











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Background
The imposter phenomenon (IP) was first described in 1978 by Clance and Imes, as ‘an internal experience of intellectual phoniness’1 in successful individuals, like health professionals and students2-3 who, lacking the perception of their high abilities, 4 feel like frauds, and attribute their successes to luck or error rather than accepting the merit of their tasks. 5-6 This affects their career progression and psychological well-being. 7
Initially, IP was identified in high-achieving women, associated with family dynamics from an early age and the stereotypes implemented by the society in which they were inserted.1 Several studies showed that men are also prone to IP. 7-8
The Clance Impostor Phenomenon Scale (CIPS) is a validated specific scale to study IP. A study of the Wisconsin general practice residency in 2004 showed that a third of the residents suffered from IP, with consequent levels of distress, because of feelings of not being competent or intelligent enough to perform the professional role. Females’ prevalence was 41% and males were 24%, and participants with high Clance Impostor Phenomenon Scale (CIPS) scores presented depression, anxiety, and self-esteem issues. 9
The CIPS is related to three principal components analysis (PCA): fake, luck, and discount. 8 However, studies point to the existence of a fourth factor - fear. The fourth factor of the current model is mostly composed of items that translate as ‘fear of failing’, 10 previously affiliated with the factor ‘FAKE’.10 Although the 3-factor model is more widely used, the 4-factor model is better balanced and efficient in factorial composition. 10
IP is related to mental health problems, namely distress, anxiety, depression, burnout, frustration, and low self-esteem. 1,3,11 A study showed that ‘in residents, the prevalence of depression or depressive symptoms is estimated to be 28.8% worldwide’. 11
To screen and verify the levels of psychological distress, a measure of sufferance, simple, short, reliable, and validated instruments, like the Patient Health Questionnaire-4 (PHQ-4), can be used, to attempt to increase mental health. 12-14
This study aimed to assess the prevalence of the IP in general practice/family medicine residency in the Central region of Portugal in 2022, by gender, year of residency (1st-4th year), and satisfaction with the curricular average mark. Additionally, we assessed its correlation with distress, anxiety, or depression.
Methods
A cross-sectional observational and correlational study was carried out in the Central region of Portugal in 2022. The studied population was the 495 general practice/family medicine residents in this region. With a confidence interval of 95% and an error of 10%, a sample of 83 participants was calculated.
An online questionnaire was applied. Data was collected between January and September 2022 (several reminders have been sent). The questionnaire was designed in Google-forms ® (Annex IV). Only 1 answer per person was admitted. The anonymity of all participants was ensured. CIPS and PHQ-4 scales, and variables such as gender, year of residency, satisfaction with residency mean mark, and the last three digits of the participants’ cell phone numbers were requested to prevent repetition of responses.
To be considered for data analysis, participants had to complete the entire questionnaire, including all the variables, the PHQ-4 scale, and the CIPS. Participants who chose not to complete the full questionnaire were excluded from the data analysis.
Besides the context of personal information two questionnaires were applied:
CIPS. To detect the presence of IP, the Clance Impostor Phenomenon Scale (CIPS) has been the reference instrument since 1985. 15 It is a 20-item measurement instrument on a Likert scale of 1 (not at all true); 2 (rarely); 3 (sometimes); 4 (often); 5 (very true). The total scale ranges from values 20-100 and depending on the final test score, the individual will be categorized into one of the following IP categories: few Impostor characteristics (if the total score is 40 or less); moderate IP experiences (if the score is between 41 and 60); frequent Impostor feelings (for a score between 61 and 80) and intense IP experiences (for a score higher than 80). 10-11 ‘The higher the score, the more frequently and seriously the IP interferes in a person’s life’. 15
PHQ-4. To assess the participants’ level of distress, we used The Patient Health Questionnaire-4 (PHQ-4). PHQ-4 is a combination of two scales: Patient Health Questionnaire-2 (PHQ-2) with two items about depression; and Generalized Anxiety Disorder (GAD-2) with two items related to anxiety. 12-14 Results from the junction of PHQ-2 and GAD-2, 12 consists of four questions measured on a scale of 0-12, for the last 14 days, responses being scored as: 0 - not at all; 1 - several days; 2 - more than half the days; 3 - nearly every day the obtained answers place the individual in one of four categories, referring to the level of anxiety and depression: normal (0-2), mild (3-5), moderate (6-8), severe (9-12).
