











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Subintimal angioplasty, also known as percutaneous intentional extraluminal recanalisation, was first described by Bolia et al. in the United Kingdom in 1989, following an endovascular procedure in which a subintimal channel was accidentally created to cross a popliteal arterial occlusion.1) This endovascular technique allows crossing more complex and calcified arterial lesions, augmenting the endovascular treatment range. During endovascular treatment, the guidewire typically follows the least-resistant pathway. In more calcified and complex lesions, the least calcified path is frequently between the media and intima layer of the arterial wall. When a subintimal track is established, re-entry in the true lumen is required to appropriately treat the arterial lesion. Re-entry of the guide wire may not occur spontaneously. When this happens, adjuvant techniques can be applied, as re-entry devices and retrograde popliteal or tibio-peroneal puncture.2 Although widely used, the impact of subintimal crossing (vs. intraluminal) on endovascular treatment outcomes is not well studied or documented. This study aims to evaluate and compare the outcomes after subintimal and intra-luminal angioplasty for femoropopliteal arterial lesions.
Methods
The authors designed a retrospective, single-centre, comparative study. The population included all patients with peripheral arterial disease (PAD) who underwent endovascular treatment (EVT) by a single operator as a native lesion revascularisation procedure for femoro-popliteal lesions from January 2023 to February 2025. Patient data, procedural details, and outcomes were collected from medical records. Disease extent was staged according to GLASS (Global Limb Anatomical Staging System) after digital subtraction angiography (DSA). The authors subjectively determined the cross-lesion pathway during the procedure by perceiving resistance during guide-wire handling and by visualising the behaviour of the guide-wire tip. According to the cross-lesion pathway, patients were grouped into the subintimal (S) and intraluminal (L) groups. Both groups were compared with respect to the pattern of atherosclerotic disease. The authors also analysed calcification severity of the lesions and EVT technical details, as well as the definitive treatment modality (plain old balloon angioplasty [POBA], drug-coated balloon [DBC] or bare metal stent [BMS]), primary arterial access, and closure technique. Calcification severity was staged according to the classification reported by Araújo et al., Table 1.3
Endpoints include freedom from major amputation (defined as any above-ankle amputation) and reinterventions to address/restore patency of the index limb femoropopliteal arterial segment.
After the procedure, all patients were maintained on acetylsalicylic acid 100 mg once daily. Patients treated with a drug-coated balloon or bailout stenting additionally received clopidogrel 75 mg once daily for a period of 3 to 6 months. Clinical evaluation was the primary postoperative follow-up approach. Arterial Doppler ultrasound was performed in patients with recurrent symptoms or worsening/non-healing trophic lesions to assess revascularisation patency.
Quantitative variables are expressed as mean ± standard deviation (SD) or as median (interquartile range [IQR]), as appropriate. Qualitative variables are expressed as absolute values and percentages. Shapiro-Wilk normative tests were used to assess the distribution pattern in quantitative variables. Student’s t-test, one-way ANOVA and the respective non-parametric tests and χ 2 test were used on univariable analysis. Kaplan-Meier estimates were created to assess the effect of calcification severity on rates of reintervention, amputation, and overall survival, and groups were compared using the Log-Rank test. A p-value of < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS software (version 26.0; SPSS, Chicago, IL, USA).
Results
The study included 95 patients, of whom 10% (n = 9) presented with intermittent claudication, 25% (n = 24) with rest pain and 64% (n = 61) with ulcers or gangrene in the foot. The S group included 30% (n = 28) of the patients, and the L group included 70% (n = 67). The median follow-up time was nine months. Baseline characteristics are described in Table 2.
The median femoro-popliteal GLASS classification was stage 4 in both groups. However, there was a statistically significant difference in GLASS staging between groups, with stage 4 being more common in the S group (p = 0.004). Moreover, the S group included more lesions classified as severe calcification (57% in S group vs 15% in L group; p < 0.001).
Regarding the study endpoints, there were no statistically significant differences in reintervention rates (p = 0.95). During the follow-up period, two patients in the S group and four patients in the L group required reintervention. All reinterventions occurred in the first 12 months of follow-up. Kaplan-Meier estimates for reintervention in the S and L groups were 10.5 ± 7% and 5.7 ± 3% at six months and 10.5±7% and 11±5% at 12 months, respectively, p = 0.95, Figure 1.
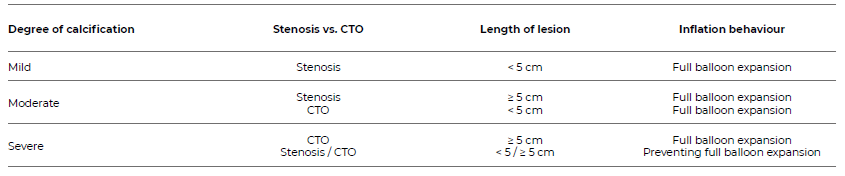
Table 2 Baseline demographic and morphological characteristics of patients with femoro-popliteal lesions treated with endovascular repair, stratified by group.
