











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Renal ectopy is a common congenital anomaly of the kidney resulting from disruption of the normal embryologic migration of the kidneys. The incidence of renal ectopy is reported as 1 in 1000 autopsies.1 It occurs when the kidney does not ascend to the retroperitoneal renal fossa. The blood supply of the ectopic kidney is variable and may arise from the iliac arteries, aorta, and at times, the hypogastric and middle sacral arteries. The majority of patients with renal ectopy are asymptomatic, and its diagnosis is usually incidental upon pre- or post-natal ultrasonography.
Although extremely rare, aortoiliac aneurysm disease can coexist with ectopic kidney. When treatment is required, kidney preservation is vital, as is proper aneurysm repair/exclusion. Treatment modalities include open, endovascular or hybrid techniques. The optimal treatment depends on various factors such as aneurysm’s anatomy, kidney vasculature, elective or urgent setting, material availability and surgeon’s experience/preference.
The aim of this paper is to perform a non-systematic literature review on the treatment of aortoiliac aneurysmal disease in patients with concomitant ectopic kidney.
Methods
A non-systematic literature research was performed on the treatment of aortoiliac aneurysmal disease in patients with ectopic kidneys. MEDLINE databases were searched with no restrictions of time period. The key words “abdominal aortic aneurysm” and “ectopic kidney” were used for defining the search strategy. Only articles published in English were considered.
Results
Ectopic kidneys with concomitant aortoiliac aneurysmal disease have been previously reported in the literature, however its exact prevalence is unknow since it is very rare. The first reported case of a patient with a pelvic kidney associated with abdominal aortic aneurysm (AAA) dates back to 1977.2 Despite being very uncommon, concomitant aortoiliac aneurysmal disease in patients with ectopic kidneys is not unheard of. As of 2003, an extensive literature research revealed only seven reports assessing the combination of these two entities, revealing the rarity of this association.3 Since then, several more have described a multitude of treatment options.
The treatment of aortoiliac aneurysmal disease concomitant with renal ectopia is challenging and troublesome, requiring adequate preoperative planning and proper vascular anatomy assessment. CT angiography is necessary for optimal planning as is the use of good software planification. The majority of reports describe open repair (OR) alternatives for these patients, despite the growing number of endovascular repairs being reported.
Several techniques for OR are described in the literature and its choice is dictated by anatomic considerations and, to some extent, the surgeon's experience and preference.4 These techniques usually comprise prosthetic graft (Dacron or ePTFE) interposition (tube or bifurcated configuration); vessel reimplantation or complementary bypasses when required.5,6 The variability of ectopic kidneys’ vasculature may require more complex procedures to maintain adequate perfusion and avoid kidney injury. Configuration and reimplantation may vary widely according to aneurysm anatomy and kidney’s vasculature. Some of these reconstructions may be complex. As an example, a publication from 2015 reported on the use of an aortoiliac bifurcated graft and 3 kidney arteries re-implanted in the graft’s limb.7 Reports for OR techniques generally have excellent technical success, without major renal function impairment.3
Renal preservation is a concern during aortoiliac cross-clamping for vascular reconstruction. Expansion of plasmatic volume with pre-operative hydration and intraoperative administration of furosemide are usual pharmacological systemic attitudes for renal protection. The cross-clamp technique limits the warm ischaemia time to around 30 minutes, requiring a rapid and straightforward repair. Hypothermic techniques extend the warm ischaemia time beyond 30 minutes and are technically easy without the need for complex material or devices - however, ex vivo techniques require complete kidney washout. Temporary shunts allow for continuous perfusion within physiologic standards, with the main disadvantage of its increased surgery duration, invasiveness, and potential complications such as embolization, haemorrhage, dissection. Extracorporeal techniques are often ideal for complex reconstructions with continuous perfusions, despite its use being limited by its high cost, equipment/training needs and need for perfusionist and pump oxygenator.6 - 9 Despite these various methods for renal protection, no procedure has been clearly considered the therapeutic gold standard. Choice of technique depends on anatomic considerations and should be selected for each patient based on preoperative examination and surgery planning.
