











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Mental health problems are very common and represent a significant portion of health-seeking contacts in primary health care. Depression and anxiety disorders are among the most common mental health issues and constitute an important cause of morbidity on a personal and social level, contributing to social isolation, absenteeism, and premature mortality.1-2 Given the prevalence and impact of mental health disorders, they constitute a public health priority, increasingly demanding initiatives that promote social integration and well-being of these patients. 3-4 Primary health care professionals, due to their proximity and continuity of care, may have an important role in identifying these patients and guiding them to these initiatives. Local non-governmental organizations with volunteering necessities may be an essential community partner.
Studies have shown that volunteer work promotes not only mental health but also social inclusion and is related to lower anxiety and depression symptoms. 5-6 The PERMA model7 proposes five pillars on which psychological well-being and happiness are based - Positive Emotions, Engagement, Relationships, Meaning, and Accomplishments. As there are studies suggesting an association between volunteering and these parameters of well-being, 8-9 our work aimed to implement an intervention project with people who suffer from properly diagnosed anxiety and/or depression disorder to improve their depression and anxiety scores and foster psychological well-being, happiness, sense of accomplishment, and belonging.
Methods
Participants and procedure
Participants were selected opportunistically among a sample of patients from the Family Healthcare Unit of Valongo (USF Valongo), with ages between 18 and 64 years old, classified with the International Classification of Primary Care (2nd edition; ICPC-2) P74 - Anxiety disorder/anxiety state and/or P76 - Depressive disorder codes and medicated with anxiolytics and/or antidepressants. They were selected during medical appointments at USF Valongo. Patients who met the criteria described and agreed to participate in the project were included.
The intervention was carried out by Pista Mágica, a Portuguese non-governmental organization for development, focused on the participants’ empowerment through training sessions on self-development, empathy, volunteering and psychoeducation; group volunteering activities accompanied by a volunteering professional, such as organizing and sorting donations, supporting the elderly and people with different types of disabilities, distributing meals to the homeless, providing care to ownerless animals, etc.; definition of individual happiness projects; and individual volunteering activities aligned with each participant’s needs, dreams and objectives. This was a pilot project, so there was no previous experience involving volunteers with the mentioned characteristics.
The project lasted for a year, with participants attending weekly sessions.
Participants were informed about the study procedures and aims. They were notified that the participation was voluntary. Informed consent was obtained, and confidentiality of data was ensured.
Instruments
Validated questionnaires for the Portuguese population were applied at the beginning and at the end of the intervention to screen for anxiety and/or depression symptoms.
The Hamilton Anxiety Scale (HAM-A) was used to screen for anxiety symptoms. This scale is composed of 14 items whose total score indicates if the patient has mild (<17), moderate (18-24), or severe anxiety (>24 points) 10-11.
The Portuguese version of the 9-item Patient Health Questionnaire (PHQ-9) was used to screen for depression symptoms. 12-13 The questionnaire is composed of nine questions and objectifies the grade of depressive symptoms in mild (<10), moderate (10-14), moderate to severe (15-20), or severe (>20) depressive symptoms.
At the end of the study, a questionnaire created by the researchers was applied to the volunteers to assess the perception of the project’s impact on each participant. The questionnaire consisted of eight subjective statements with a 6-point Likert scale ranging from 0 (Not applied) to 5 (Totally agree).
Statistical analysis
Data analysis was conducted using IBM Statistics SPSSⓇ, v. 29. Descriptive statistics were used to summarize sample characteristics, as gender (male/female) and age group (age 18-29, 30-49 or above), time on project and volunteer hours, as well as the number of participants in each level of anxiety/depression according to the HAM-A and PHQ-9 scales. Since the data was not normally distributed, nonparametric tests, namely the Wilcoxon Signed Ranks and Mann-Whitney U, were conducted to identify any significant improvement in anxiety and depression between T0 (pre-intervention) and Tf (post-intervention). The results of the scale assessments at T0 and Tf were presented using the median [min-max]. A p-value of <0.05 was considered statistically significant.