The representative sample size was calculated for a confidence interval of 95% and an error margin of 10%, as of n=76.
A full response to both CIPS and PHQ4 was mandatory as inclusion criteria.
After data collection, descriptive and inferential statistics were performed to analyze data. Parametric for normal distribution data and nonparametric for non-normal distribution data or ordinal variables was performed, using the 27th edition of the IBM Statistical Package for the Social Sciences (SPSS) Statistics®, setting a p-value of <0.05 for statistical significance.
The Kolmogorov-Smirnov test was used to verify if numeric data had a normal distribution. The Mann-Whitney U test was used to study IP differences between residents according to gender and satisfaction with residency mean mark. The Kruskal-Wallis test was used to assess differences in the prevalence of IP by year of residency. Spearman’s correlation was used to assess the relationship between IP and distress.
This study was approved by the Ethics Committee of ARS Centro (Annex I), the author of the CIPS scale au-thorized its use (Annex II) and the participation of the residents was authorized by the Coordinator of the Residency in General Practice/Family Medicine of the Center Region (Annex III).
Results
Although the total sample was 89 participants, the study was conducted with 62 participants fulfilling the inclusion criteria.
According to Table 1, n=62 questionnaires were included for data analysis. For this sample, 80% were female (n=40), 30.6% (n=19) were attending the 1st-year of residency, 24% (n=13) in the 2nd-year, 11% (n=17) the 3rd-year and 27% (n=17) the 4th-year.
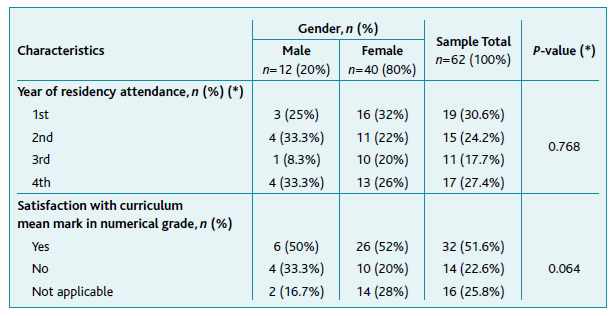
For 51.6% of the sample, there was satisfaction with the curriculum mark, women, not significantly, p=0.064, more satisfied n=39 (81.3%). Of those who were not satisfied, 87.5% (n=14) were women. No difference was found by gender for the year of residency (p=0.768).
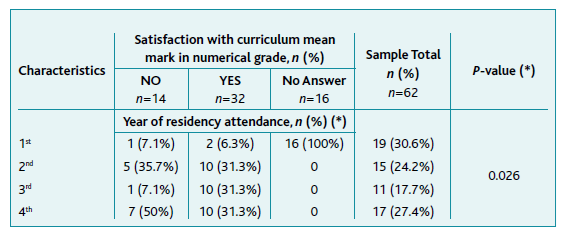
The analysis of satisfaction with the curriculum average numerical mark and year of residency showed that 1st-year respondents scarcely responded and that 2nd, 3rd, and 4th-year ones were more satisfied (p=0.026), as shown in Table 2. For 33,3% of the 2nd-year residents, 10% of the 3rd-year, and 70% of the 4th-year ones there was no satisfaction with such numerical mark.
Kolmogorov-Smirnov tests revealed a non-normal distribution for HQ-4 and CIPS scores (p=0.001 and p=0.030, respectively), and non-parametric tests were applied. The Spearman’s correlation between PHQ-4 and CIPS was very weak and not significant (ρ=0.085, p=0.511). The same was seen for the classes of distress (PHQ4) and IP (ρ=0.050, p=0.701).
