, Zenith is suitable for necks with ≥ 15mm. This stent graft is indicated in iliac diameters 7.5-20 mm and can be applied when distal fixation length ≥10 mm.
AFX® (Endologix Inc., Irvine, CA, USA)
The AFX graft, available since 2011, is the only unibody endograft that is currently approved in the US. It is made of a cobalt-chromium stainless steel endoskeleton which is sutured only at the proximal and distal ends of the inner surface of the graft material, a low porosity expanded polytetrafluoroethylene (ePTFE), allowing its flexibility.(11)
It is the only graft with anatomical fixation to the aortic bifurcation, offering fixation into both proximal and distal landing zones, in contrast to almost all other grafts that present their main fixation point in the infrarenal neck. As the main body rests on the aortic bifurcation, this graft seems to be protected from migration.(11)(12)
This graft accommodates onto the irregularities of the aortic neck which allows its use for narrow bifurcations (≤ 15mm). Moreover, the AFX has a more durable ePTFE fabric than the Powerlink® system, its predecessor.(9)
The AFX main body is available in different diameters – 22, 25 and 28 mm – and lengths – from 40-120 mm (body) and 30-55 mm (limbs).(11)
The delivery system of this stent graft consists of a 17F hydrophilic introducer sheath with a hemostatic valve and a 9F contralateral percutaneous access and is approved for neck lengths ≥15 mm neck with an infrarenal angulation less than 60º. The AFX stent graft can be used in neck diameters from 18-32 mm. This stent graft can be used in patients with iliac diameters 10-23 mm and with distal fixation length ≥15 mm.
However, its navigation and deployment can be challenging for physicians even those with moderate experience, because of its extreme flexibility. (2)(9)(13)
C3 EXCLUDER® (W.L. Gore & Associates, Inc., USA)
The Excluder endograft was firstly launched in 1997 and it underwent several modifications, until it was replaced by the third generation device with C3 Delivery System.(14)(15)
The C3 Excluder is a modular-bifurcated device with a PTFE-fabric and active infrarenal attachment with barbs. While there were no changes made to the device itself, the C3 system, FDA approved in 2011, provides the ability to reposition the graft prior to final release from the delivery catheter. This way, the device can be adjusted until the ideal location is reached.(2)(14)
This device is currently approved to treat infrarenal aortic neck diameters ranging from 19-32 mm with a minimum aortic neck length of 15 mm and a proximal aortic neck angulation ≤60º. Iliac diameters that are adequate for this endograft range 8-25 mm. Distal fixation length should be ≥10 mm.
The C3 Excluder requires a separate introducer sheath with diameters of 18 or 20F for main body deployment.(3)
This endograft has been used for 20 years now, with proven safety, efficacy and long-term durability. The enhancements made to this device have led it to become the US market leader for EVAR.(16)
Endurant® II (Medtronic Vascular, Inc., Minneapolis, MN, USA)
The Endurant II device, FDA approved in 2012, is the latest generation device that started with the Talent® stent graft.
Before its introduction, about 1/3 of patients with AAA and about 50% of high-risk AAA patients were excluded from EVAR because of anatomic criteria.(17)
It is a modular-bifurcated, composed of nitinol stents and polyester graft, low-profile (23-36 mm main body sizes deployed through 18F access) device with a sheathless hydrophilic delivery system.(2)(13)
The Endurant II provides better resistance to migration in short and angulated proximal aortic necks because of its combination of M-shaped configuration of nitinol stents and enhanced suprarenal active fixation with anchoring pins.(2)
Precise deployment is achieved using the controlled release system which allows separate deployment of the barbed suprarenal fixation stent apart from the main body. Multiple lengths and diameters are available for the iliac limbs with the largest flared limb measuring 28 mm. This stent graft is approved for aortic necks at least 10 mm in length with angulation ≤60º.(13)
This endograft can be used in neck diameters 19-32 mm. In what concerns to iliac diameters, it's indicated when range 8-25 mm. Distal fixation length must be ≥15 mm.
Ovation® (Trivascular Inc, USA)
The Ovation endograft, FDA approved in 2012, was developed to navigate small, tortuous, or diseased vessels as well as short aortic necks. This device has one of the lowest delivery profile currently approved, 14-15F outer diameter for the main body, and 13-15F for the iliac limbs, providing treatment for patients that present a wide range of iliac access.(9)(18)
This device is a bifurcated tri-modular device consisting of an aortic body comprised of ePTFE material, iliac limbs and iliac extensions as required.
IFU for Ovation stent graft include proximal neck angulation <60º, proximal aortic neck length <7 mm, aortic neck diameter 16-30 mm (at 13 mm below the lowest renal artery), distal iliac landing zone <10mm, and/or aortic neck/iliac inner wall diameter inappropriately sized to the stent graft.(13)
Aorfix™ (Lombard Medical, Didcot, UK)
The Lombard Aorfix stent graft is the more recently FDA approved device (2013) and it was designed to accommodate severe neck angulation.
The Aorfix is a modular device made of woven polyester and a continuous electropolished nitinol wire using a ring stent configuration that allows the stent graft to be flexed axially without collapsing or twisting. Its features allow the accommodation of necks with angulation up to 90º, which lies outside the IFU for other devices.(9)(19)
The bifurcated endograft has body diameters ranging from 24-31 mm combined with iliac limbs that can vary from 10-20 mm in diameter. The body length ranges from 81- 142 mm. Aortic segments of bifurcated grafts with attached ipsilateral leg prostheses are commonly delivered through a 22F sheath, while the contralateral leg is delivered via a 14F sheath. The delivery system provides fine adjustment and precise positioning even inside tortuous anatomy.(19)
This endograft is indicated to treat aneurysms with neck lengths ≥15 mm, neck diameters ranging from 19 to 33 mm and neck angles ≤90º. Also, it should be applied when iliac diameters 9-19 mm and distal fixation length ≥15 mm.