Results
Group description
According to the inclusion criteria, 33 participants joined the project. Of these, eight were lost during follow-up and, therefore, excluded from the project, for a total of 25 participants (n=25).
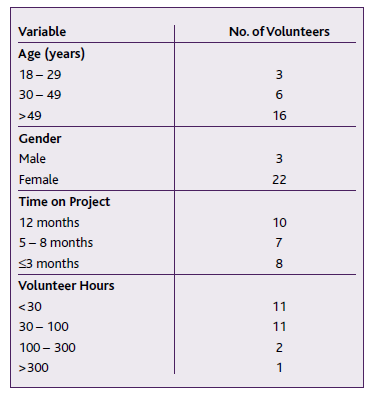
Most participants were 50 years of age or older (n=16) and female (n=22) - Table I.
Project lead times
The project lasted a total of 12 months, but only 10 participants attended the whole period; seven participants took part in the project for five to eight months, and the rest for three months or less (Table I).
All volunteers initially completed five to eight hours of training sessions on self-knowledge, empathy, volunteering, and psychoeducation.
Among the 25 participants, 11 completed less than 30 hours of volunteering; 11 completed 30 to 100 hours; two performed 100 to 300 hours, and one performed more than 300 hours - Table I. On average, participants completed approximately 48 hours of volunteering.
Scales
Anxiety (HAM-A)
Total group
At the beginning of the study (T0), according to the scale HAM-A, three participants presented mild anxiety levels, eight moderate anxiety, and 14 severe anxiety. After intervention (Tf), only six of them remained with severe anxiety.
The median of the scale scores between the two assessments decreased from 28 to 17, with statistically significant differences (p<0.001).
Group with ≥30h of volunteering
Highlighting the group of participants who volunteered ≥30 hours (n=14), seven participants had severe anxiety at the beginning of the study, while only four had this level of anxiety after the intervention.
There are statistically significant differences between the median scores of pre- and post-intervention assessments (p=0.026).
Group with <30h of volunteering
Regarding the group of participants who volunteered <30 hours (n=11), seven participants had severe anxiety at the beginning of the study, while only two showed this level of anxiety after the intervention.
There are statistically significant differences between the median scores of the pre- and post-intervention assessments (p=0.006).
The results described above are labelled in Table II.
Table II No. of participants by levels of intensity of anxiety symptoms. Median HAM-A scale scores
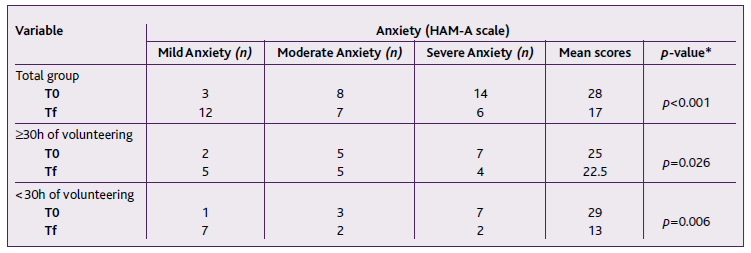
*p-value = Wilcoxon Signed Ranks Test. T0 = Beginning of the study; Tf = After intervention.
Depression (PHQ-9)
Total Group
According to the PHQ-9 scale, at the beginning of the study, 11 participants had moderate depressive symptoms, seven had moderate to severe symptoms, and three had severe symptoms. After the intervention, 22 volunteers presented mild depressive symptoms and three presented moderate symptoms; no one presented moderate to severe or severe depressive symptoms.
The median of the scale scores between the two assessments decreased from 12 to five, with statistically significant differences (p<0.001).
Group with ≥30h of volunteering
Highlighting the group of volunteers who volunteered ≥30 hours (n=14), 12 participants had mild depressive symptoms at the end of the study, and two presented moderate symptoms; no one presented severe depressive symptoms.