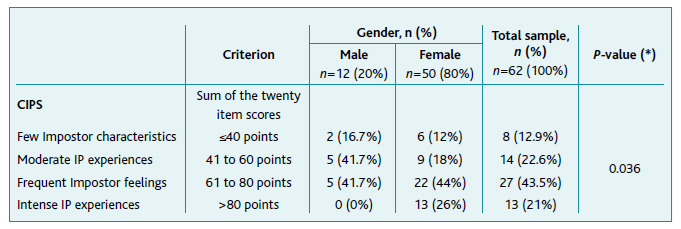
Statistically significant differences were observed between genders for the CIPS class (p=0.036), revealing Frequent Impostor feelings and intense IP experience levels significantly more frequent in females (Table 3).
As shown in Table 4, the analysis by residents’ gender of PHQ-4 global score (p=0.640), distress class (p=0.696), and CIPS global score (p=0.059) was not significantly different. However, a gender difference was verified by CIPS categories, p=0.036.
Table 4 Significance (p) of nonparametric tests between the epidemiologic variables and the classes PHQ-4, distress, CIPS

No significant differences were observed in the PHQ-4 global score (p=0.598), distress class (p=0.625), CIPS global score (p=0.085), and CIPS class (p=0.131) according to year of residency.
As a function of satisfaction with curriculum mean mark and considering only 2nd to 4th-year residents (n=43), there were significant differences in the CIPS global score (p=0.043) and no significant differences in the PHQ-4 global score (p=0.685), distress class (p=0.690), and CIPS class (p=0.088).
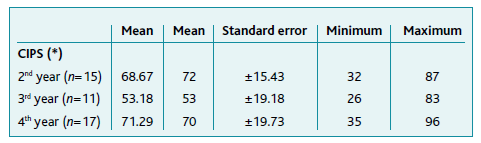
Table 5 shows that the average score is the lowest (53.18) in the overall CIPS score for the 3rd-year residents, and half of these are positioned between 26 and 53 (moderate IP experience); 2nd and 4th-year residents have close average scores (68.67 and 71.29, respectively) and half of each group showed frequent IP feelings level (between 72 and 87 and between 70 and 96, respectively). No responses were obtained from 1st-year residents.
Since significant differences were found for the total CIPS class for gender and CIPS score for the year of residency, the four CIPS factors - discount, luck, fake, and fear - were studied. The Kolmogorov-Smirnov test revealed non-normality for the numerical scores of all four factors of CIPS. Table 6 shows no significant differences in any of the four factors scores regarding gender, year of residency, and satisfaction with mean curricular mark.

Discussion
This study was conducted to detect the prevalence of IP among residents from Central Portugal and ascertain if it is related to the level of distress, gender, year of residency, and satisfaction with the mean curricular mark.
Eighty-nine residents, from a universe of 495, participated in this study (a higher number than the calculated sample size, n= 83), but only 62 (69.7%) questionnaires were analyzed because of incomplete submissions. This answering frequency must be debated for several reminder messages were sent. As possible explanations, nonresponse can have had to do with fear of suffering IP, fear of showing the sufferance of IP, and answering the questionnaire and not sending it for fear. Future studies must answer the personal reasons for fear of answering context questions.
No important correlation was observed between the PHQ-4 class and the CIPS class. So, the IP for this sample is independent of distress, anxiety, or depression raising a sharp problem to be studied in the future. It is a fact that 11.6% of Medicine students experienced few, 29.6% moderate, 42.2% frequent, and 16.6% intense impostor feelings, with women having the highest prevalence of the IP (p=0.030). No significant differences existed between the several years of residence (p=0.362). A moderate and significant correlation existed with the PHQ-4 scale (ρ=0.565; p<0.01), with impostor feelings being related to lower satisfaction with the curriculum average (p<0.001). 17
Of the 62 participants, 12.9% (n=8) had few, 22.6% (n=14) moderate, 43.5% (n=27) frequent, and 21% (n=13) intense IP experience. Thus, most residents presented frequent or intense Impostor feelings (43.5%), revealing the severity of IP in these responding resident’s, somehow different from other studies. 2,7,9-11 In the categories of few IP and moderate IP, men showed higher prevalence (16.7% and 41.7%, respectively), while in the higher levels of IP, frequent and intense, women showed higher levels (43.5%; 21%, respectively), consistently with other studies. 16 These results show the need for more studies in this area exploring if this is a pattern of residents or if it is related to the residency, or the context of the Portuguese general practice in the National Health Service. These results also raise the need for mental health care at individual and structural levels. The difference between genders must now be studied by qualitative studies, but individual personality or psychological traits and also career aspects may be involved.