CE approved stent grafts
Anaconda™ (Vascutek, Terumo, Inchinnan, Scotland, UK)
The Anaconda stent graft system, CE marked in 2005, is a tri-modular device with woven polyester fabric and nitinol skeleton. Since its first introduction, this device suffered alterations that allowed the decrease of migration risk.(20)
The main body comes in different proximal diameters that range from 21.5 to 34 mm. On the other hand, the iliac limbs proximal diameters vary from 10 to 23 mm.
The delivery system of the main body has an outer diameter of 20.4 or 22.5F and consists of a flexible thermoplastic fluoropolymer hydrophilic-coated sheath with a repositionable deployment system that enables relocation for optimal positioning; the delivery system for the iliac limbs has an outer diameter of 18.3F.(13)
The Anaconda stent graft is indicated to treat infrarenal neck angulations up to 90º, with proven results within challenging anatomy.(21)
Anaconda is indicated to treat patients with neck length ≥15 mm and neck diameters ranging 16-31 mm. Iliac diameters range between 8.5mm and 21mm, while appropriated distal fixation length is ≥20 mm.
E-vita ABDOMINAL XT® (Jotec, Hechingen, Germany)
The E-vita stent graft is a bi-modular device, first approved for the European market in 2008, composed of low porosity woven polyester fabric and nitinol stents, with suprarenal fixation.
The bifurcated main body is available in 150 and 170 mm ipsilateral lengths and in body lengths of 80 and 100 mm to the end of the 14 mm-diameter contralateral connection socket. Proximal diameters range from 24 to 34 mm and iliac diameters from 12 to 24 mm.
Delivery systems for main bodies and aortic extensions are available in 20 and 22F – for contralateral legs and iliac extensions even in sizes as from 16F. The “Squeeze-to-Release” mechanism allows for gradual or continuous release at minimum effort, providing most precise positioning and handling.
This device is designated to aortic neck length ≥15mm, comprehending diameters range 19-29 mm. It is indicated for neck angles ≤60º. It allows treating patients with distal fixation length ≥15 mm and iliac diameters range 11-23 mm.
E-tegra® (Jotec, Hechingen, Germany)
The E-tegra endograft, CE approved in 2014, is a bi-modular device and consists of a main body and a contralateral leg. The system can be individually adapted once iliac and aortic extensions are available in the market. For selected cases the aorto-uni-iliac device will be indicated.
The main body of this stent graft is available 80 and 100 mm length, while the proximal diameter ranges from 23 to 36 mm. The contralateral leg is available with a proximal diameter of 15 mm, while iliac extension varies from 13 to 27 mm.
It shares the same delivery system, “Squeeze-to-Release”, with E-vita ABDOMINAL XT, which is available in 18 and 20F for the main body, aortic extensions and aorto-uni-iliac components and start at only 16F for contralateral legs and iliac extensions.
The main differences between this endograft and E-vita ABDOMINAL XT are the fact that E-tegra is more flexible, allowing neck diameters up to 32mm to be treated. Also, E-tegra is indicated in aortic neck angulation up to 75º.
Incraft® (Cordis, Fremont, CA, USA)
The Incraft stent graft, available since 2014, is a next-generation, ultra-low profile, bifurcated graft that was designed to overcome the limitation of smaller and more diseased access vessels.
It is a tri-modular device constructed of a seamless, low porosity, woven polyester graft maintained by a series of self-expanding nitinol stents throughout the whole graft.(2)
The main body comes in 26 and 30 mm diameters, while iliac graft limbs are available in diameters that range from 13-20 mm.(22)
The most remarkable features of this stent graft are: low profile – with a delivery system for the main body with an outer diameter of 14F, which enables delivering through narrow iliac vessels – and extremely bendable delivery system; “in situ length adjustment” of the limb prostheses for optimal distal landing; suture knots on the outer surface of the limb prostheses comprise an interlocking mechanism between the components, that removes the risk of limb separation.(23)
The Incraft endograft is indicated in neck length ≥15 mm, neck diameters 17-31 mm, neck angulation ≤60º. Iliac diameter can range from 7-22 mm.
TREOVANCE® (Bolton Medical, Inc., Barcelona, Spain)
The Treovance stent graft, CE approved since 2015, it's a tri-modular system that consists of a main bifurcated body and two leg extensions. It is made of self-expanding nitinol stents sutured to woven polyester fabric. Unlike other endografts that have suprarenal or infrarenal fixation, multiple proximal fixation points are provided by suprarenal and infrarenal barbs extending from the suprarenal stent. The double level of proximal barbs contributes to minimize the risk of migration even in tortuous anatomies.(24)
The main body of this endograft comes in different diameters (20-36 mm) while each leg is always the same diameter (14 mm), regardless of the proximal diameter size.
The delivery system is low-profile, flexible and hydrophilic with detachable sheaths. Sheath sizes for the main body ranges from 18 (for main bodies up to 28 mm) to 19F (for larger diameters) and iliac limb system ranges from 13 to 14F.(13)
This device has quite specific IFU, allowing treatment of neck lengths ≥10 mm; neck diameters 17-32mm if neck length ≥10 mm, and 16-30 mm if neck length >15mm; iliac diameter 8-13, if iliac length ≥10 mm and 14-20 mm if iliac length ≥15 mm.
