











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Defensive medicine is defined as a deviation from standard medical practice for fear of medical malpractice claims and may include two types of behaviors: a safety behavior which consists of prescribing more tests and procedures than those clinically recommended, and an avoidance behavior which involves avoiding high-risk procedures and/or patients to distance oneself from possible malpractice.1
Defensive medicine is on the rise, and it has been demonstrated in healthcare systems around the world. Patients are increasingly dissatisfied with health services and resort to litigation more easily. Physicians fear malpractice proceedings and adopt self-defense conduct that deviates from standard practice. These actions can have serious consequences for patients’ and physicians’ health,2 besides wasting public funds. 3 For all these reasons, it seems mandatory to build preventive strategies. There is some international literature available about the impact of defensive medicine on clinical practice. In Spain, the main reasons mentioned by family doctors for prescribing unnecessary procedures were to increase patient satisfaction, the lack of time during appointments, and fear of malpractice claims. 4 In Denmark, a qualitative study explored how defensive medicine was understood by family doctors in primary health care (PHC). It was described as all unnecessary and meaningless medical procedures due to external factors such as pressure done by patients, other professionals, or their own.1 In 2015, in the United States of America, another study showed an association between greater use of resources and lower subsequent rates of negligence incidents. However, this association was not statistically significant in PHC, which may reflect low rates of malpractice claims in general or a lower number of family doctors included compared with other specialties. 5
National literature about defensive medicine in PHC is scarce. In Portugal, the National Healthcare System (SNS, from Serviço Nacional de Saúde) was founded in 1979 and is described as universal, general, and tending-towards-free health service. It operates under the supervision of the Ministry of Health and is managed by the Central Administration of the Health System and by five Regional Health Administrations (RHA). Each RHA includes several groups of PHC centers and hospitals that work in a network based on geography and care differentiation. PHC contemplates three types of functional units with a growing level of organization, professional goals, monetary incentives, and cost controls: personalized healthcare unit (UCSP), family healthcare unit model A, and model B (USF A and B). Physicians can work in public and private health services simultaneously.
Objectives
Our main goal was to understand the perception of the practice of defensive medicine in PHC, specifically in the primary healthcare centers group of Western Lisbon and Oeiras (HCG WLO).
Secondarily, we aimed to describe the demographic characteristics of HCG WLO’s family doctors staff; understand their perception regarding health costs associated with defensive medicine; identify the reasons that lead to the practice of defensive medicine; describe how physicians practice defensive medicine in their work routine; verify if any specific patient characteristic was associated with more frequent defensive medicine practice; and survey which strategies were suggested by family doctors to reduce the practice of defensive medicine.
Methods
Study design and settings
We used a cross-sectional design for this study. The research protocol was approved by the Ethics Committee of the Regional Health Administration of Lisbon and Tagus Valley.
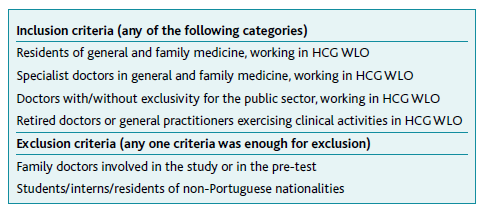
The study began in May 2019, with the design of the protocol and the elaboration of a questionnaire by the research team, which after being subjected to a pre-test to detect any difficulties and having not identified any need for modification, was then applied to the family doctors which met the inclusion criteria, in all the functional units of the HCG WLO, Lisbon, Portugal (see Table 1). Questionnaires distribution was initially planned for September 2019 but was delayed until August 2020 due to complications with the approval of distribution of the questionnaires in some of the functional units and the COVID-19 pandemic. In October 2020, the questionnaires were collected by the research team, and the information obtained was subjected to statistical analysis.
This article follows STROBE guidelines.
Participants
The total number of doctors who work at HCG WLO was obtained through its human resources department, divided by professional category (specialists/residents in general and family medicine and general practitioners), ensuring anonymity of all participant data. All physicians who met the eligibility criteria defined in Table 1 were included in this study. The research team tried to reduce the existence of confounding factors by creating exclusion criteria. Thus, some possible confounding factors were not considered in the statistical analysis.
Variables
The initial questionnaire was submitted for validation by the Ethics Committee to maintain the anonymity of the study participants, and some changes were made. The final questionnaire integrating the variables under study (see Table 3) has the main objective of characterizing the practice of defensive medicine by family doctors at the HCG WLO. On the other hand, it intends to know the reasons that lead to the practice of defensive medicine, how defensive medicine is practiced in their daily activities, and which factors, human or not, may influence the physician to practice defensive medicine. It also intends to evaluate the physician’s perception regarding the financial impact of the practice of defensive medicine and to understand which strategies to reduce defensive medicine are considered more useful by family doctors.
