











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Background
Aortic arch aneurysms represent significant treatment challenges due to their complex anatomy and the vital structures they supply. Traditionally, the gold standard for treatment has been open surgical repair, which typically involves a sternotomy, cardiopulmonary bypass, and hypothermic arrest. Although effective, this approach carries significant risks, including a pooled mortality of approximately 5% and a stroke rate of similar magnitude.1 The morbidity and mortality associated with these procedures, particularly in high-risk patients, underscore the need for alternative therapeutic approaches.
Endovascular techniques have evolved as a promising alternative for the management of aortic arch aneurysms, offering the potential to reduce operative mortality and morbidity. Particularly, the development of custom-made endografts with branched designs has been a breakthrough in the treatment of complex aneurysms.2,3 In this report, we describe the case of a 70-year-old male patient with an asymptomatic saccular aortic arch aneurysm, who underwent treatment using a custom-made, three-inner-branched stent graft. The goal of this intervention was to achieve a total endovascular repair, ensuring the exclusion of the aneurysm and the preservation of the upper aortic branches.
Case report
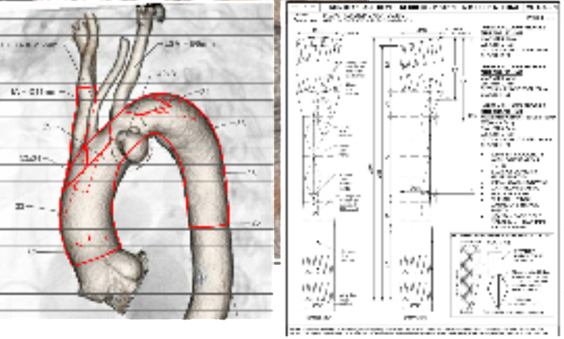
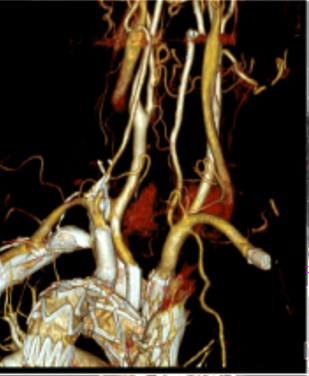
A 70-year-old man with hypertension and dyslipidemia was incidentally diagnosed with an asymptomatic saccular aortic arch aneurysm, Figure 1. Although not considered high-risk based on comorbidities, the patient’s age was taken into account, and after a multidisciplinary discussion with vascular and cardiac surgeons, it was decided to perform a total endovascular arch repair using a custom-made, three-inner-branched stent graft, Figure 2.Percutaneous access to the right femoral, axillary and brachial arteries and the left femoral vein was obtained. Only the left carotid artery was surgically exposed. A bolus of 5,000 units of heparin was administered, followed by monitoring of the activated clotting time.The device was pre-flushed with CO2 before saline infusion to prevent cerebral gas embolisation.A custom-made three-inner branched stent graft (40 mm x 30 mm x 246 mm) was deployed under temporary balloon occlusion of the inferior vena cava. The endograft had two anterograde branches, one for the innominate trunk accessed from the right axillar artery and bridged with an Cook Zenith 12 mm diameter iliac limb and another for the left carotid artery bridged with a Begraft stent 6 mm, while a retrograde branch with a preloaded catheter for the left subclavian artery, accessed from the femoral artery and bridged with Viabhan 10 mm followed by a 10mm Bentley Begraft due to a kink, Figure 3. There were no complications, and the duration of the operation was 3.5 hours. The total fluoroscopy time was 56.2 min, the total radiation dose was 809.9 mGy, and the total iodine contrast volume was 100 mL. The patient was discharged three days postoperatively, without symptoms. A control computed tomography angiography performed three months after the operation demonstrated aneurysm exclusion, the patency of the three supra-aortic branches and absence of cerebral ischemic lesions, Figure 4.
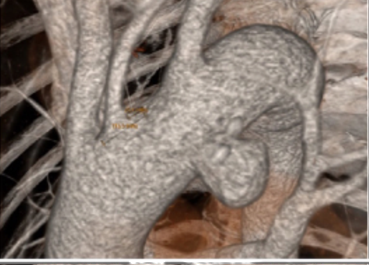
Figure 1 Pre-operative computed tomography angiography 3D reconstruction showing the saccular aneurysm of the aortic arch.
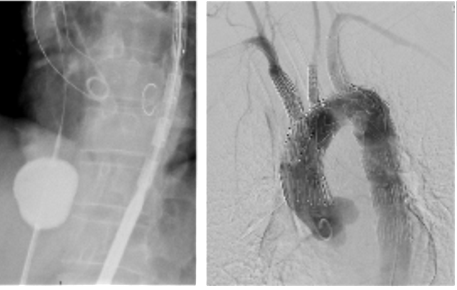
On the left, temporary balloon occlusion of the inferior vena cava is shown; on the right, completion digital subtraction angiography.