Altura™ (Lombard Medical, Didcot, UK)
The Altura stent graft is the most recent CE marked endograft (2015). It consists of a braided nitinol frame, a fabric woven polyester sleeve with a flexible modular system. Its fixation is suprarenal. The evolutionary step was to split the main infrarenal body into two sections, which has the potential to simplify EVAR.
The top and bottom stents are placed first, and if the stent overlap is too small, a simple universal bridging piece is placed to bridge the central portion.
One of the features that makes this device unique is that there's no need for contralateral limb cannulation, as both iliac limbs are simply inserted over the preexisting stiff wires. The delivery system has an ultra-low profile with an outer diameter of 14F.
This endograft is available in diameters that range between 24-30 mm, whereas the suprarenal stent diameter ranges from 29-36 mm. The leg has a 13 mm universal diameter. The iliac limbs diameters vary from 13-21 mm.
Altura stent graft is indicated if neck length ≥15 mm, neck diameters from 18-28 mm, neck angulation ≤60º and iliac diameter 8-18mm.
Fenestrated and Branched Stent Grafts
Up to 40% of patients are unsuitable for traditional EVAR. In patients with a juxtarenal or thoracoabdominal aneurysm there is no proximal or distal zone for anchorage. To overcome these limitations, fenestrated and branched stent grafts were developed.(25)(28)
Fenestrated grafts were developed with holes in the device, which are positioned adjacent to the aortic branch artery orifices. Distinctively, branched stent grafts incorporate pre-attached limbs or cuffs targeted for visceral aortic branches.(29)
Zenith® Fenestrated AAA Endovascular Graft (Cook Medical Technologies, Bloomington, IN, USA)
The only fenestrated stent graft currently FDA approved is the Zenith fenestrated endovascular stent graft. (26)
This device is a modular system with three components: a proximal body graft, a distal bifurcated body graft and one iliac leg. These are made of full-thickness woven polyester fabric sewn to self-expanding stainless steel Cook-Z® stents with braided polyester and monofilament polypropylene suture. Ancillary devices such as main body extensions, iliac leg extensions, converters and iliac plugs may also be required. The delivery system uses a 20 or 22F H&L-B One-Shot Introduction System.
The Zenith Fenestrated is indicated to treat patients with abdominal aortic or aorto-iliac aneurysms having morphology suitable for endovascular repair, including non-aneurysmal infrarenal aortic segment proximal to the aneurysm with a length ≥4mm and unsuitable for a non-fenestrated graft; a diameter ≥19mm and ≤31mm and angulation <45º. Ipsilateral iliac artery distal fixation must be >30mm in length and 9-21mm in diameter, while contralateral iliac artery distal fixation site >30mm in length and 7-21mm in diameter is required.
Fenestrated Anaconda™ (Vascutek, Terumo, Inchinnan, Scotland, UK)
The Fenestrated Anaconda stent graft is not FDA-approved; however it is commercially available in Europe. The system consists of an aortic endograft and two separate iliac limbs. The proximal end of the main body consists of two separate nitinol ring stents and four pairs of nitinol hooks that aid in sealing. The main body itself does not contain any stents, allowing for flexibility in fenestration placement. After deployment, the device can be fully repositioned. It also offers a magnetically assisted limb cannulation system that can decrease contralateral cannulation time. This stent graft is custom made for each patient. (28)(30)(32)
Zenith® p-Branch® Endovascular Graft (Cook Medical Technologies, Bloomington, IN, USA)
The Zenith pivot branch (p-branch) endograft is a tubular, fenestrated device designed to work as a single implant when the distal landing site within a prior aortic repair is ≤22 mm or as the proximal component of a modular bifurcated system that may be combined with other Zenith devices. It is made of polyethylene terephthalate fabric with a proximal stainless steel uncovered barbed supraceliac stent, followed by a series of nitinol Z-stents that incorporate a scallop for the celiac artery, a fenestration for the superior mesenteric artery and two renal pivot fenestrations. The renal fenestrations are precannulated, making it easier to catheterize the target vessels.(33)(34) The delivery system consists of a 20 F system.
The Zenith p-branch is indicated to treat patients with a non-aneurysmal aortic segment proximal to the aneurysm with ≥4 mm of length, a 21-31mm diameter, an angle <60º relative to the centerline of the aneurysm and an angle <45º relative to the supraceliac aorta. Also, renal vessel origins as measured relative to the superior mesenteric artery compatible with the renal fenestration and celiac vessel origin compatible with the celiac scallop.(35)
Zenith® t-Branch® Thoracoabdominal Endovascular Graft (Cook Medical Technologies, Bloomington, IN, USA)
The Zenith t-Branch thoracoabdominal endovascular graft is designed to be used in combination with other Zenith thoracic endovascular grafts, Zenith distal endovascular grafts and iliac leg grafts.
It consists of a tubular graft with four branches and with a covered stent at the proximal end that contains barbs for additional fixation of the device. The purpose of the branches is to allow uninterrupted blood flow to visceral vessels of the aorta. This device is designed to be connected with the celiac, superior mesenteric and two renal arteries via self-expanding covered vascular bridging stents.
It is made of woven polyester sewn to self-expanding stainless steel Cook-Z® stents with braided polyester and monofilament polypropylene suture.
The delivery system uses a 22F H&L-B One-Shot Introduction System.
The Zenith t-Branch is indicated for the endovascular treatment of high-risk patients with thoracoabdominal aneurysms who are not amenable to open surgical repair. The patient must have a non-aneurysmal thoracic aorta fixation segment proximal to the aneurysm with an angle <90º, with a length ≥25mm and a diameter ≥24mm and ≤30mm.