There are statistically significant differences between the median scores of the pre- and post-intervention assessments (p<0.001).
Group with <30h of volunteering
Regarding the group of participants who volunteered <30 hours (n=11), 10 participants had mild depressive symptoms at the end of the study, and one presented moderate symptoms; no one presented severe depressive symptoms.
There are statistically significant differences between the median scores of the pre- and post-intervention assessments (p=0.003).
The results regarding depression evaluation are described in Table III.
Table III No. of participants by levels of intensity of depressive symptoms. Median PHQ-9 scale scores
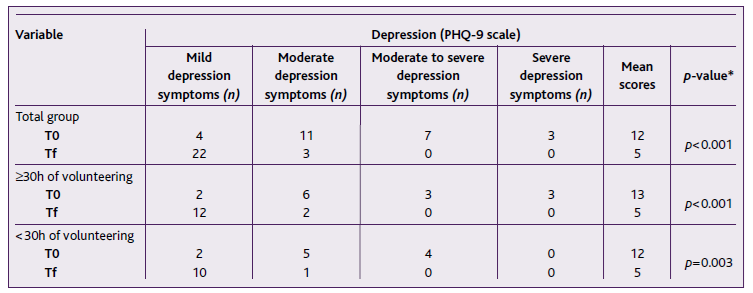
*p-value = Wilcoxon Signed Ranks Test. T0 = Beginning of the study; Tf = After intervention.
Group with ≥30h of volunteering vs Group with <30h of volunteering
The differences between the two groups, at T0 and Tf, were not statistically significant for anxiety (p=0.366) or depression (p=0.739).
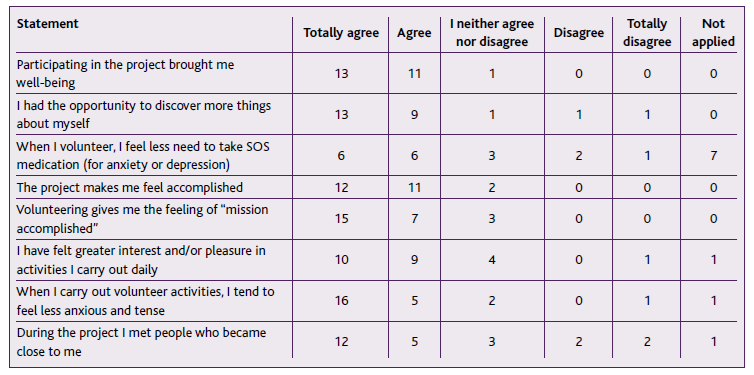
Subjective questionnaire
More than 65% of participants marked «agree» or «completely agree» in all statements present in the subjective questionnaire, applied at the end of the intervention (Table IV).
The statements “Participating in the project brought me well-being” and “The project makes me feel accomplished” presented more than 95% agreement responses.
Furthermore, 85% of participants agreed that they felt less tense and anxious when volunteering and more than 75% of participants increased their interest and pleasure in day-to-day activities. For 68% of participants, the project increased the network of people close to them.
Discussion
To the best of our knowledge, there are no studies yet published regarding the impact of volunteer work on the mental health of people who suffer from anxiety and/or depression disorder in the Portuguese population. Our data suggests that these initiatives may contribute to increasing the well-being and mental health of these patients, which corroborates previous studies regarding other populations. 14
In our sample, there was a significant reduction in the anxiety and depression scores, which is in line with extensive previous literature. 15-16 However, this considerable reduction was observed regardless of the number of hours spent volunteering, unlike preceding studies indicate. 17 This might suggest the importance of being engaged in a meaningful activity like volunteering, and that the engagement by itself can have a quick effect on these patients’ well-being.
We found with the subjective questionnaire that our patients felt that the volunteering program increased their sense of belonging and accomplishment, their well-being and the pleasure they felt with daily activities. In addition, the results show that our patients’ self-perceived levels of anxiety or tension decreased while performing volunteer activities.