Each author was responsible for personally delivering the questionnaires and informed consent in a sealed envelope to a randomly assigned primary healthcare center coordinator. Both questionnaires and envelopes were not signed, stamped, or had vignettes identifying the participating physician or healthcare center. After the two months that were defined as the period for completing the questionnaires (August and September 2020), the authors collected the envelopes and transcribed the data into an Excel® database. To minimize the potential error in the transfer of information, the transcriptions were subsequently independently reviewed by another member of the team, and the author, JR, did not transcribe or review any questionnaire. The database was protected by a password, and it was only accessible to the research team. To reduce the rate of non-response to the questionnaire, the authors committed to reinforcing the delivery times in person with the family doctors of the healthcare centers where they worked, and some periodic kind reminders were sent to the other centers.
After data collection, the paper questionnaires were stored in a physical folder, together with the informed consent. Three years after the completion of the study, the Excel database and the physical folder will be eliminated. If the responsible author verified that question number 8 of the questionnaire was not answered, the questionnaire was excluded from the study.
Data sources/Measurement
To the best of our knowledge, the study was the first of its kind in Portugal. The research team prepared a questionnaire that was subjected to a pre-test by a total of six family doctors, who understood the questions and did not identify the need for changes. As an opinion questionnaire, consisting of categorical variables, its results are measured in frequencies.
In this study, the exposure was the practice of defensive medicine, and the intended outcomes were the perception of defensive medicine by the primary healthcare physician regarding its importance, daily practice, direct costs for the Portuguese healthcare system, and strategies for its reduction. Being a cross-sectional study, the descriptive analysis of the variables and the identification of potential associations between them was also intended.
Bias
During the design of the questionnaire, several aspects were considered to reduce the risk of bias. Thus, when preparing the questions, the team was careful to avoid using not only ambiguous, complex, or rare words but also to avoid any phrases that were too long or too short so that the objective of the question was easily understood by the participant. The questionnaire was self-administered and related to the clinical practice of each physician, which can lead to a bias of belief vs. behavior in which the answer is not correlated with their practice, but rather to their belief or vice versa. Another bias that we considered was that of social desirability. However, these are biases that could not be minimized, given the nature of the study. The questions were intended to be straightforward, simple, and in an adequate number so that the time to complete them was easily acceptable by the participants. The questionnaire allowed participants to comment on several questions, so some perspectives were obtained and analyzed. Other biases to consider are the bias of the volunteer and the bias of memory. Thus, results should be critically interpreted when analyzed.
Statistical methods
Information about defensive medicine in Portuguese primary healthcare is scarce, so we chose to do exploratory descriptive analysis and study potential associations between variables. To do so, data analysis was performed by the author JR, using the software SPSS®, v. 27. All questionnaires in which question 8 was not answered or the answer was «Do not know/Do not answer» were excluded (2%). Although some questionnaires had missing data points, 85% were fully answered, so missing data points were ignored in the analysis due to the exploratory nature of the study. For descriptive analysis, we included nominal categorical variables such as sex; professional situation; workplace; private activity; economic impact of defensive medicine; previous practice of defensive medicine; reasons for the practice of defensive medicine; translation of the practice of defensive medicine; gender influence in the practice of defensive medicine; economic class influence in the practice of defensive medicine; age influence in the practice of defensive medicine; defensive medicine leading to lesser probability of prosecution; knowing someone sued for negligence and preventive measures of the practice of defensive medicine; and ordinal categorical variables such as age; the practice of defensive medicine as a problem; frequency of the practice of defensive medicine and probability of being sued in the next ten years.
The statistical analysis of categorical variables, regardless of their classification as nominal or ordinal, was done with absolute and relative frequencies.
Statistical tests such as Chi-square or Fisher were carried out to compare categorical variables and thus establish possible associations and correlation was assessed through Pearson’s coefficient. There was no need to carry out a sensitivity analysis.
