











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkCase Presentation
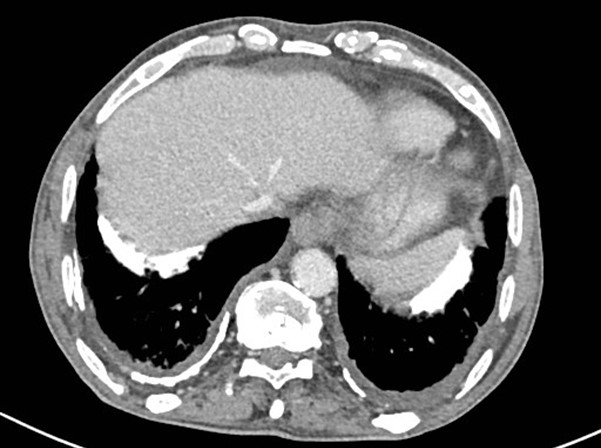
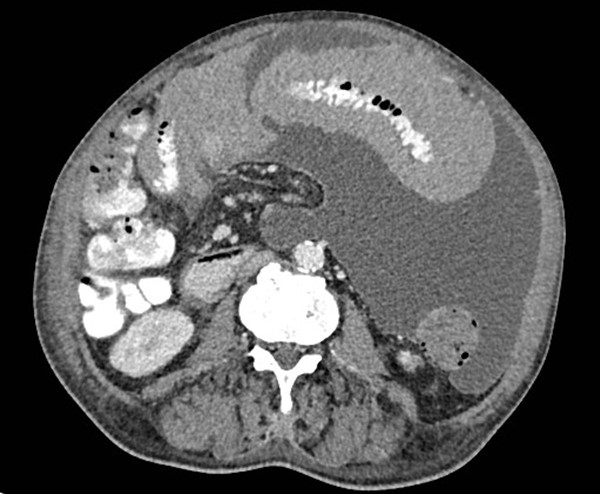
72-year-old male, referred to our hospital due to 5-month history of dry cough, increasing abdominal discomfort and feeling of abdominal fullness. Laboratory results revealed anaemia, mild leucocytosis and elevated C-reactive protein levels. The patient had a history of long exposure to asbestos. Ultrasound was initially performed, showing unspecific peritoneal thickening (Fig.1) and was followed by Computed Tomography (CT), which showed peritoneal and mesenteric mass-like soft tissue thickening with bowel encasement and moderate ascites (Figs. 3, 4, 5). No enlarged lymph nodes were seen. Calcified pleural plaques were observed at the lung bases (Fig. 2).



Discussion
Mesothelioma is a rare malignancy of serosal membranes, most frequently encountered in the pleura. The second most common location is the peritoneum and it may also arise from the pericardium or the tunica vaginalis testes. It has been linked to toxic exposure to industrial pollutants, namely asbestos.
Malignant peritoneal mesothelioma (MPM) commonly presents with diffuse and extensive abdominal involvement. On CT it appears as a solid, heterogeneous enhancing soft tissue mass, with expansive rather than infiltrative characteristics and frequently diffuse distribution throughout the abdominal cavity. Little to moderate ascites is almost always present at the time of diagnosis and encysted peritoneal collections, scalloping or direct invasion of intra-abdominal organs and areas of peritoneal thickening and omental cake may also frequently be seen. Lymph node involvement and distant metastasis are usually not present. While peritoneal tumoral calcifications are uncommon, the presence of calcified pleural plaques, indicative of asbestos exposure, are a useful clue for the diagnosis.
However, CT findings are nonspecific and the differential diagnosis include peritoneal carcinomatosis, lymphomatosis, serous peritoneal carcinoma, ovarian carcinoma and tuberculous peritonitis. CT is useful for detection, characterization, staging, and guiding biopsy. The usefulness of MRI, PET or PET/TC for diagnostic purposes has still not been established. Serum markers such as serum mesothelin-related protein, CA-125, CA 15- 3, hyaluronic acid and osteopontin are potentially useful for diagnosis and follow-up.
MPM is frequently diagnosed in advanced stages and, if left untreated, has an aggressive course with median survival ranging from 5 to 12 months. Radical resection is associated with better prognosis and should be pursued whenever possible. Other treatments include cytoreductive surgery, early post-operative intraperitoneal chemotherapy and immunotherapy.