The limitations of this paper mainly concern the project’s design since it does not allow the determination of causality between the qualified and accompanied volunteer work and the reduction of anxiety and depression scores observed. Also, the lack of random assignment led to confounding variables that were not controlled by the investigators, such as changes in medication, psychological support, concomitant personality disorders, and social aspects that normally coexist with anxiety/depression, making it difficult to determine causality. Furthermore, the sample size and its lack of representativeness limit the possibility of generalizing the results. Given the different periods of project participation, standardizing the intervention becomes difficult.
Besides the limitations, the reduction in anxiety/depression scores is statistically significant in this sample, which aligns with the results of the subjective questionnaire, suggesting that volunteer work can play a role in the patients’ well-being, which is consistent with the literature.
For future research, it would be important to study this question through a clinical trial or at least standardize the intervention period and obtain a larger and more representative sample of the adult population in terms of age range, unlike this study, where the vast majority of participants were aged 50 or over. In this study, only adults up to the age of 64 were included, to contribute to the integration of patients on sick leave or unemployed people into society. However, the literature also indicates greater benefits of volunteering on the mental health of the elderly, 15-16 which highlights the importance of extending the project to older ages in the future.
Although the benefits found were independent of the number of volunteering hours, more studies will be needed to understand whether this will be a determining variable. A possible confounding factor is that all participants had attended training sessions before volunteering, which may have influenced the results (e.g., improving participants’ self-esteem). Therefore, we cannot assume that volunteering without these sessions will have the same impact.
Even so, we consider the previous training sessions to be, in fact, a crucial part of the volunteering process, especially for people suffering from mental health disorders, promoting a more self-conscious and adequate volunteering.
In subsequent studies, it would be relevant to evaluate other variables that may influence the results, such as changes in medication, life-changing events, seasonality, comorbidities that limit the participation in volunteering activities (acute diseases, surgeries, hospital stays...), support network vs loneliness, concomitant psychological support, social aspects that normally coexist with anxiety/depression as poverty, unemployment, domestic violence, burnout, pathological grief, among others.
Conclusion
This study suggests that volunteering managed by a qualified mental health professional, following a specific methodology that includes training on self-knowledge, empathy, volunteering, and psychoeducation, can help lower the anxiety and depression scores and increase the patients’ self-perception of accomplishment and well-being.
It seems that an intervention (training and accompanied volunteering) based on the PERMA model, that creates opportunities to feel positive emotions, engage with the community, build relationships based on empathy, find meaning and sum accomplishments, may truly contribute to psychological well-being and impact anxiety/depression patients’ quality of life through personal empowerment and the possibility to change one’s self-perception.
This intervention proposes that qualified and accompanied volunteer work can be a complementary approach to treating anxiety and/or depression symptoms, helping these patients in their social reintegration.
Family doctors are closer to the community and, therefore, are more likely to use social prescribing as a complement in the management of some pathologies. However, it remains to be understood how doctors can include volunteering in their prescriptions.
Acknowledgments
The intervention carried out by Pista Mágica, the VoluntariaMente project, was funded by the Active Citizens Program, originating from Iceland, Liechtenstein, and Norway through the EEA Grants, managed by Fundação Calouste Gulbenkian in consortium with Fundação Bissaya Barreto.
Authors contribution
Conceptualization, AG, PT, SA, and FSC; methodology, AG, PT, SA, and FSC; software, AG, PT, and SA; validation, PT, SA, AG, ASF, FSC, PC, and BTR; formal analysis, PT, SA, AG, and ASF; investigation, PT, SA, and AG; resources, PT, SA, AG, and ASF; data curation, PT, SA, AG, ASF, and PC; writing - original draft, PT, SA, and AG; writing - review & editing, PT, SA, AG, ASF, FSC, PC, and BTR; visualization, PT, SA, AG, ASF, FSC, PC, and BTR; supervision, PT, SA, AG, ASF, FSC, PC, and BTR; project administration, PT, SA, and AG;

