











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Background
Around 40 - 60% of abdominal aortic aneurysm (AAA) patients are deemed ineligible for standard endovascular aneurysm repair (EVAR) because of hostile anatomy.1 While the precise definition remains a subject of ongoing debate, the clinical significance of hostile neck anatomy is well recognised. A systematic review and meta-analysis by Stather et al., focusing on the outcomes of EVAR in patients with hostile anatomy - defined, in this study, by the presence of neck length < 15 mm, neck diameter > 28 mm, or angulation > 60º - revealed a significant increase in intra-operative complications and type Ia endoleaks.2 Moreover, many cases exhibit multiple anatomical features that collectively and exponentially increase the risk of both immediate and long-term procedural complications.
Short and angulated necks pose a serious risk of type Ia endoleak due to the difficulty in achieving proper proximal fixation and endograft seal, compromising both the stability of the endograft at its initial deployment site and the effective exclusion of blood flow from the aneurysm sac.3
Recognition of the challenges posed by suboptimal neck anatomy in EVAR has driven the development of novel endografts and adjunctive techniques, primarily aimed at improving graft fixation and sealing. Custom-made stent grafts, such as fenestrated and branched devices, extend the proximal seal zone, enabling secure proximal fixation, effective sealing above the aneurysm sac, and maintenance of perfusion to vital branch vessels.3 Among adjunctive techniques, endoanchors (Medtronic®) were developed as fixation devices to mechanically secure the endograft to the aortic wall. By replicating the function of surgical sutures, they provide active fixation and reinforce proximal sealing, thereby reducing the risk of stent graft migration and Type Ia endoleaks.3 Increasing recognition by device manufacturers of the limitations posed by complex proximal neck anatomy has been instrumental in the development of newer stent grafts designed for hostile necks, often with less restrictive instructions for use (IFU). Concurrently, innovative graft deployment methods and techniques have been introduced and increasingly reported in the literature, supporting broader patient selection criteria for EVAR.
In this case report, we aim to present a case report using a previously described technique that allows a more aggressive deployment of the Endurant II (Medtronic, Santa Rosa, Calif) stent graft for short and angulated necks.
Case Report
A 72-year-old male with a history of dyslipidaemia and smoking was admitted to the vascular ward with a large AAA, measuring 85 mm in maximum diameter. The patient had recently undergone an uneventful recovery following a Hartmann procedure, performed for a transmural ischemic colitis. The anatomical features of the aneurysm were suboptimal for EVAR, specifically a short neck (approximately 13 mm) and an infrarenal angulation of 90°, Figure 1.
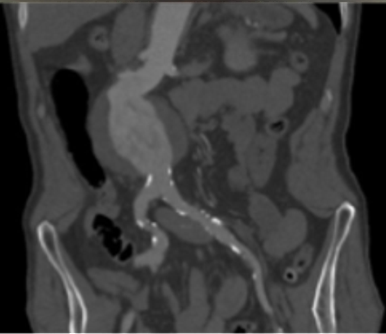
An infrarenal abdominal aorta aneurysm with a maximum diameter of 85 mm is evident, with a short neck and severe infrarenal angulation.
However, considering the recent colonic intervention, open surgical repair was considered inappropriate, and hence, we proceeded with an endovascular exclusion of the aneurysm.
The Endurant II stent graft (Medtronic, Santa Rosa, Calif) was deployed using the reverse slider technique, Figure 2.4 This was performed in the following steps:
Deployment the first stent of the main body by rotating the external slider in the usual manner (larger main front deployment wheel).
Rotation the back-end wheel slightly to loosen the captured suprarenal stent.
Slow rotation the external slider one and one-half to two times in reverse to raise the outer sheath until there is resistance and rotation of the external slider in a counterclockwise direction, to return the outer sheath to its natural position.
Deployment of the main body until the second stent and repetition of steps 2 and 3 until the edge of the stent graft expands, which is visible on the fluoroscope. By repeating these steps slowly, the top edge of the graft fabric expands increasingly. These steps help the graft fabric edge come into contact with, or be positioned close to, the aortic wall by deploying only two or three stents without unfastening the suprarenal stent.
Release the suprarenal stent.
The remainder of the procedure followed the standard techniques, and the completion of angiographic images confirmed successful exclusion of the aneurysm with accurate fixation on the proximal point, Figure 3. The post-operative course was uneventful, and the patient was discharged home after three days.
A CTA performed one month after the procedure revealed correct endograft positioning with no evidence of endoleak, Figure 4.
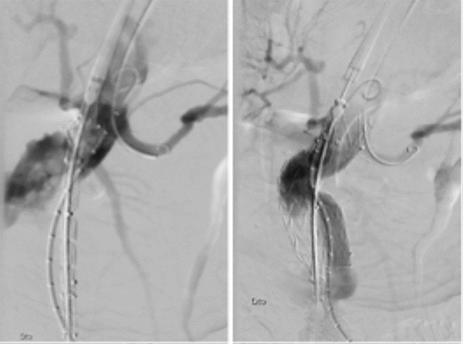
Figure 2 Intra-operative fluoroscopy images demonstrating the proximal deployment of the Endurant II stent graft, using the reverse slider technique

Complete exclusion of the aneurysm and no evidence of endoleak are observed. Na accurate proximal fixation point was also achieved.
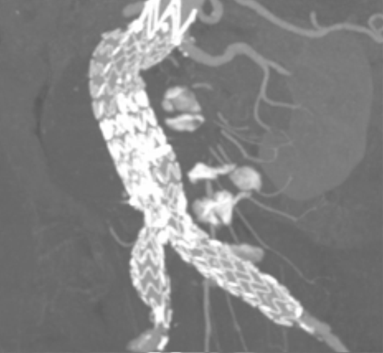
Figure 4 Computed tomography angiography one month after the procedure (multiple intensity projection, coronal view)
Correct positioning of the endograft with no evidence of endoleak are noted.
Discussion
Hostile proximal neck anatomy remains the most significant impediment to successful EVAR.5 The reverse slider technique allows proximal sealing in short and angulated neck aneurysms. It was developed by Morikage et al. and published in 2019.4 In summary, the reverse slider technique involves the repeated rotation of the external slider in the reverse direction, accompanied by gradual deployment of the suprarenal stent, allowing the proximal edge of the endograft to gradually expand, progressively approaching the contralateral side of the aortic wall.
Extreme neck angulation complicates achieving an adequate proximal seal in short necks. This technique ensures a proximal sealing zone on the greater curvature side that resembles that on the lesser curvature.4 In the original study, the reverse slider technique was applied to 34 patients with hostile necks. The six-month follow-up CTA or duplex ultrasound showed no type Ia endoleak and no migration, distal atheroembolization, or stent graft infolding.4
The reverse slider technique represents an alternative for patients whose aneurysm neck anatomy compromises the success of standard deployment methods, by facilitating graft placement orthogonally to the aortic axis, enabling the main body of the graft to deploy in alignment with the aortic angulation. In this case, a satisfactory proximal seal was achieved intraoperatively using the reverse slider technique, as confirmed on early postoperative imaging, thereby hindering the implantation of endoanchors.
Conclusion
Compared with novel endografts and adjunctive techniques for hostile necks, the reverse slider technique is a cost-effective, straightforward alternative for the endovascular treatment of AAA patients with hostile infra-renal aneurysm necks. Furthermore, it does not preclude future interventions if necessary.