Results
Participants
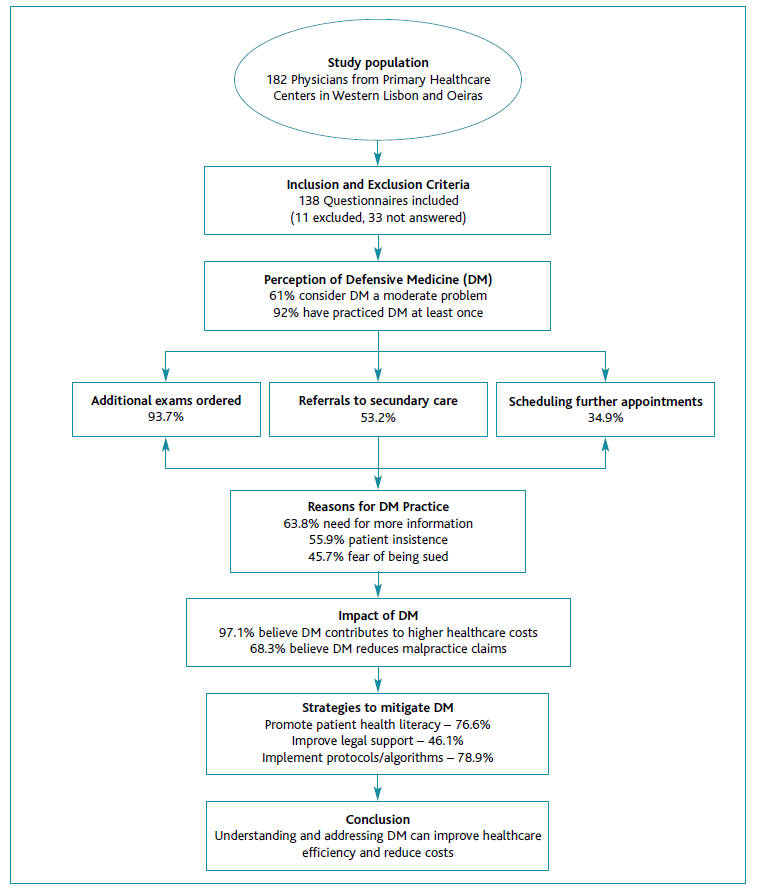
Of the 182 clinicians who met the eligibility criteria, 138 (75.8%) of the family doctors completed the questionnaire. Only 33 (18.1%) did not complete the questionnaire, as requested. Of the remaining 11 (6.1%), eight were part of the research team, two did not answer question 8 and were thus excluded, and one had previous access to the protocol.
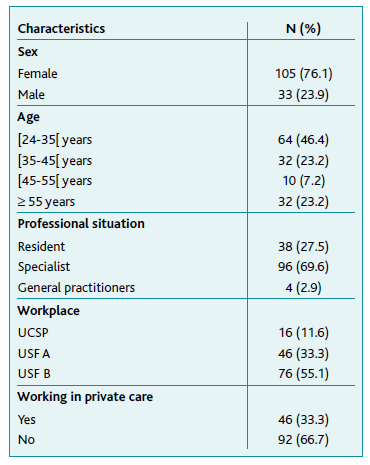
Most of the functional units of the HCG WLO were USF A (33.3%) or B (55.1%), with teams made up mostly of female family doctors (76.1%), specialists in general and family medicine (69.9%) and aged between 24-35 years (46.4%). Most maintained exclusivity with the SNS (66.7%).
Table 2 shows the socio-demographic characteristics of the population studied in greater detail.
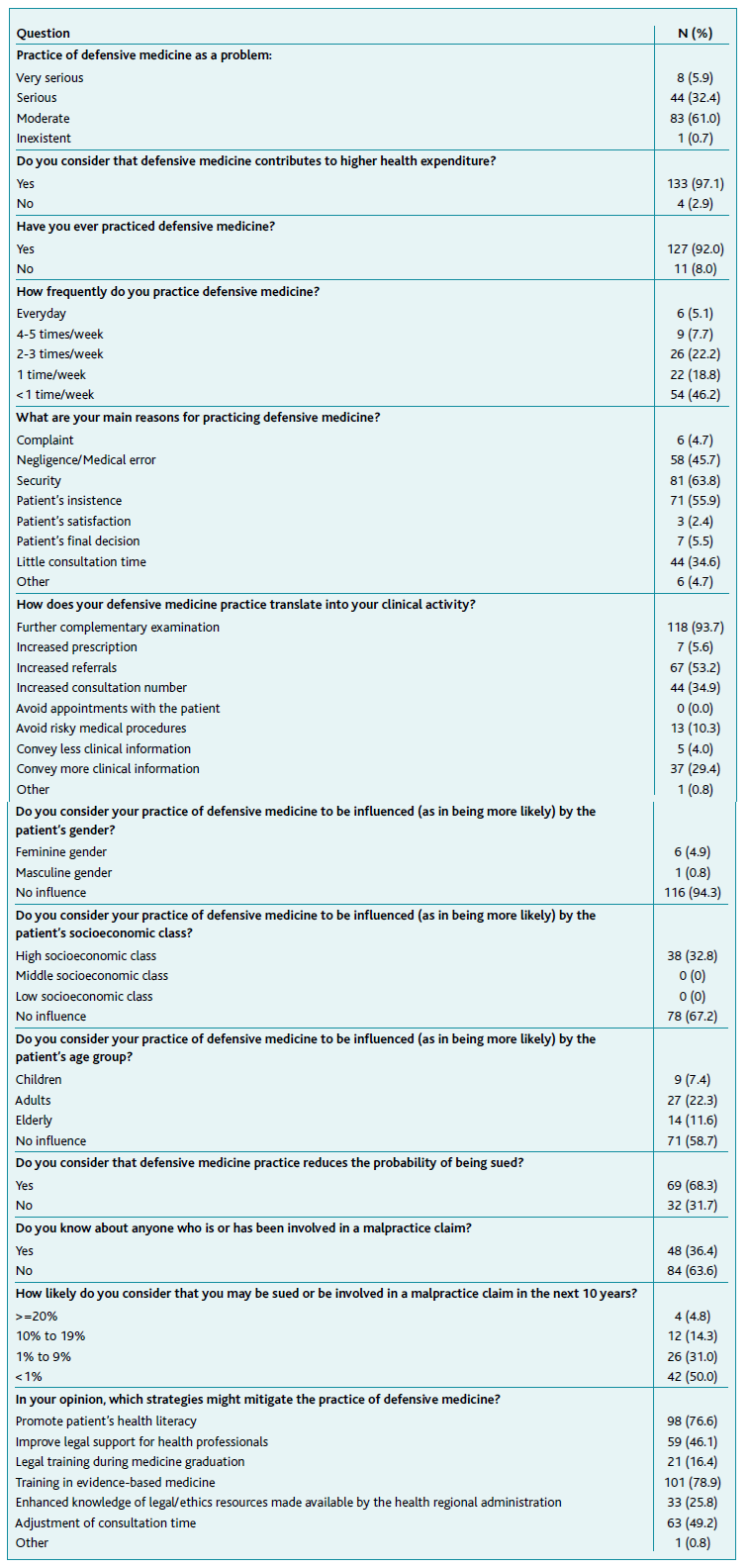
About 61% of family doctors consider the practice of defensive medicine to be a moderate problem and 32.4% a serious problem. The vast majority (97.1%) consider that the practice of defensive medicine contributes to higher health expenditures.
In our study population, 92% of family doctors reported having already practiced defensive medicine in their clinical practice, and approximately half (46.2%) practiced defensive medicine less than once a week, followed by 22.2% of family doctors who practiced defensive medicine two or three times a week. The main effects of defensive medicine practice considered by family doctors were additional exams (93.7%), referring to secondary care (53.2%), and scheduling further appointments (34.9%).
The majority (63.8%) of family doctors attributed the practice of defensive medicine to the need for more information to be safe in their clinical decision, 55.9% to the patient’s insistence, and 45.7% to the fear of being sued for a medical error or negligence. Other reasons cited for the practice of