Alternatively, this endograft can be attached to a preexisting endovascular graft.
Also, celiac and superior mesenteric arteries must be 6-10mm in diameter, renal arteries 4-8mm, the distance between each cuff and the corresponding arterial orifice <50mm and the line between the cuff and the arterial orifice as projected onto the vessel wall deviates by no more than 45º from the long axis of the aorta.
DISCUSSION
EVAR represents the most common modality for AAA repair. However, a significant stent graft evolution has occurred over the last years.
The first generation endografts were devices with very high complication rates, particularly stent migration and limb occlusion.(3)
Since then, the manufacturers made an effort to correct major drawbacks: Stent migration and limb occlusion rates have been drastically reduced, which allowed a great increase in their durability, leading to lower rates of morbimortality. The most iconic examples are the evolution of Talent stent graft to Endurant and also the advancement made with the Excluder.(3)(36-40)
Based on available literature, endografts have overlapping results in what concerns major adverse events. ( Table 3)
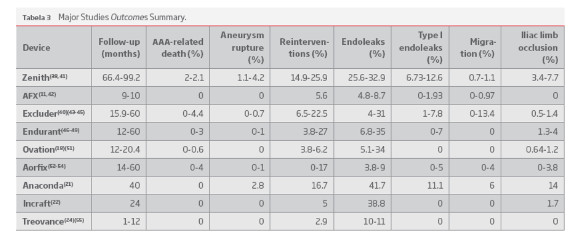
The Zenith endograft, in a mean follow-up period of 66.4-99.2 months, presented 2-2.1% of AAA-related death, 1.1-4.2% of aneurysm rupture, 14.9-25.9% of secondary intervention, 6.73-12.6% of type I endoleaks, 0.7-1.1% of stent migration (≥10 mm) and 3.4-7.7% of limb occlusion.(38)(41)
The AFX stent graft, in a mean follow-up period of 9-10 months, showed the following outcomes: null rates of AAA-related deaths, aneurysm rupture or limb occlusion; 5.6% of secondary intervention, 0-1.93% of type I endoleak and, finally, stent migration (≥10 mm) range 0-0.97%.(11)(42)
The Excluder stent graft, in a mean follow-up period of 15.9-60 months, presented 0-4.4% of AAA-related deaths, 0-0.7% of aneurysm rupture, 6.5-22.5% of secondary interventions, 1-7.8% of type I endoleaks, 0-13.4% of stent migration (≥10 mm) and 0.5-1.4% of limb occlusion.(40)(43-45)
The Endurant device, in a mean follow-up period of 12-60 months, it were reported 0-3% of AAA-related death, 0-1% of aneurysm rupture, 3.8-27% of secondary intervention, 0-7% of type I endoleaks, null rates of stent migration (≥10 mm) in all four studies and 1.3-4% of limb occlusion.(46-49)
The Endurant device was also studied in challenging anatomies. Inclusion criteria were short proximal aortic necks (≤15 mm) and/or small (<8mm), calcified and severely angulated/ tortuous (Iliac tortuosity index [ITI] ≥ 1.4) iliac access vessels. In a mean follow-up period of 15 months 2% aneurysm-related death was registered with 4% of patients presenting with had contained aneurysm ruptures. Reintervention was needed in 8% of patients. There was a 6% rate of type I endoleak as well as a 6% rate of type II endoleak. Graft limb occlusion was noticed in 4% of patients.(50)
Five-year data from the ENGAGE registry, which included follow-up imaging from approximately 500 of the 1262 initial patients, was presented at the 39th Charing Cross Symposium, in 2017. It was stated a 97.8% freedom from AAA-related death, 84.3% freedom from secondary procedures and 89.4% stable or decrease in AAA sac diameter.
The Ovation endograft, in a mean follow-up period of 12-20.4 months, presented 0-0.6% of AAA-related deaths, null aneurysm rupture and stent migration (≥ 10mm) rates, 3.8-6.2% of secondary intervention, 5.1-34% of endoleaks, all type II, and limb occlusion ranging 0.64-1.2%.(18)(51)
As it goes for the Aorfix endograft, in a mean follow-up period of 14-60 months, aneurysm-related deaths ranges from 0 to 4%, while presenting 0-1% of aneurysm rupture, 0-17% of reintervention, 0-5% of type I endoleak, 0-4% of stent migration (≥10 mm) and, finally, 0-3.8% of limb occlusion.(52-54)
In a 40-month study, with the use of Anaconda stent graft it was obtained 0% of AAA-related death, 2.8% of aneurysm rupture, 16.7% of secondary intervention, 41.7% of endoleak, including 11.1% type I endoleak, 6% of stent migration and 14% of limb occlusion.(21)
In what concerns to the Incraft device, in a 24-month follow-up period, null rates of aneurysm-related death, aneurysm rupture and also stent migration were observed. There was a 5% reintervention rate, 38.8% endoleak rate, all type II, and 1.7% limb occlusion rate.(22)
For TREOVANCE, in a mean follow-up period ranging from 30 days to 12 months, it was registered a 0% of AAA-related deaths, as well as aneurysm rupture, secondary intervention, stent migration and limb occlusion. There was a 10-11% type II endoleak rate.(24)(55)
For the most recent stent graft, Altura, there's only provisory results from the ELEVATE registry; At 1 year, clinical success was obtained in 97.3% of the 103 initial patients, type I endoleak rate was 1%, and there are no recorded cases of migration. There are now 30 Altura treated patients with 2-year follow-up and all of them are free from type I endoleak, as are the 12 patients with 3-year follow-up. At 3 years, no migrations are reported. A 1000 patients multicenter registry, ALTITUDE study, started in 2017.(56)
Unfortunately, there is no recent data available neither for E-vita ABDOMINAL XT nor E-tegra.
