











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
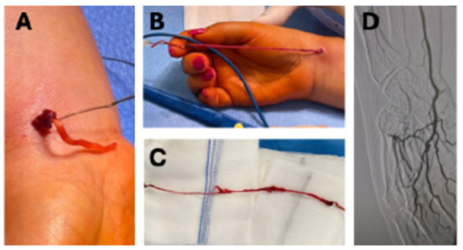
A 64-year-old woman with a history of severe aortic valve stenosis was admitted electively for diagnostic coronary angiography1. A right radial access was selected. Upon progression of a 0.035 PTFE coated guidewire, wire retention was noted. The wire tip was located 4cm below the elbow. After numerous endovascular attempts at wire retrieval, partial extrusion of the radial artery was noted through the orifice of puncture (panel A), suggesting avulsion of the distal segment of the artery.
Surgical exploration was decided. Under axillary nerve block, the guidewire was extracted, bringing along the entire radial artery as in an inversion venous stripping procedure (panels B and C). There were no signs of acute bleeding or hematoma formation. Exploration of the umeral bifurcation was performed, which confirmed the avulsion of the radial artery since its origin and integrity of the ulnar artery. Ligation of the proximal end of the radial artery was performed, and intra-operative angiography revealed good permeability of the ulnar artery, palmar arch and digital arteries (panel D). The post-operative course was uneventful, and the patient was discharged after 24h without symptoms or signs of hand ischaemia.