defensive medicine included insufficient response from the secondary health care system (both for the patient and for family doctors), teleconsultations, recurrent and/or persistent complaints from patients, difficulty in obtaining adequate clinical history (due to teleconsultation or other communication barriers with the patients), prevention of conflict with the patients (even when not resulting in complaints).
The majority of family doctors who practice defensive medicine do not consider themselves as being influenced by the patient’s gender (94.3%) or age (58.7%). Though most family doctors do not consider themselves to be influenced by the patient’s socio-economic class (67.2%), 32.8% considered the high socio-economic class an influencing factor to practice defensive medicine.
Regarding the probability of being sued, 68.3% believe that it decreases with the practice of defensive medicine. Still, 63.4% do not know other professionals involved in medical malpractice cases. Concerning the likelihood of being sued or involved in a case of negligence in the next 10 years, 50% of doctors assumed less than 1% probability. However, a significant proportion of respondents (31%) considered that the probability could be between 1-9%.
The majority of physicians (78.9%) think that the implementation of protocols/performance algorithms based on current scientific evidence could be one of the strategies to be adopted to reduce the impact of defensive medicine. Additionally, the promotion of health literacy among patients (76.6%), the adjustment in consultation time (49.2%), and the improvement of legal support for health professionals (46.1%) were the most frequently mentioned measures. The development of communication between primary and hospital care through consultation meetings was one of the suggestions pointed out by clinicians as an attempt to mitigate defensive medicine (see Table 3).