In what concerns to fenestrated and branched devices, the obtained results in the different studies are also similar. (Table 4)
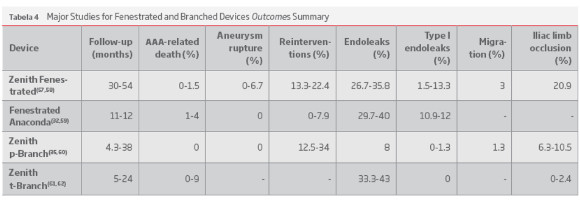
The Zenith Fenestrated endograft, in a mean follow-up period of 30-54 months, presented 0-1.5% of AAA-related death, 0-6.7% of aneurysm rupture, 13.3-22.4% of secondary intervention, 1.5-13.3% of type I endoleaks, 3% of stent migration (≥10 mm) and 20.9% of limb occlusion.(57)(58)
The Fenestrated Anaconda stent graft, in a mean follow-up period of 11-12 months, presented 1-4% of AAA-related death, 0% of aneurysm rupture, 0-7.9% of secondary intervention and 10.9-12% of type I endoleaks.(32)(59)
The Zenith p-Branch endograft, in a mean follow-up period of 4.3-38 months, presented no AAA-related death nor aneurysm rupture; 12.5-34% of secondary intervention, 0-1.3% of type I endoleaks, 1.3% of stent migration (≥10 mm) and 6.3-10.5% of limb occlusion.(35)(60)
The Zenith t-Branch thoracoabdominal endograft, in a mean follow-up period of 5-24 months, presented 0-9% of AAA-related death, 0% of type I endoleaks, and 0-2.4% of limb occlusion.(61)(62)
A major flaw in many of these endografts outcomes is the lack of long-term data.
While the older stent grafts, like Zenith, Excluder and Endurant have long-term (≥ 5 years) results published, other stent grafts recently introduced, only have short to midterm data available. This makes the comparison between different endografts unreasonable. Despite this, the few available long-term outcomes withstand the effectiveness and safety of EVAR technique.
From the data presented in this review, it can be settled that new generation endografts perform better, particularly in challenging anatomies. The paradigmatic example is the Gore C3 Excluder. The C3 system results in reduced procedural time and, simultaneously, it allows a great number of patients to be eligible for EVAR. Despite there was no significant difference in what concerns to major adverse events neither in survival rates, compared to the previous generation, the C3 system demonstrated to be safer and more effective in high-risk patients.(14)
Furthermore, the comparative studies point out that more recent endoprosthesis are associated with less complications, re-intervention and mortality rates; and are more implanted in challenging anatomies. Verzini et al. reported a higher 7-year freedom from reintervention and late conversion events (83.6 vs. 74.2%, 96.1 vs 89.1%) for the newer endografts.(63) In a single center study comparing the outcomes of Endurant with Talent, its predecessor, the rate of type I endoleak was higher for the Talent group (5.7 vs. 2.8%, p=0.614). Type III endoleaks were reported only in this group (2.9%, p=0.493) while type II endoleaks were significantly more frequent in patients treated with the old-generation endograft (28.6 vs. 8.3%, p=0.035).(64) However, continuous surveillance is imperative whether old grafts or new generation stents are used.(2)(65)
Reports from different stent graft performance reveal that EVAR represents a safe and efficient modality of treatment regardless of the type of endograft used, as long as compliance to IFU for each stent graft is respected.(66-69)
It's of high importance to emphasize that no randomized comparative trial between different stent grafts has been carried out. This epitomizes the difficulty in generalizing the selection of the appropriate device and, on the reverse side of the coin, the ephemerality of endografts.
CONCLUSION
New-generation endografts appear to provide better results while broadening eligibility criteria. Long-term data performance seems to be similar for the different devices.
This reinforces the need for a tailored selection of devices according to patient's anatomy. Still, further long-term studies are needed to assure differences in EVAR durability and efficacy between different devices.
REFERENCES
1. Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminal graft implantation for abdominal aortic aneurysms. Ann Vasc Surg. 1991;5(6):491-9. [ Links ]
2. Schoretsanitis N, Georgakarakos E, Argyriou C, Ktenidis K, Georgiadis GS. A critical appraisal of endovascular stent-grafts in the management of abdominal aortic aneurysms. Radiol Med. 2017;122(4):309-18. [ Links ]
3. Bastos Goncalves F, Rouwet Ellen V, Metz R, Hendriks JM, Vrancken Peeters M, Muhs BE, et al. Device-specific outcomes after endovascular abdominal aortic aneurysm repair. J Cardiovasc Surg (Torino). 2010;51(4):515-31. [ Links ]
4. Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG, participants Et. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: randomised controlled trial. Lancet. 2004;364(9437):843-8. [ Links ]
5. Prinssen M, Buskens E, Blankensteijn JD. The Dutch Randomised Endovascular Aneurysm Management (DREAM) trial. Background, design and methods. J Cardiovasc Surg (Torino). 2002;43(3):379-84. [ Links ] [ Links ]
7. Oliveira-Pinto J ON, Bastos-Gonçalves F, Hoeks S, Van Rijn MJ, Ten Raa S. Long term results of outside "instructions for use" EVAR. The Journal of Cardiovascular Surgery. 2017. [ Links ]
8. Bryce Y, Rogoff P, Romanelli D, Reichle R. Endovascular repair of abdominal aortic aneurysms: vascular anatomy, device selection, procedure, and procedure-specific complications. Radiographics. 2015;35(2):593-615. [ Links ]
9. Michael Marin CC, Daniel Fremed, Daniel Han, Peter Faries. Update on the use of abdominal and thoracic endografts for treating aortic aneurysms. Expert Review of Medical Devices. 2016. [ Links ]
10. Ricotta JJ, 2nd, Oderich GS. The Cook Zenith AAA endovascular graft. Perspect Vasc Surg Endovasc Ther. 2008;20(2):167-73. [ Links ]
11. Welborn MB, III, McDaniel HB, Johnson RC, Kennedy RE, Knott A, Mundinger GH, et al. Clinical outcome of an extended proximal seal zone with the AFX endovascular aortic aneurysm system. Journal of Vascular Surgery. 2014;60(4):876-84. [ Links ]
12. Kouvelos GN, Nana P, Bouris V, Peroulis M, Drakou A, Rousas N, et al. Initial Clinical Experience with the Endologix AFX Unibody Stent Graft System for Treating Patients with Abdominal Aortic Aneurysms: A Case Controlled Comparative Study. Vasc Specialist Int. 2017;33(1):16-21. [ Links ]
13. Eckroth-Bernard K, Garvin R, Ryer E. Current status of endovascular devices to treat abdominal aortic aneurysms. Biomed Eng Comput Biol. 2013;5:25-32. [ Links ]
14. Bergonti M, Teruzzi G, Santagostino G, Grancini L, Ferrari C, Trabattoni D, et al. Third- versus Second-Generation Stent Graft for Endovascular Aneurysm Repair: A Device-Specific Analysis. Annals of Vascular Surgery. 2017.
