










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkAngiologia e Cirurgia Vascular
versão impressa ISSN 1646-706X
Angiol Cir Vasc vol.15 no.4 Lisboa dez. 2019
ARTIGO ORIGINAL
Venous arterialization for some patients with no option critical limb ischemia - a desperate attempt or an experience-proved successful technique?
Arterialização venosa para alguns doentes com isquemia crítica sem outra opção - uma tentativa desesperada ou um tratamento de sucesso comprovado?
Inês Antunes1, Carlos Pereira1, Luís Loureiro1, Gabriela Teixeira1, Carlos Veiga1, Daniel Mendes1, Carlos Veterano1, Henrique Rocha1, João Castro1, Rui Almeida1
1 Serviço de Angiologia e Cirurgia Vascular, Centro Hospitalar do Porto, Porto, Portugal
Endereço para correspondência | Dirección para correspondencia | Correspondence
ABSTRACT
Introduction: Between 14-20% of patients with critical lower-limb ischemia (CLI) are not candidates for revascularization due to extensive occlusions in crural/pedal vessels. Frequently these patients are young and functionally active. In these cases, the concept of shunting blood through veins to get this reversed flow to reach the nutritive tissue capillary bed becomes attractive. Our aim is to report our very recent experience in venous arterialization.
Material/Methods: We retrospectively reviewed the cases of venous arterialization performed in our institution between April 2018-2019.
Results: Four patients were treated: 3 males/1 female with mean age of 58.5 years. All patients had PAD stage 4. All patients were studied with arteriography and ultrasound and were considerate no revascularizable (2 of them after an attempt of endovascular/surgical treatment). In one patient a trial with endovenous prostaglandin was performed, without clinical response. In all cases, the patients were facing a major amputation. Arterialization was performed as a last attempt to save the limb. Regarding the surgical procedures, the donor inflow artery was the infragenicular popliteal artery in 2 cases, distal femoral artery in 1 case and anterior tibial artery in 1 case. In 3 cases the bypass used the great saphenous vein (GSV) in situ to arterialize the medial marginal vein; in 1 case was used an inverted GSV bypass with the distal anastomosis at the posterior tibial vein. The venous valves were destroyed by combination of Fogarty catheter (proximally) and angioplasty balloon (distally). Collaterals were ligated to focalize the blood flow. In all patients marked improvement in foot perfusion was achieved. Two of them had excellent evolution in the postoperative period and healed foot lesions. One patient was amputated with permeable bypass. One patient presented good initial evolution but later had bypass thrombosis (presumably due to inadequate arterial inflow from the anterior tibial artery) and undergone major amputation.
Discussion/Conclusions: Despite advances in surgical and endovascular techniques, an important number of patients with CLI are not candidates to arterial revascularization and most patients with inoperable CLI will face a major amputation. In that setting, venous arterialization should be considered but not all patients are candidates to this procedure and a careful preoperative evaluation is required. Our preliminary experience is encouraging: the procedure was relatively straightforward, the resulting improve in foot perfusion was surprisingly good, the patency rate and limb salvage rate was 75 and 50%. In our opinion the major issues are selection of inflow artery and outflow vein and the learning curve in interpretation of the angiographic result to guide optimal focalization of the blood flow.
Keywords: Venous arterialization; Critical limb ischemia; Major amputation; Revascularization procedures
RESUMO
Introdução: Entre 14 a 20% dos doentes com isquemia crítica não são candidatos para revascularização dada a extensa doença oclusiva nas artérias crurais/pé. Frequentemente estes doentes são jovens e ativos e, nestes casos, o conceito de fazer aumentar o fluxo sanguíneo através de veias com o objetivo de obter um fluxo sanguíneo a nível da rede capilar torna-se atrativa. O nosso objetivo é apresentar a nossa muito recente experiência em arterializações venosas.
Materiais/Métodos: Revisão retrospetiva dos casos clínicos de aretrialização venosa realizados na nossa instituição entre abril 2018 - 2019.
