











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Images in Case
A female patient in her 60s has been followed up with annual chest-abdominopelvic computed tomography (CT) due to a clinical history of extraskeletal mesenchymal chondrosarcoma with disseminated metastatic disease. She was previously submitted to various surgical treatments, namely excision of the primary lesion located on the left thigh thirteen years before, as well as bilateral pulmonary and colic metastasectomy, left adrenalectomy and nephrectomy, splenectomy and caudal pancreatectomy in 2019. In a routine contrast-enhanced thoraco-abdominopelvic CT, a round, solid mass was found with heterogeneous attenuation, as well as internal calcifications, occupying most of the right ventricular chamber, due to heart metastasis from extraskeletal mesenchymal chondrosarcoma. It involves the right apex and almost two thirds of the ventricular septum, causing discrete bulging to the left.(Figs. 1, 2 and 3)
At the time of this diagnosis the patient was under a second-line treatment with trabectedin for three years. No symptoms were reported, so the patient remained under vigilance with chest-abdominopelvic CT once a year, as previously established.
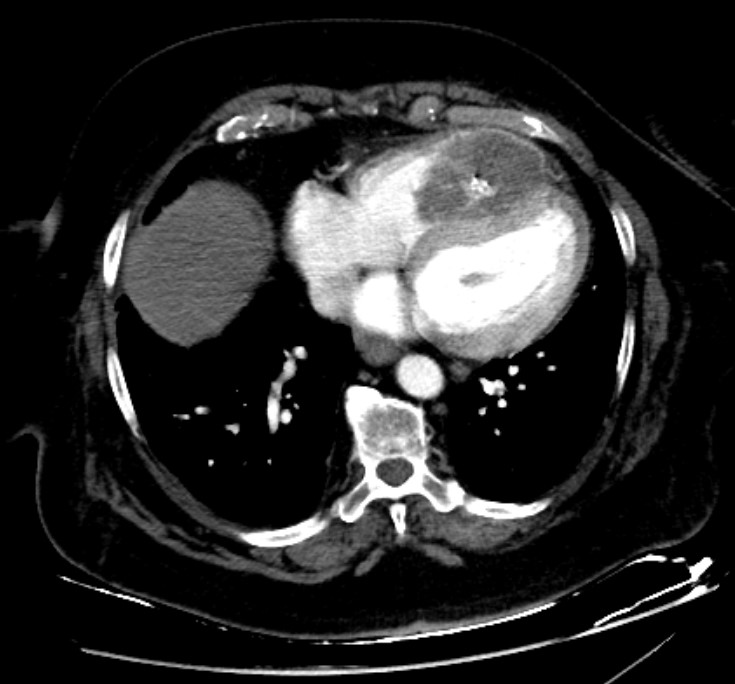
Figure 1: Axial contrast-enhanced CT image reveals a round, solid mass, with heterogeneous attenuation, as well as internal calcifications, occupying most of the right ventricular chamber, due to heart metastasis from extraskeletal mesenchymal chondrosarcoma. It involves the right apex and almost two thirds of the ventricular septum, causing discrete bulging to the left.

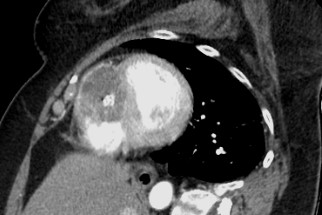
Figure 2: Coronal contrast-enhanced CT image shows the same round, solid mass, with heterogeneous attenuation, as well as internal calcifications, occupying most of the right ventricular chamber, in this image being more evident its apical location, as a result of heart metastasis from extraskeletal mesenchymal chondrosarcoma.
Discussion
Mesenchymal chondrosarcoma is an extremely rare neoplastic disease, comprising fewer than 2% of all chondrosarcomas, usually originating from bone or soft tissue, with an extraskeletal location in 30-50% of all cases .1,2Most commonly found in patients in their third decade, in contrast with conventional chondrosarcoma, which is more prevalent during the fifth to seventh decade of life,3 mesenchymal chondrosarcoma is associated with high incidence of distant metastasis, thus with poor prognosis.1,3
The standard therapy for heart metastasis should be surgery resection, as it aids with symptoms in addition to providing a histologic confirmation. Unfortunately, it is rarely possible, with chemotherapy and radiotherapy as the main options for these patients, often showing suboptimal efficacy.3
In this case we present a diagnosis of heart metastatic disease in a patient already under chemotherapy treatment, with no associated clinical manifestations, and for that reason remained with yearly follow up. Extraskeletal mesenchymal chondrosarcoma has a high risk of early dissemination, poor response to treatment and, consequently, it is associated with low rates of survival. Given the sparse therapeutic interventions, follow up with imaging studies is frequently recommended and local, as well as distant, recurrence should be actively searched by the Radiologist when evaluating patients with a clinical history of extraskeletal mesenchymal chondrosarcoma.3

