











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Background
Popliteal Artery Entrapment Syndrome (PAES) is an uncommon but important cause of lower-limb ischaemia, particularly affecting young, active individuals without traditional risk factors for peripheral artery disease. PAES is rare, with an estimated prevalence of 0.17 - 3.5% in the general population. Among patients under 40 years of age with claudication and no atherosclerotic risk factors, PAES accounts for approximately 3 - 5% of cases.1,2 The condition predominantly affects males (ratio 15: 1), particularly military personnel and athletes.2,3
PAES was first described by Anderson Stuart in 1879 as an anatomical abnormality during cadaveric dissection. However, the first successful operative decompression was not performed until 1959 by Hamming and Vink, marking a significant advancement in the management of this condition.4 PAES results from an abnormal anatomical relationship between the popliteal artery and surrounding structures, such as muscles or tendons, causing compression and intermittent claudication. If not diagnosed early, chronic compression can lead to serious vascular complications, including thrombosis or arterial occlusion.1,5 Levien and Veller reported prevalence rates of up to 15% in asymptomatic individuals following targeted screening, suggesting the condition may be underdiagnosed in clinical practice.6
This case report discusses a 36-year-old patient with type 3 PAES who presented with severe claudication and underwent successful surgical management.
Case Report
A 36-year-old previously healthy male presented to the outpatient vascular clinic with right lower-limb claudication. He reported walking less than 100 metres due to pain, which significantly impaired his quality of life (Rutherford grade 3). He had no history of smoking, hypertension, diabetes, or other cardiovascular risk factors.
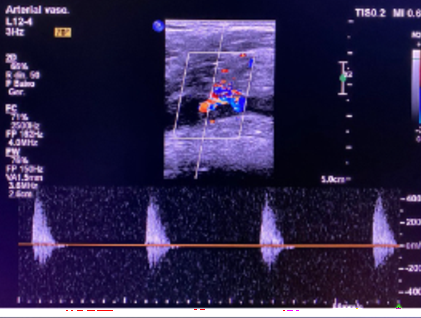
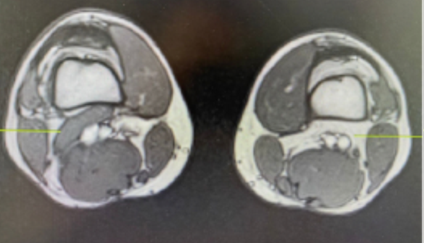
On physical examination, his right distal pulses were absent, whereas the contralateral limb had palpable pulses. Doppler ultrasound showed a peak systolic velocity (PSV) of 400 cm/s in the right popliteal artery, corresponding to 90 - 99% stenosis, Figure 1.7 Given the absence of atherosclerotic risk factors and his young age, magnetic resonance angiography (MRA) was performed, Figure 2. This confirmed a diagnosis of type 3 PAES with sub-occlusive stenosis of the popliteal artery.3
After a detailed discussion of treatment options, the patient chose surgical intervention. The surgery comprised myotomy of the lateral accessory head of the medial gastrocnemius muscle, which was compressing the popliteal artery, and an interposition graft of the popliteal artery from P1 to P3 using a contralateral inverted great saphenous vein (GSV). The procedure was performed via a posterior popliteal approach.8,9
Postoperatively, the patient recovered uneventfully. His right lower limb distal pulses were restored, and follow-up examinations confirmed the graft's patency. One year after surgery, the patient remained symptom-free with preserved distal pulses.1
Discussion
PAES is a rare but well-documented cause of claudication in young, active individuals, typically without atherosclerotic risk factors. It can be difficult to diagnose because of its rarity and overlap with other causes of leg pain, such as chronic exertional compartment syndrome.2,10 In this case, the absence of traditional cardiovascular risk factors and the patient's age raised suspicion of PAES, prompting further diagnostic imaging that confirmed the diagnosis.
