











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
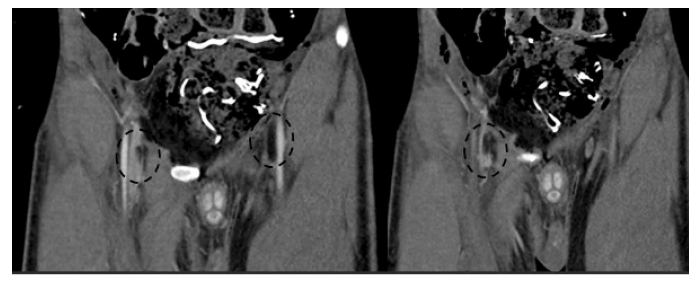
Polytraumatized after a 10-meter fall, which resulted in multiple fractures, including the right femur and pelvis. A 24-hour thoracoabdominal-pelvic computed tomography showed non-occlusive fat embolism in both femoral veins, with a length of 1.7cm on the right and 3.7cm on the left. This diagnosis was based on the identification of emboli with fat-like density. He was treated with elastic compression (18mmHg) with no evidence of pulmonary embolism. Placement of an inferior vena cava filter was not considered necessary given the lack of evidence. Anticoagulation was contraindicated in view of trauma plus hemothorax and grade IV hepatic lacerations.
Fat embolism is rarely diagnosed. Asymptomatic in the hyperacute phase, can trigger a syndrome characterized by respiratory distress, neurological symptoms and petechiae. In bone fractures, the bone marrow accesses small adjacent venules, developing systemic inflammatory reaction and widespread platelet aggregation, typically 24-72h after the embolism.