15. Katsargyris A, Mufty H, Wojs R, Utech G, Verhoeven EL. Single-centre experience with the Gore C3 Excluder stent-graft in 200 consecutive patients. J Cardiovasc Surg (Torino). 2016;57(4):485-90. [ Links ]
16. Michael M. McNally SLS. The story of evolution of endovascular aneurysm repair and the Gore Excluder Device. Supplement to Endovascular Today. 2017;16(3):4. [ Links ]
17. Carpenter JP, Baum RA, Barker CF, Golden MA, Mitchell ME, Velazquez OC, et al. Impact of exclusion criteria on patient selection for endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2001;34(6):1050-4. [ Links ]
18. Sirignano P, Mansour W, Pranteda C, Siani A, Accrocca F, d'Adamo A, et al. Real life experience with Ovation stent-graft: lesson learned from first hundred-fifty treated patients. Annals of Vascular Surgery. 2017. [ Links ]
19. Perdikides T, Georgiadis GS, Avgerinos ED, Fotis T, Verikokos C, Hopkinson BR, et al. The Aorfix stent-graft to treat infrarenal abdominal aortic aneurysms with angulated necks and/or tortuous iliac arteries: midterm results. J Endovasc Ther. 2009;16(5):567-76. [ Links ]
20. Rodel SG, Geelkerken RH, Prescott RJ, Florek HJ, Kasprzak P, Brunkwall J, et al. The Anaconda AAA stent graft system: 2-year clinical and technical results of a multicentre clinical evaluation. Eur J Vasc Endovasc Surg. 2009;38(6):732-40. [ Links ]
21. Rodel SG, Zeebregts CJ, Huisman AB, Geelkerken RH, Multicenter Angulated Neck Study with the Anaconda study p. Results of the Anaconda endovascular graft in abdominal aortic aneurysm with a severe angulated infrarenal neck. J Vasc Surg. 2014;59(6):1495-501, 501 e1. [ Links ]
22. Scheinert D, Pratesi C, Chiesa R, Coppi G, Brunkwall JS, Klarenbeek G, et al. First-in-human study of the INCRAFT endograft in patients with infrarenal abdominal aortic aneurysms in the INNOVATION trial. J Vasc Surg. 2013;57(4):906-14. [ Links ]
23. Sugimoto M, Torsello GF, Torsello GB, Austermann M, Stachmann A, Bisdas T. Postmarket Clinical Experience with the INCRAFT AAA Stent Graft System for Challenging Access Routes. Ann Vasc Surg. 2017;40:120-7. [ Links ]
24. Chiesa R, Riambau V, Coppi G, Zipfel B, Llagostera S, Marone EM, et al. The Bolton Treovance abdominal stent-graft: European clinical trial design. J Cardiovasc Surg (Torino). 2012;53(5):595-604. [ Links ]
25. Rylski B, Czerny M, Sudkamp M, Russe M, Siep M, Beyersdorf F. Fenestrated and Branched Aortic Grafts. Dtsch Arztebl Int.2015;112(48):816-22. [ Links ]
26. Graves HL, Jackson BM. The Current State of Fenestrated and Branched Devices for Abdominal Aortic Aneurysm Repair. Semin Intervent Radiol. 2015;32(3):304-10. [ Links ]
27. Oderich GS, Correa MP, Mendes BC. Technical aspects of repair of juxtarenal abdominal aortic aneurysms using the Zenith fenes¬trated endovascular stent graft. J Vasc Surg. 2014;59(5):1456-61. [ Links ]
28. Bungay PM, Burfitt N, Sritharan K, Muir L, Khan SL, De Nunzio MC, et al. Initial experience with a new fenestrated stent graft. J Vasc Surg. 2011;54(6):1832-8. [ Links ]
29. Bakoyiannis CN, Economopoulos KP, Georgopoulos S, Klonaris C, Shialarou M, Kafeza M, et al. Fenestrated and branched endogra¬fts for the treatment of thoracoabdominal aortic aneurysms: a systematic review. J Endovasc Ther. 2010;17(2):201-9. [ Links ]
30. Shahverdyan R, Gray D, Gawenda M, Brunkwall J. Technical feasi¬bility of endovascular aortoiliac aneurysm repair combining Anaconda fenestrated and Zenith iliac side-branched stent grafts. J Vasc Surg. 2015;61(5):1324-8. [ Links ]
31. Rolls AE, Jenkins M, Bicknell CD, Riga CV, Cheshire NJ, Burfitt N, et al. Experience with a novel custom-made fenestrated stent graft in the repair of juxtarenal and type IV thoracoabdominal aneurys¬ms. J Vasc Surg. 2014;59(3):615-22. [ Links ]