Discussion
At our centre, the multidisciplinary aortic team includes vascular surgeons, cardiac surgeons, and anesthesiologists, and there is a monthly multidisciplinary meeting to discuss these cases. In the case herein presented, although the patient was not considered high risk based solely on comorbidities (hypertension and dyslipidemia), the multidisciplinary discussion led to selecting a total endovascular arch repair with a custom-made, three-inner-branched endograft as the primary repair option.
The treatment of aortic arch aneurysms remains a significant challenge due to the complexity of the anatomy and the critical branches arising from the arch. Endovascular repair has become a viable alternative, particularly with the development of branched and fenestrated endografts tailored to individual patient specificities.
Although endovascular aortic arch repair was initially reserved for patients unfit for open surgery, it is now offered to patients with suitable anatomy in high-volume referral centres, even to non-high-risk patients, after discussion in a multidisciplinary team.4 This is in accordance with the increased use of transcatheter treatment of aortic valve stenosis (TAVI) among low-risk patients with severe, symptomatic aortic stenosis. In a randomised noninferiority trial conducted at 38 sites in Germany, Blanckenberg et al. showed that among patients with severe aortic stenosis at low or intermediate surgical risk, TAVI was noninferior to surgical aortic valve replacement with respect to death from any cause or stroke at one year.5
In fact, endovascular aortic arch repair with custom-made branched grafts has been increasingly recognized for its lower risk profile, quicker recovery times, and its ability to avoid the complications inherent in open surgery, inherent to aortic cross-clamping, cardiopulmonary bypass and hypothermic arrest. Also, the addition of a third inner branch to the device design, such as in this case report, avoids the need for extra-anatomic reconstruction using transposition or bypass, allowing a total endovascular aortic arch reconstruction. Frola et al. compared hybrid and total endovascular aortic arch repair at two tertiary vascular surgery centers and reported that total endovascular repair seems to shorten operative times and provide higher clinical success compared with hybrid solutions, without significant 30-day mortality differences.6
Recent studies have further explored the outcomes and advancements in endovascular repair techniques for aortic arch aneurysms, highlighting the promising role of branched endografts in improving patient outcomes. Behdinan et al. published a meta-analysis in which clinical outcomes of total endovascular aortic arch repair in non-emergent adult patients were assessed. Across 23 studies and 1867 patients, technical success was 97.4%, 30-day mortality was 2.7%, and in-hospital stroke rate was 4.3%. No significant outcome differences were found between branched and fenestrated endografts. The early endoleak rate was found to be 6.8% (95% CI, 4.0 - 11.3), and 7.7% (95% CI, 4.0 - 14.5) of patients underwent reintervention within the first 30 postoperative days.7 McCarthy et al. compared elective endovascular stent grafting with open surgical repair for aortic arch and descending thoracic aneurysms and included five comparative cohort studies. Endovascular stent grafting was associated with lower short-term mortality (OR 0.71; 95% CI 0.51-0.98), while open surgery showed better long-term survival and fewer reinterventions.8 It is crucial understanding the long-term viability of endovascular aortic arch repair with customed made branched grafts as ongoing surveillance ensures that complications such as endoleaks or graft failure can be promptly addressed. Also, Lim et al. reported a pilot study in which compared quality of life in patients undergoing branched endograft-based endovascular aortic arch repair versus open surgery. Using the RAND SF-36 questionnaire, early postoperative outcomes favored the endovascular group in terms of physical recovery and general well-being.9
From a technical point of view, during the deployment of the main device, to ensure a very precise deployment, there are different blood pressure-lowering measures that can be employed which include rapid ventricular pacing or right atrial balloon inflow occlusion technique, the latter used in our case. The Munich Valsalva technique is another alternative which consists in closing the adjustable pressure-limiting valve to 25 mmHg during manual mechanical ventilation, creating "manual bloating" of the lungs and sustained apnea. The increased intrathoracic pressure causes compression of the vena cava and pulmonary veins, reducing the venous backflow and gradually decreasing the arterial pressure. Once the desired pressure is obtained, the stentgraft can be accurately deployed. The airway pressure is thereafter slowly reduced, and the patient is taken back to normal ventilation. The procedure is then finished following standard practice.10 Also the risk of cerebral embolization remains a limitation to the endovascular approach, there are several maneuvers to mitigate this risk, including flushing the device with CO2 and sequentially clamping the carotid arteries during catheter manipulations.
In conclusion, the integration of recent advances in endovascular techniques, including the use of custom-made, branched endografts, represents a significant step forward in the treatment of aortic arch aneurysms and the results from recent studies underscore the safety and effectiveness of these approaches. Our case adds to the growing body of evidence supporting the use of total endovascular repair for aortic arch aneurysms even in standard risk patients, if the anatomy is suitable and after discussion in a multidisciplinary team. Reporting of long-term outcomes is necessary to demonstrate the efficacy and durability of branched arch repair.