Resultados: Foram tratados 4 doentes: 3 homens/1 mulher com idade média de 58.5 anos. Todos os doentes apresentavam doença arterial periférica grau IV. Todos os doentes foram estudados com ecodoppler e com angiografia e foram considerados não revascularizáveis (2 deles após uma tentativa de revascularização). Em 1 doente foi tentado um ciclo de prostagandina endovenosa, sem resposta clínica. Em todos os casos o tratamento alterativo seria a amputação major. A arterialização representou uma última tentativa para salvar o membro. Relativamente à técnica cirúrgica, a artéria dadora de inflow foi a poplítea infra-genicular em dois casos, a femoral superficial distal em 1 e a tibial anterior em 1 caso. Em 3 casos foi utiizada veia grande safena (VGS) in situ para arterializar a veia mediana marginal; em 1 caso foi usada a VGS invertida como conduto de bypass com a anastomose distal a veia tibial posterior. A destruição valvular foi feita com recurso a catéter Fogarty (proximalmente) e a balão de angioplastia (distalmente). As colaterais foram laqueadas de modo a direccionar o fluxo sanguíneo. Em todos os doentes foi percetível uma melhoria na perfusão do pé no pós-operatório. Dois deles tiveram boa evolução e cicatrizaram as lesões do pé. Um doente foi submetido a amputação major (transtibioperoneal) com bypass permeável. Um doente apresentou boa evolução inicial, mas teve trombose do bypass (presumivelmente devido a inadequado inflow da artéria tibial anterior) e foi submetido a amputação major (transtibioperoneal).
Discussão/Conclusões: Apesar dos avanços nas técnicas de revascularização (cirúrgicas e endovascualres), um número importante de doentes com isquemia crítica não são candidatos para revascularização e a maioria deles irá enfrentar uma amputação major. A arterialização venosa deve ser considerada, mas nem todos os doentes são candidatos a este tratamento e uma cuidada avaliação pré-operatória é fundamental. A nossa muito recente experiência é encorajadora: o procedimento é relativamente simples, os resultados em termos de melhoria da perfusão do pé são surpreendentemente bons, a permeabilidade e salvamento do membro são respetivamente 75 e 50%. Na nossa opinião, as principais dificuldades são a seleção da artéria de inflow e da veia de outflow e a curva de aprendizagem na interpretação do resultado angiográfico para a ótima focalização do fluxo sanguíneo.
Palavras-chave: Arterialização venosa; Isquemia crítica membro; Amputação; Revascularização
Introduction
In the past, several patients (almost 50% in some reports) were not candidates for revascularization due to extensive occlusions in crural and pedal arteries(1). With the progress of endovascular procedures (techniques and materials), the number of patients considered with no revascularization potential has decreased(2). But still, there is a number of patients (between 14-20%) with critical limb ischemia (CLI) who are not candidates for revascularization, especially diabetic and end-stage renal disease patients that normally have severe and heavy calcified occlusive disease, frequently with extension to the below the ankle level(3). For these patients, several therapeutic alternatives have been explored, such as: prostanoid therapy, stem cell therapy and spinal cord stimulation; from these 3 therapeutic alternatives, only spinal cord stimulation showed a potential benefit for preventing amputation based in a Cochrane review, but with very low grade evidence(4-6). Also, frequently these no revascularizable patients are young and functionally active and an effort to find alternative techniques to improve foot perfusion have been developed, such as venous arterialization. In fact, the concept of shunting blood through deep/superficial veins to get this reversed flow to reach the nutritive tissue capillary bed becomes attractive. Halstead and Vaughan first published this concept in 1912(7). Since then, venous arterialization has been described as a last attempt of vascularization in patients facing a major amputation, with variable results.
Our aim is to report our very recent experience in venous arterialization. Between April 2018 to April 2019 we treated 4 patients with venous arterialization. All patients are young (with a mean age of 58.5 years), functionally active and facing a major amputation at the time of the procedure.
Clinical Cases
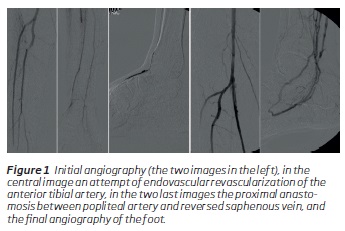
The first patient was a 63-year-old male, hospitalized because of gangrene of 3 toes, submitted to transmetatarsal amputation. An angiography was performed (Figure 1) that showed: permeability of the femoro-popliteal sector with no stenosis; concerning crural arteries the patient had an occlusion of the posterior tibial artery, the anterior tibial and peroneal arteries were permeable until the distal third of the leg, but with no visible arteries in the foot. We performed an attempt of endovascular revascularization (Figure 1), without success and so, the patient was considered no revascularizable. Given the bad evolution of the foot and patient characteristics (age, physical status), we decided to make a last try to improve the perfusion of the foot with a venous arterialization. As inflow artery we chose the infragenicular popliteal artery, as conduit we used the great saphenous vein (GSV) in an inverted position. The distal outflow vein was the posterior tibial vein. With a 2mm diameter angioplasty balloon, we dilated the foot venous arcade. Final control angiography revealed no technical defects in the anastomoses and a good flow to the foot (Figure 1). In the postoperative period, there was a notable improvement in foot perfusion, but despite the functional bypass, there was a bad evolution of the foot with difficult to control infection and the patient was submitted to a major (below the knee) amputation 21 days after the bypass surgery.