32. Dijkstra ML, Tielliu IF, Meerwaldt R, Pierie M, van Brussel J, Schurink GW, et al. Dutch experience with the fenestrated Anaconda endograft for short-neck infrarenal and juxtarenal abdominal aortic aneurysm repair. J Vasc Surg. 2014;60(2):301-7. [ Links ]
33. Tim Resch M, PhD. Global Experience With the Zenith p-Branch Device. Endovascular Today. 2015. [ Links ]
34. Mark Farber M. Current State and Future of Fenestrated Techno¬logy. Endovascular Today. 2013. [ Links ]
35. Kitagawa A, Greenberg RK, Eagleton MJ, Mastracci TM. Zenith p-branch standard fenestrated endovascular graft for juxtarenal abdominal aortic aneurysms. J Vasc Surg. 2013;58(2):291-300. [ Links ]
36. Nordon IM, Thompson MM, Loftus IM. Are concerns about EVAR durability relevant with modern devices? J Cardiovasc Surg (Tori¬no). 2013;54(2):181-9. [ Links ]
37. Bisdas T, Weiss K, Eisenack M, Austermann M, Torsello G, Donas KP. Durability of the Endurant stent graft in patients undergoing endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2014;60(5):1125-31. [ Links ]
38. Verzini F, Romano L, Parlani G, Isernia G, Simonte G, Loschi D, et al. Fourteen-year outcomes of abdominal aortic endovascular repair with the Zenith stent graft. J Vasc Surg. 2017;65(2):318-29. [ Links ]
39. t Mannetje YW, Cuypers PWM, Saleem BR, Bode AS, Teijink JAW, van Sambeek M. Comparison of midterm results for the Talent and Endurant stent graft. J Vasc Surg. 2017;66(3):735-42.
40. Verhoeven EL, Katsargyris A, Bachoo P, Larzon T, Fisher R, Ettles D, et al. Real-world performance of the new C3 Gore Excluder stent-graft: 1-year results from the European C3 module of the Global Registry for Endovascular Aortic Treatment (GREAT). Eur J Vasc Endovasc Surg. 2014;48(2):131-7. [ Links ]
41. Mertens J, Houthoofd S, Daenens K, Fourneau I, Maleux G, Lerut P, et al. Long-term results after endovascular abdominal aortic aneurysm repair using the Cook Zenith endograft. J Vasc Surg. 2011;54(1):48-57 e2. [ Links ]
42. Melas N, Stavridis K, Saratzis A, Lazarides J, Gitas C, Saratzis N. Active proximal sealing in the endovascular repair of abdominal aortic aneurysms: early results with a new stent-graft. J Endo¬vasc Ther. 2015;22(2):174-8. [ Links ]
43. Verhoeven EL KA, Milner R. The GREAT registry: lessons learned from real-world experience with the GORE® C3® delivery system. Endovascular Today. 2013. [ Links ]
44. Bastos Goncalves F, Jairam A, Voute MT, Moelker AD, Rouwet EV, ten Raa S, et al. Clinical outcome and morphologic analysis after endovascular aneurysm repair using the Excluder endograft. J Vasc Surg. 2012;56(4):920-8. [ Links ]
45. Pratesi C, Piffaretti G, Pratesi G, Castelli P, Investigators ITER. ITalian Excluder Registry and results of Gore Excluder endo¬graft for the treatment of elective infrarenal abdominal aortic aneurysms. J Vasc Surg. 2014;59(1):52-7 e1. [ Links ]
46. Rouwet EV, Torsello G, de Vries JP, Cuypers P, van Herwaarden JA, Eckstein HH, et al. Final results of the prospective European trial of the Endurant stent graft for endovascular abdominal aortic aneurysm repair. Eur J Vasc Endovasc Surg. 2011;42(4):489-97. [ Links ]
47. Stokmans RA, Teijink JAW, Forbes TL, Böckler D, Peeters PJ, Riam¬bau V, et al. Early Results from the ENGAGE Registry: Real-world Performance of the Endurant Stent Graft for Endovascular AAA Repair in 1262 Patients. European Journal of Vascular and Endo¬vascular Surgery. 2012;44(4):369-75. [ Links ]
48. 4Zandvoort HJ, Goncalves FB, Verhagen HJ, Werson DA, Moll FL, de Vries JP, et al. Results of endovascular repair of infrarenal aortic aneurysms using the Endurant stent graft. J Vasc Surg. 2014;59(5):1195-202.