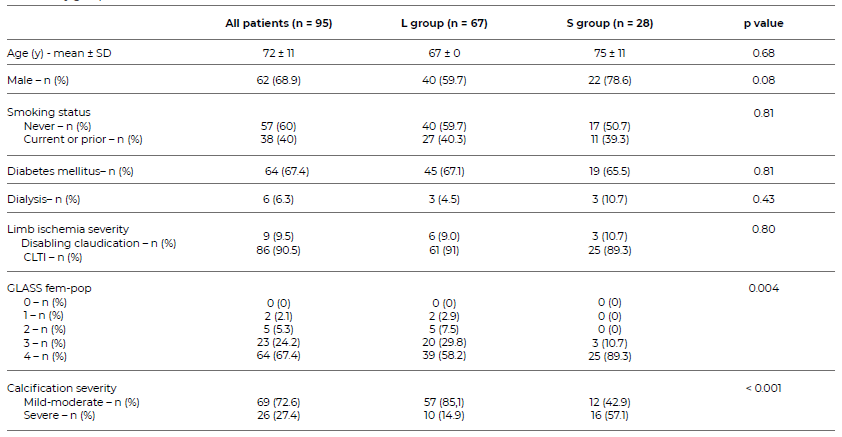
SD: standard deviation; CLTI: Chronic limb threatening ischaemia; GLASS: Global Limb Anatomical Staging System
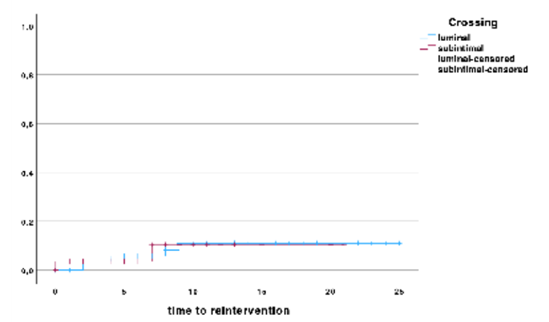
Figure 1 Kaplan-Meier curve for time to reintervention, comparing patients with subintimal or intraluminal lesion crossing
Also, there were no statistically significant differences in amputation rates between groups (p = 0.26). During the follow-up period, there were three major amputations in the S group and two in the L group, all occurring within the first six months of follow-up. Amputation rates in the S group and the L group were 12.2 ± 7% and 4.6 ± 3% at 12 months (p = 0.86), Figure 2. Regarding the technical details of EVT, statistically significant differences were identified for primary access used and the definitive treatment strategy, table 3.
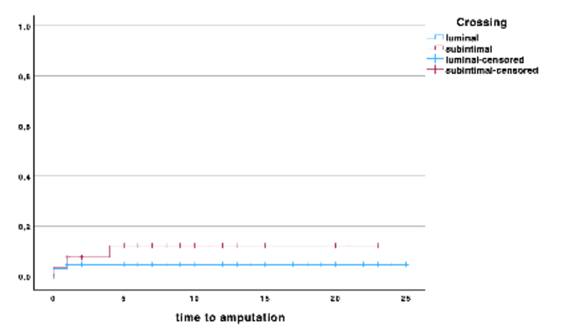
Figure 2 Kaplan-meier curve for time to amputation, comparing patients with subintimal or intraluminal lesion crossing
Table 3 Technical details of endovascular treatment of patients with femoro-popliteal lesions, stratified by group.
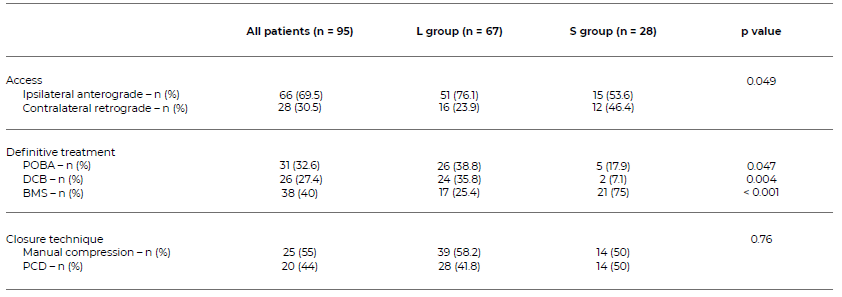
POBA: plain old balloon angioplasty; DCB: drug-coated balloon; BMS: bare metal stent; PCD: percutaneous closure device
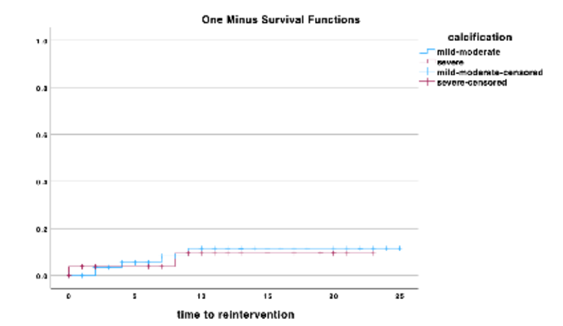
In terms of primary access, 46.4% (n = 12) of patients in the S group required contralateral retrograde access, which was significantly higher than the L group, where only 23.9% (n = 16) needed contralateral retrograde puncture (p = 0.049). Arterial calcification did not influence freedom from reinterventions, Figure 3. Relatively to the definitive treatment strategy, DEB was more frequently used in L group (p = 0.004) and bailout stenting in s group (p < 0.001). POBA was the definitive treatment modality in 17.9% (n = 5) patients in S group and 38.8% (n = 21) in L group (p = 0.47), while deb was used for 7.1% (n = 2) and 35.8% (n = 26) of the patients in S and L group, respectively (p = 0.004). 75% (n = 21) of the patients in s group and 25.4% (n = 17) in L group required bailout stenting (p < 0.001). closure technique did not differ significantly between the two groups (p = 0.76), with similar rates of manual compression and PCD use.