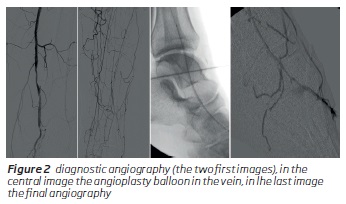
Second case was a 56-year-old male that came to the emergency department with toe gangrene. Due to extensive aortoiliac disease, the patient was submitted to an aortobifemoral bypass and, in the same time, toe amputation was performed. Despite the proximal revascularization, the amputation stump maintained bad evolution and we considered that a distal revascularization was mandatory. The patient was submitted to an angiography (Figure 2) which revealed permeability of the femoral artery (without important stenosis), occlusion of the popliteal artery and, concerning crural arteries, only the distal peroneal artery was discernible, with no arteries in the foot. The foot maintained a bad evolution with progression of gangrene and the patient was submitted to a surgical revision of the stump, but the stump maintained bad evolution after that despite antibiotic therapy and optimized wound care. We decided to do a last attempt for revascularization through venous arterialization. As inflow artery, we used de distal femoral artery and as conduit, we used the GSV in situ. To destroy the valves we used a Fogarty 3 catheter (for more proximal) and a 3mm diameter angioplasty balloon for the distal vein (Figure 2). After that, we performed an angiography with identification of the major collaterals that diverted the flow of the forefoot and we surgically ligated these collateral veins. In the same procedure, we performed a transmetatarsal amputation. Due to uncontrolled infection, several debridement procedures of the stump were performed, and the stump presented an excellent evolution after that with negative pressure dressing.
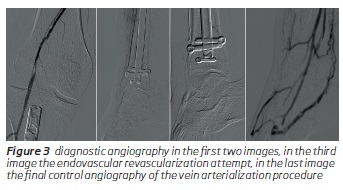
The third case was a 47-year-old female with toe necroses. A diagnostic angiography was performed and showed: a stenosis in the popliteal artery, occlusion of the posterior tibial artery, the peroneal and anterior tibial arteries were permeable up until the distal third of the leg, with no arteries discernible in the foot (Figure 3). We performed an angioplasty of the popliteal artery stenosis and an unsuccessful attempt of endovascular revascularization of the pedal artery (Figure 3). The patient maintained a bad evolution of the foot with necrosis progression and uncontrolled pain. We decided that it was necessary to perform another attempt of revascularization, so we proceeded to a surgical exploration of the pedal artery (completely occluded, with no conditions for bypass) and we performed a venous arterialization at the same time. The selected inflow artery was the anterior tibial artery and we used as conduit the GSV in situ. To destroy the valves, we used an angioplasty balloon 2.5mm diameter, we performed an angiography with identification of the major collaterals that diverted blood flow and ligated these collaterals. The final control angiography was satisfactory (Figure 3). The bypass thrombosed at the 15th post-operative day, an attempt to recover the bypass was unsuccessful. We performed a transmetatarsal amputation, but the stump presented a bad evolution and the patient was submitted to a major (below the knee) amputation.
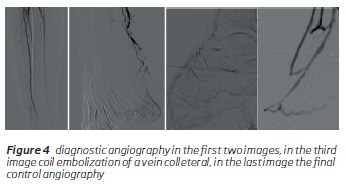
The fourth case was a 68-year-old male admitted due to toe necrosis. A diagnostic angiography was performed and showed: an occlusion of the anterior tibial artery and occlusion of the posterior tibial artery in the ankle, with no arteries discernible in the foot (Figure 4). We decided to perform an attempt of revascularization through vein arterialization. The inflow artery was the infragenicular popliteal artery and the used conduit was GSV in situ. The destruction of the valves was performed with a Fogarty 3 catheter and angioplasty balloon 3.5mm diameter. We performed an angiography with identification of the major collaterals that diverted blood flow and occluded these collaterals with surgical ligation and coil embolization (in 1 collateral) (Figure 4). After the procedure there was an immediately improvement in foot perfusion, we proceeded to toe amputation that healed properly. The patient developed foot edema that we are still managing.
Critical limb ischemia is associated with poor quality of life and high amputation and mortality rates(8). Conventional surgery (bypass) and endovascular techniques have become the treatment of choice for these patients to prevent amputation.