49. Singh MJ, Fairman R, Anain P, Jordan WD, Maldonado T, Samson R, et al. Final results of the Endurant Stent Graft System in the United States regulatory trial. J Vasc Surg. 2016;64(1):55-62. [ Links ]
50. Hyhlik-Durr A, Weber TF, Kotelis D, Rengier F, Gahlen J, Bock S, et al. The Endurant Stent Graft System: 15-month follow-up report in patients with challenging abdominal aortic anatomies. Langen¬becks Arch Surg. 2011;396(6):801-10. [ Links ]
51. Mehta M, Valdes FE, Nolte T, Mishkel GJ, Jordan WD, Gray B, et al. One-year outcomes from an international study of the Ovation Abdominal Stent Graft System for endovascular aneurysm repair. J Vasc Surg. 2014;59(1):65-73 e1-3. [ Links ]
52. Malas MB, Hicks CW, Jordan WD, Jr., Hodgson KJ, Mills JL, Sr., Maka¬roun MS, et al. Five-year outcomes of the PYTHAGORAS U.S. clinical trial of the Aorfix endograft for endovascular aneurysm repair in patients with highly angulated aortic necks. J Vasc Surg. 2017;65(6):1598-607.
53. Volpe P, Massara M, Alberti A, Marino S, Volpe A, Mazzaccaro D, et al. Preliminary Results of Aorfix Stent Graft to Treat Infrarenal Abdominal Aortic Aneurysms with Severe Proximal Aortic Neck Angulation. Ann Vasc Surg. 2017. [ Links ]
54. Weale AR, Balasubramaniam K, Macierewicz J, Hardman J, Horrocks M. Outcome and safety of Aorfix stent graft in highly angulated necks - a prospective observational study (arbiter 2). Eur J Vasc Endovasc Surg. 2011;41(3):337-43. [ Links ]
55. Georgakarakos E, Pitoulias G, Schoretsanitis N, Argyriou C, Mavros DM, Lazarides MK, et al. Early Results of the Bolton Treo¬vance Endograft in the Treatment of Abdominal Aortic Aneurys¬ms. J Endovasc Ther. 2017:1526602817713736. [ Links ]
56. Paul Heyes M. Evolution Not Revolution: The Altura Stent Graft. Insert to Endovascular Today Europe.5(2):5. [ Links ]
57. Hu Z, Li Y, Peng R, Liu J, Zhang T, Guo W. Experience With Fenestra¬ted Endovascular Repair of Juxtarenal Abdominal Aortic Aneurys¬ms at a Single Center. Medicine (Baltimore). 2016;95(10):e2683. [ Links ]
58. Oderich GS, Greenberg RK, Farber M, Lyden S, Sanchez L, Fairman R, et al. Results of the United States multicenter prospective study evaluating the Zenith fenestrated endovascular graft for treatment of juxtarenal abdominal aortic aneurysms. J Vasc Surg. 2014;60(6):1420-8 e1-5. [ Links ]
59. Colgan FE, Bungay PM, Burfitt N, Hatrick A, Clarke MJ, Davies AH, et al. Operative and 1-Year Outcomes of the Custom-Made Fenes¬trated Anaconda Aortic Stent Graft-A UK Multicenter Study. Ann Vasc Surg. 2018;46:257-64. [ Links ]
60. Farber MA, Eagleton MJ, Mastracci TM, McKinsey JF, Vallabhaneni R, Sonesson B, et al. Results from multiple prospective single¬-center clinical trials of the off-the-shelf p-Branch fenestrated stent graft. J Vasc Surg. 2017;66(4):982-90. [ Links ]
61. Spanos K, Kolbel T, Theodorakopoulou M, Heidemann F, Rohlffs F, Debus ES, et al. Early Outcomes of the t-Branch Off-the-Shelf Multibranched Stent-Graft in Urgent Thoracoabdominal Aortic Aneurysm Repair. J Endovasc Ther. 2018;25(1):31-9. [ Links ]
62. Bosiers MJ, Bisdas T, Donas KP, Torsello G, Austermann M. Early expe¬rience with the first commercially available off-the-shelf multibran¬ched endograft (t-branch) in the treatment of thoracoabdominal aortic aneurysms. J Endovasc Ther. 2013;20(6):719-25. [ Links ]
63. Verzini F, Isernia G, De Rango P, Simonte G, Parlani G, Loschi D, et al. Abdominal aortic endografting beyond the trials: a 15-year single-center experience comparing newer to older generation stent-grafts. J Endovasc Ther. 2014;21(3):439-47. [ Links ]
64. Mensel B, Kuhn JP, Trager T, Duhrkoop M, von Bernstorff W, Rosen¬berg C, et al. Technical and clinical outcome of Talent versus Endu¬rant endografts for endovascular aortic aneurysm repair. PLoS One. 2012;7(6):e38468. [ Links ]
65. Kontopodis N, Papadopoulos G, Galanakis N, Tsetis D, Ioannou CV. Improvement of patient eligibility with the use of new genera¬tion endografts for the treatment of abdominal aortic aneurysms. A comparison study among currently used endografts and litera¬ture review. Expert Rev Med Devices. 2017;14(3):245-50. [ Links ]
66. Lee JT, Ullery BW, Zarins CK, Olcott Ct, Harris EJ, Jr., Dalman RL. EVAR deployment in anatomically challenging necks outside the IFU. Eur J Vasc Endovasc Surg. 2013;46(1):65-73. [ Links ]
67. JESSICA P. SIMONS M, ANDRES SCHANZER, MD. Exploring EVAR Instructions for Use in 2016. Endovascular Today. 2016;15. [ Links ]
68. Schanzer A, Messina L. Two decades of endovascular abdominal aortic aneurysm repair: enormous progress with serious lessons learned. J Am Heart Assoc. 2012;1(3):e000075. [ Links ]
69. Lee GK, Ullery BW, Lee JT. Elective EVAR in nonagenarians is safe in carefully selected patients. Ann Vasc Surg. 2014;28(6):1402-8. [ Links ]
Correio eletrónico: anafilipa1111@gmail.com (F. Cordeiro).
Recebido a 02 de março de 2018
Aceite a 07 de junho de 2018