In our sample, there was no statistically significant association between family doctors’ gender, professional status, or private practice and the frequency of practicing defensive medicine, which for this analysis was recoded into three groups: less than once a week (n=54; 46.1%), one to three times a week (n=48; 41.0%) and more than three times a week (n=15; 12.8%). However, there was a weak but statistically significant association between the workplace and the practice of defensive medicine (Pearson’s correlation coefficient of -0.278), suggestive of a tendency for less frequent practice of defensive medicine in model B USF compared to model A USF.
Discussion
The main goal of our study was to understand the perception of the practice of defensive medicine in PHC, specifically in the HCG WLO. Figure 1 presents the summarized analysis of the study. Our results show that most family doctors have already practiced defensive medicine in their daily clinical activities, the majority practicing less than once a week, followed by doctors who practice two to three times a week.
Although the reasons for defensive medicine practice differ, most doctors emphasize the need for more information to be sure about the clinical attitude to take, and still, a significant number of doctors refer to the fear of committing a medical error or being perceived as committing one by the patient, with the possible consequence of a malpractice claim. The study suggests that family doctors understand the concept of defensive medicine, are aware of their defensive medicine practice and its’ negative economic outcomes. The absence of good communication between secondary and primary care providers was also appointed by the respondents. When physicians practice defensive medicine, they do it mainly by prescribing more complementary exams and more referrals to secondary health care, which seems to agree with what has been observed in the literature.
On the other hand, contrary to what the literature mentioned, family doctors do not seem to feel the need to practice defensive medicine when they observe children, women, or people of a higher socioeconomic class. Most doctors practice defensive medicine less than once a week, and about half assume the likelihood of being sued within 10 years is extremely low. However, in addition to considering the practice of defensive medicine as a moderately serious problem, the family doctors report that the practice of defensive medicine reduces the risk of having a malpractice claim. When asked about strategies to reduce the growth of defensive medicine, they point out several that they consider important to be applied in primary health care, namely, the promotion of health literacy among patients, the adjustment in consultation time, and the improvement of legal support for health professionals.
Although they believe that practicing defensive medicine would decrease their probability of being sued, the reality is that family doctors in HCG WLO practice less defensive medicine. This could be because physicians are familiar with the concept of defensive medicine and recognize its negative impact on both costs and health outcomes and/or because participants’ responses were towards what it would be socially and desirably the correct answer. The results, therefore, must be interpreted critically.
Residents do not practice more defensive medicine than specialists, contrary to what would be expected, and this can perhaps be explained by the fact that their work is supervised. Possibly, they find it easier to discuss clinical doubts with their supervisors, and despite having clinical autonomy, they are legally protected during the medical internship. Regarding the workplace, there seems to be a statistically significant relationship, but weak between the workplace and the practice of defensive medicine, and we were able to conclude that the physicians from the model B USF practice less defensive medicine than the physicians from the model A USF. A possible interpretation of this result is that these units work different objectives, namely in terms of access, health/disease management, prescription qualification, continuous quality improvement, and internal training, and others, which must be completed annually to receive the financial incentives that are intended for them. Thus, the prescription qualification and the internal training can be interpreted as limiting factors for the growth of defensive medicine in these units since they are related to an obligation to update the scientific knowledge of physicians and the need to consider the best cost-effectiveness of all medical acts. This option can be strengthened considering the participants’ responses related to the strategies to prevent defensive medicine growth in PHC, in which the highlight is the implementation of protocols/algorithms based on current scientific evidence.
Other limitations of this study, beyond the aforementioned biases, are the absence of a validated questionnaire that could be applied to Portuguese doctors because, as far as we know, this is the first study to explore this topic and probably a quantitative descriptive study may not be the best option for a field which is still in an exploratory phase of understanding. And so, a qualitative study, with focus groups or other methodologies, could be of greater value to better understand the relationship between family doctors and the practice of defensive medicine.
We cannot directly extrapolate these results to other HCG. They provide a useful first insight into the topic of defensive medicine in PHC and serve as the basis for studies in other HCGs. Although most family doctors at the HGC WLO do not practice defensive medicine, in general, they are aware of its importance and its negative impact on health. We do not know the reality of defensive medicine practice in other HRA, so research is needed nationwide, not only to understand the real scope of influence of defensive medicine in medical practice but also to develop and implement measures to prevent its growth in primary health care.
Authors contribution
Conceptualização, ACE, CBC e MF; metodologia, ACE, CBC, MF, MS, LF, ST, SJ e CC; software, JR; análise formal, JR; investigação, ACE, CBC, MF, MS, LF, ST, SJ e CC; redação do draft original, ACE, CBC, MF, MS, JR, LF, ST, SJ e CC; revisão, validação e edição do texto final, ACE, CBC e MF; supervisão, ACE.