Venous arterialization has been pointed as an alternative technique for some, but not all, patients. The main principle is that, by improving the blood flow in the venous bed, the reversal flow through the capillary vessels will occur, improving tissue nutrition and possibly promoting angiogenesis(9,10).
Regarding the surgical technique, there is still controversy and there is no established surgical strategy. Regarding the proximal anastomosis to the donor inflow artery, there is an almost consensual opinion that the most distal patent artery should be the one used. In fact, most authors defend that using a more proximal artery implies a longer bypass, which may lead to a higher risk of occlusion. Regarding the distal anastomosis, there is no consensual information. There are two types of venous arterialization described: of superficial and of deep veins. Regarding superficial vein arterialization, there are reports where the GSV was left in situ(11-15,19); others where the bypass was anastomosed to the median marginal vein of the foot(16-19) and others where the distal anastomosis was performed to the dorsal venous arch(20-22). Regarding deep veins arterialization(23-25), the deep vein selection was based on the angiosome theory in some reports or to the adjacent deep vein to the most distal permeable artery in others. Limb salvage between these two techniques (superficial versus deep veins) were comparable. Regarding the conduit used, some studies reported only the use of GSV(11-15,17,19), others reported the use of different conduits when the GSV was not available such as: composite vein, composed graft/vein or PTFE graft. Another cause of controversy is regarding branch ligation. In fact, in some studies the authors performed a systematically ligation of side branches to ankle, but some authors defended not to perform side branch ligation in order to improve perfusion of the limb and because of they believe that it could improve bypass patency(14). In our institution we now prefer to perform arterialization of superficial veins, using the GSV in situ and we systematically proceed to occlusion of collateral veins (with surgical ligation or coil embolization) in order to direct the blood flow to the to the intended area, usually the forefoot. Another controversial issue is the medication management in the postoperative period (anticoagulant versus thrombocyte antiaggregating inhibitors) and the duration of this therapy. So, there is still a long way of improvement of the surgical technique and other studies are required to optimize the technique. Recently Percutaneous Deep Venous Arterialization (PDVA) has been developed as a less invasive procedure(26).
Regarding limb salvage, Schreve et al published, in 2017 in a systematic review of venous arterializations, that the pooled proportion of limb salvage at 12 months was 75%(2) but results are very variable between studies.
In conclusion, despite advances in surgical and endovascular techniques, an important number of patients with CLI are not candidates to arterial revascularization and most patients with inoperable CLI will face a major amputation. In that setting, venous arterialization should be considered, but not all patients are candidates to this procedure and a careful preoperative evaluation is required. Also, a standardization of surgical technique is needed. Our preliminary experience is encouraging: the procedure was relatively straightforward, the resulting improve in foot perfusion was surprisingly good, the patency rate and limb salvage rate was 75 and 50%. In our opinion the major issues are selection of inflow artery and outflow vein and the learning curve in interpretation of the angiographic result to guide optimal focalization of the blood flow.
REFERENCES
1. Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, et al. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet 2005;366(9501):1925-1934. [ Links ]
2. Schreve MA, Vos CG, Vahl AC, Vries JPPM, Kum S, Borst G, et al. Venous arterialisation for salvage of critically ischaemic limbs: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2017 (53):387-402. [ Links ]
3. Heuvel D, Schreve M, Kum S. Venous arterialization for CLI: When, Why, and How? Endovascular Today;2018(17):72-76. [ Links ]
4. Abu Dabrh AM, Steffen MW, Asi N, Undavalli C, Wang Z, Elamin MB, et al. Nonrevascularization-based treatments in patients with severe or critical limb ischemia. J Vasc Surg. 2015(62):1330-1339. [ Links ]
5. Peeters Weem SM, Teraa M, Borst GJ, Verhaar MC, Moll FL. Bone marrow derived cell therapy in critical limb ischemia: a meta-analysis of randomized placebo controlled trials. Eur J Vasc Endovasc Surg. 2015(50):775-783. [ Links ]