Endovascular repair is currently the mainstay treatment for aortoiliac aneurysmal disease in general. For patients with concomitant ectopic kidney, an increasing number of reports refer to endovascular repair. These may range from straightforward repairs to complex ones. New endovascular techniques and customised stent graft availability have expanded the treatment range, and may be particularly suited for patients considered at high risk for OR. Such patients, previously considered unfit for OR or whose anatomy was incompatible with extensive and complex reconstructions, may now be eligible for aneurysm repair.
A 2009 report from Morales et al. exposes the complexity of some of these repairs. It concerns a congenital left pelvic kidney in association with a type IV thoraco-abdominal aortic aneurysm, left common iliac aneurysm (CIA) and left internal iliac aneurysm (IIA). Treatment initially involved embolization of the lower pole of a right renal artery and right internal iliac artery. Customised fenestrated stent graft incorporated the superior mesenteric artery and right renal artery. The pelvic kidney’s artery was maintained using a fenestration at the distal level of the bifurcated graft. Stent grafts were then used to branch into the left internal iliac artery to exclude the CIA and IIA.10
The minimal invasiveness of endovascular repair allows its use in aged or frail patients unfit for OR. A 2018 report from Massoni et al. perfectly illustrates this - an endovascular repair of an 11cm ruptured AAA in a patient with congenital fused pelvic kidney (with 3 renal arteries). The treatment comprised an aorto-uni-iliac endograft, occluder device and a femorofemoral crossover bypass. This allowed for the patency of 2 out of 3 renal arteries without any major renal impairments.11
There are also reports of hybrid repair, including one of an aortoiliac aneurysm associated with pelvic kidney treated by staged hybrid approach using total renal revascularization with an ileorenal bypass, unilateral internal iliac artery (IIA) coil embolization, and subsequent EVAR.12
The authors of this manuscript have recently published a paper reporting the use of iliac branch devices (IBD) for exclusion of bilateral common iliac aneurysms in a patient with a congenital pelvic kidney. Inadequate distal landing zones required the isolated use of IBDs for proper sealing (Figure)13 while maintaining kidney’s vasculature.
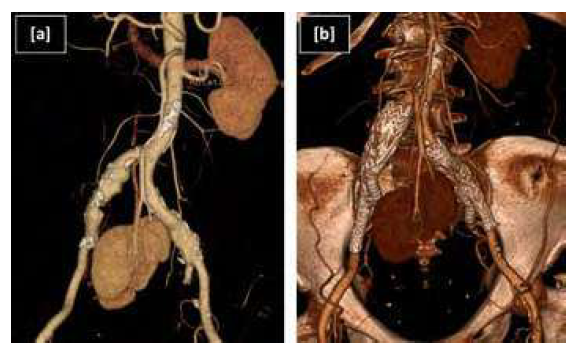
Figure: Iliac branch device for ectopic renal preservation. [a] Pre and [b] postoperative 3D reconstruction CTA of common iliac aneurysms exclusion with bilateral iliac branch devices and preservation of pelvic kidney’s artery.
This brief literature search reveals the natural recent tendency for a rising number of patients being treated with endovascular techniques. Despite the excellent and proven results of OR, unfit patients with complex anatomies may not be eligible for this treatment. The additional anatomical complexity in ectopic kidneys promotes inventive solutions using new endovascular devices and techniques for proper aneurysm exclusion.
Discussion
Ectopic kidney is a congenital anomaly that is rarely found in association with aortoiliac aneurysmal disease. When indicated, aneurysm treatment is additionally challenging since it is vital to preserve and maintain the ectopic kidney’s arterial supply. Historically, OR was the treatment of choice. However, in parallel to standard AAA repair, it is expected that a growing number of patients will be treated with endovascular techniques, and this may rapidly become the treatment of choice for this rare patient group.