Classification and prevalence
There are six types of PAES, classified by the anatomical relationship between the popliteal artery and surrounding structures. Type 3 PAES, as observed in our patient, accounts for approximately 35% of all PAES cases.3
Diagnostic approach
Early diagnosis is crucial to prevent complications such as thrombosis, aneurysm formation, or irreversible ischaemia.2 Non-invasive imaging techniques, such as Doppler ultrasound and MRA, are valuable for assessing the extent of vascular compression and guiding treatment.7
Table 1 Classification of popliteal artery entrapment syndrome
| Type | Prevalence | Anatomical characteristic |
|---|---|---|
| I | 30% | Medial deviation of popliteal artery, normal medial gastrocnemius |
| II | 25% | Lateral insertion of medial gastrocnemius head |
| III | 35% | Accessory slip of gastrocnemius compressing popliteal artery |
| IV | 7% | Popliteal artery passes deep to popliteus muscle or fibrous brands |
| V | <2% | Any combination of types I-IV with concurrent venous compression |
| VI | ~1% | Functional entrapment with normal anatomy but compression during muscle contraction |
Treatment options
Surgical intervention is the preferred treatment for symptomatic PAES. Revascularisation via a posterior approach with the patient in the prone position provides optimal access to the artery and adjacent structures in the popliteal fossa, facilitating accurate diagnosis and targeted release of the popliteal artery. This approach also allows the use of a suitable saphenous vein as an interposition graft, maximising the effectiveness of revascularisation and supporting excellent long-term outcomes.2,5,10 Autologous vein grafts are often preferred for their superior long-term patency compared with synthetic grafts.8
In cases presenting with acute thrombosis, thrombolytic therapy serves as an important adjunctive treatment that may permit less extensive surgical procedures. Studies have demonstrated successful restoration of patency in 75 - 85% of acutely thrombosed arteries prior to definitive surgical intervention.2
It is important to note that while thrombolysis may successfully restore patency, it does not obviate the need for definitive surgical correction of the underlying anatomical abnormality. Without addressing the causative compression, recurrent thrombosis is likely.2
The posterior approach used in this case offers several advantages, including direct visualisation of the neurovascular bundle and surrounding musculature, easier identification of aberrant muscular attachments, and superior exposure for arterial reconstruction when required.9 Long-term outcomes for both medial and posterior approaches are comparable, with patency rates exceeding 90% at 5 years when performed by experienced vascular surgeons.9
Bilateral involvement
PAES is frequently bilateral. More recent series report bilateral involvement in 30 - 67% of cases, underscoring the importance of comprehensive assessment.3 Screening of the contralateral limb is strongly recommended, even in unilateral presentations such as in our patient, as asymptomatic compression may be present. Early detection allows prophylactic intervention before arterial damage occurs. In our case, the patient underwent bilateral lower-limb examination and contralateral limb imaging, which revealed normal anatomy and flow dynamics, ruling out asymptomatic contralateral involvement. This thorough approach aligns with current best practice recommendations.1
Long-term outcomes
The patient’s uneventful recovery and the maintenance of distal pulses throughout a one-year follow-up period highlight the effectiveness of surgical intervention. Delayed treatment could have led to more severe complications, underscoring the importance of early recognition and prompt intervention.2,3
Follow-up studies demonstrate that properly treated patients can typically resume previous physical activities without sequelae.2 Even high-performance athletes have successfully returned to competitive sports following appropriate surgical intervention, though a graduated return to activity protocol is recommended.2
This case report highlights the importance of considering PAES as a differential diagnosis in young patients presenting with claudication, particularly when atherosclerotic risk factors are absent. The case underscores the need for a thorough diagnostic workup, including imaging such as Doppler ultrasound and MRA, to ensure early detection and prevent potentially severe complications such as thrombosis or irreversible ischaemia. The successful surgical management of this patient, involving myotomy and vascular reconstruction with an interposition graft, demonstrates that timely intervention can lead to excellent functional outcomes.
The restoration of distal pulses and the patient’s symptom-free status after one year reflect the effectiveness of this approach. Beyond its clinical implications, this case emphasises the broader need for heightened awareness of PAES among healthcare providers. Early recognition and intervention not only improve individual patient outcomes but also help reduce the long-term burden of undiagnosed vascular disease. This case ultimately demonstrates that with appropriate diagnostic tools and timely surgical intervention, PAES can be effectively managed, enabling patients to return to their normal activities and achieve an excellent quality of life.