6. Ubbink DT, Vermeulen H. Spinal cord stimulation for nonreconstructable chronic critical leg ischaemia. Cochrane Data-base Syst Rev. 2005:CD004001. [ Links ]
7. Halstead AE, Vaughan RT. Arteriovenous anastomosis in the treatment of gangrene of the extremities. Surg Gynecol Obstet. 1912;14:1. [ Links ]
8. Sprengers RW, Teraa M, Moll FL, De Wit GA, Van der Graaf Y, Verhaar MC. Quality of life in patients with no-option critical limb ischemia underlines the need for new effective treatment. J Vasc Surg 2010;52:843-844. [ Links ]
9. Ozek C, Zhang F, Lineaweaver WC, Chin BT, Newlin L, Eiman T, et al. Arterialization of the venous system in a rat lower limb model. Br J Plast Surg. 1997;50:402-407. [ Links ]
10. Baffour R, Danylewick R, Burdon T, Sniderman A, Common A, Graham A, et al. An angiographic study of ischemia as determinant of neovascularisation in arteriovenous reversal. Surg Ginecol Obstet 1988;166:28-32. [ Links ]
11. Busato CR, Utrabo II Cal, Gomes RZ, Hoeldtke E, Housome II JK, Costa DMM, et al. The great saphenous vein in situ for the arterialisation of the venous arch of the foot. J Vasc Bras 2010;9:119-123. [ Links ]
12. Djoric P. Early individual experience with distal venous arterialization as a lower limb salvage procedure. Am Surg 2011;77:726-730. [ Links ]
13. Djoric P., Zeleskov-Djoric J., Stanisavljevic D.M., Markovic Z.D., Zivkovic V., Vuletic M., et al. Distal venous arterialization and reperfusion injury: focus on oxidative status. Eur Surg Res 2012;48:200-207. [ Links ]
14. Gavrilenko A.V., and Skrylev S.I. Long-term results of venous blood flow arterialization of the leg and foot in patients with critical lower limb ischemia. Angiol Sosud Khir 2007; 13: 95-103. [ Links ]
15. Mätzke S., Pitkänen J., and Lepäntalo M.: Does saphenous vein arterialisation prevent major amputation in critical leg ischaemia? A comparative study. J Cardiovasc Surg (Torino) 1999; 40:845-847. [ Links ]
16. Lengua F., Cohen R., L'Huiller B., and Buffet J.M. Arteriovenous revascularization for lower limb salvage in unreconstructible arterial occlusive disease (long term outcome). Vasa 1995; 24:261-269. [ Links ]
17. Lengua F., La Madrid A., Acosta C., and Vargas J. Temporal venous arterialization of the diabetic foot. J Vasc Bras 2010; 9:14-20. [ Links ]
18. Mutirangura P., Ruangsetakit C., Wongwanit C., Sermsathanasawadi N., and Chinsakchai K. Pedal bypass with deep venous arterialization: the therapeutic option in critical limb ischemia and unreconstructable distal arteries. Vascular 2011; 19:313-319. [ Links ]
19. Schreve M.A., Minnee R.C., Bosma J., Leijdekkers V.J., Idu M.M., and Vahl A.C. Comparative study of venous arterialization and pedal bypass in a patient cohort with critical limb ischemia. Ann Vasc Surg 2014;28:1123-1127. [ Links ]
20. Engelke C., Morgan R.A., Quarmby J.W., Taylor R.S., and Belli A.M. Distal venous arterialization for lower limb salvage: angiographic appearances and interventional procedures. Radiographics 2001;21:1239-1248. [ Links ]
21. Houlind K., Christensen J., Hallenberg C., and Jepsen J.M. Early results from an angiosome-directed open surgical technique for venous arterialization in patients with critical lower limb ischemia. Diabet Foot Ankle 2013;4:22713. [ Links ]
22. Taylor R.S., Belli A.M., and Jacob S. Distal venous arterialisation for salvage of critically ischaemic inoperable limbs. Lancet 1999; 354: 1962-1965. [ Links ]
23. Alexandrescu V., Ngongang C., Vincent G., Ledent G., and Hubermont G. Deep calf veins arterialization for inferior limb preservation in diabetic patients with extended ischaemic wounds, unfit for direct arterial reconstruction: preliminary results according to an angiosome model of perfusion. Cardiovasc Revasc Med 2011;12:10-19. [ Links ]
24. Vira Reddi H.T., and Nath L.S. New concepts in the management of ischaemic lower extremities. Int Angiol 1990;9:97-104. [ Links ]
25. Wu Z.Q., Jiang X.P., Wu Z.P., Zhang L., Liu X.M., Xia G.H., et al. Experimental and clinical studies on one-stage arterialization of the venous channels for revascularization of severely ischemic limbs. Chin Med J (Engl) 1993;106:814-820. [ Links ]
26. Kum S, Tan YK, Tang T, Schmidt A, Scheinert D, Ferraresi R. Percutaneous deep venous arterialization: A brief technical overview of a new therapy for treating end-stage “no-option” critical limb ischemia. Endovascular Today. 2015:80-83.
Endereço para correspondência | Dirección para correspondencia | Correspondence
Correio eletrónico: ines.antunes89@gmail.com (I. Antunes).
Recebido a 15 de junho de 2019
Aceite a 17 de novembro de 2019