Discussion
With the rapid advancements in EVT techniques, it is essential to continuously update clinical data to ensure patient care aligns with evidence-based medicine.
Despite the widespread use of the subintimal approach for crossing complex arterial lesions, data on its use in this anatomical territory and its impact on patient outcomes remain limited.4 This knowledge gap prompted the authors to conduct the present retrospective cohort study.
To classify calcification severity, the authors use the classification system proposed by our group and previously published.3 This classification system integrates femoro-popliteal degree of calcification and also technical factors that may influence target-lesion treatment patency.
Regarding the femoro-popliteal GLASS classification, it’s important to note that there was a statistically significant difference between groups, despite an equivalent median class, with subintimal crossing being more frequently required in more complex lesions. Moreover, this pathway was more commonly required in more calcified lesions. These results suggest that, when treating complex and calcified lesions, subintimal guidewire tracking is more likely to cross the lesion and allow adequate treatment.
In our cohort, an antegrade approach was preferred. When intraluminal crossing was unsuccessful, the subintimal tracking and re-entry (STAR) technique was attempted, followed by retrograde puncture and other re-entry techniques, such as controlled antegrade and retrograde tracking (CART), reverse-CART, or double-balloon, when necessary. Reentry devices were rarely used.
The results of this study suggest that subintimal crossing does not negatively impact reintervention or amputation rates. These findings support the use of this technique when intraluminal crossing is not feasible, providing greater confidence that the subintimal guidewire pathway does not adversely affect patient outcomes. This may justify lowering the threshold for adopting the subintimal pathway in more complex and heavily calcified lesions.
Another factor not assessed in this study that may have contributed to the absence of significant differences between the groups is vessel preparation before the definitive treatment. In the authors’ opinion, meticulous vessel preparation plays a more critical role in determining outcomes following EVT of femoropopliteal arterial lesions than the lesion-crossing pathway.
Although no correlations were found between the subintimal pathway and patient outcomes, this technique was more frequently associated with some technical details. The association between contralateral retrograde puncture and subintimal lesion crossing can be explained by the correlation between lesion complexity and calcification severity - factors previously noted by the authors as being associated with the subintimal approach - and their frequent presence in more proximal locations, such as the common femoral artery or ostial superficial femoral artery. In these cases, anterograde ipsilateral puncture may be unsafe, making contralateral access the preferred approach.5
Regarding stent deployment, a bail-out strategy was adopted, with stenting performed in cases of flow-limiting dissection or significant residual stenosis (>30%). Our findings indicate that subintimal tracking was more frequently associated with bail-out stenting. This can be explained by the dissection plane created by the guidewire during subintimal crossing, which is more commonly associated with flow-limiting dissections. However, this aspect did not translate into any negative impact on patient outcomes.
This study has several limitations to note. It is a single-centre retrospective study, which inherently has unavoidable bias. Also, the small sample size may contribute to type 2 statistical errors. Also, the source data depends on appropriate medical records and clinical follow-up, which limits the available morphological data. Finally, the selection of vascular procedures depends solely on a single surgeon’s experience, potentially limiting generalizability. In this study, we included only patients who underwent EVT by a single operator to standardise procedural techniques and restricted the analysis to those treated in the past two years to minimise variability from evolving surgical techniques.
Conclusion
The results of this study suggest that subintimal angioplasty yields clinical outcomes comparable to those of intraluminal angioplasty in the treatment of femoro-popliteal lesions, particularly with respect to limb preservation and reintervention rates. While the subintimal approach was associated with a higher bailout stenting rate, it nonetheless demonstrated a similar efficacy and safety profile. We found that the subintimal pathway was used more frequently to cross more complex and calcified lesions. These findings highlight the utility of the subintimal technique as a reliable alternative, especially when intraluminal crossing is not feasible for this group of lesions. As such, the data support a more liberal use of the subintimal pathway in complex lesion subsets, reinforcing its role as an effective and safe strategy within the endovascular treatment armamentarium.