A significant difference in satisfaction with the average mean mark in the 2nd, 3rd and the 4th-year of residency and the CIPS levels of the participants (p=0.043) was observed, residents with higher average scores had higher IP scores. This could be explained by perfectionism, which is a personality type associated with IP. 3
Regarding the year of residency, no statistically significant differences related to IP were observed, which is corroborated by other studies already conducted. 9,11,16
No relation was found between CIPS and PHQ-4, which differs from previous studies showing a positive correlation between feelings of imposter and mental health problems, namely, distress, anxiety, and depression. 11 The reasons for this must now be studied. A defense mechanism may have been put in place by young doctors dating back to the time when they chose to study medicine, one of the areas with the highest marks to enter College studies.
Although a representative sample was collected, generalization to all residents in Portugal is not possible, since there are factors that make residents’ experiences different, namely cultural, socioeconomic, and psychological, across Portugal. The results in this study may have been influenced by the intrinsic quality of the respondents. One must inquire about the reasons for this sample dimension even though there were reminders. As reasons for this kind of response, one can think of tiredness of answering questionnaires, fear of answering, intuition of bad results, and sufferance with the reading of questions leading to answering rejection. This ambiance defies the medical community linked to the residency in general practice and family medicine to respond. The problems may come back from pre-graduate studies still there is a need to think about what to do in pre-graduate and post-graduate preparing the kind of doctors the country and humanity need.
Given the harmful effect of IP on residents, there are three key actions to take: recognize, increase awareness, and manage IP. This management must involve both individual and institutional measures. 6-7
At the individual level, cognitive-behavioral interventions must be implemented, to improve self-awareness, and perception of thoughts and behaviors associated with IP. 7 Peer support can be very beneficial in combating IP, so residents should acknowledge and share feelings of IP with trusted peers who share the same problem and ask for truthful and objective feedback from mentors. The practice of self-compassion, the maintenance of the record of one’s accomplishments, the development of skills to achieve goals, and the open discussion about residency objectives (great marks or great doctors) may model a growth mindset. Furthermore, if needed, attend individual or group psychotherapy. 3,7
However, doctors may not seek the support they need from the healthcare institutions they belong to, so healthcare organizations themselves should act preventively, screening and implementing strategies, such as workshops and inclusive learning environments to address, manage, and reduce IP. 3,7 In the future, more research should be conducted to assess the impact of these interventions in reducing imposter feelings.
Further studies are essential to expand the application of the CIPS in General Practice Resident from other regions of the country, as well as to physicians, to determine the prevalence of IP and possibly establish a comparison, considering the variables of the different study groups.
Conclusions
In this sample’s study, 87.1% of the residents had an IP score at or above Moderate, higher levels of IP more frequently in women, but not different per year of residency.
As for the satisfaction with curriculum mean mark of the 2nd, 3rd, and 4th-year of residency, a relation was found with the values of IP, since the 3rd-year residents showed lower impostor feelings values (between 26-83) than the 2nd and 4th-year (between 32-87 and 35-96, respectively).
There was no relationship between IP levels and the participants’ levels of distress (p=0.701).
Authors contribution
Conceptualização, APP, LMS e JAS; metodologia, APP, LMS e JAS; software, APP e LMS; validação; APP, LMS e JAS; análise formal, APP, LMS e JAS; investigação, APP, LMS e JAS; recursos, APP, LMS e JAS; gestão de dados, APP e LMS; redação do draft original, APP, LMS e JAS; revisão, validação e edição do texto final, APP, LMS e JAS; visualização, APP, LMS e JAS; supervisão, LMS e JAS; administração do projeto, LMS e JAS.

