Imagens de Interesse
Abdominal Pain in a Female Adolescent: A Diagnosis to Consider
Dor Abdominal numa Adolescente: Um Diagnóstico a Considerar
1Department of Pediatrics, Unidade Local de Saúde de Trás-os-Montes e Alto Douro, Vila Real, Portugal
Abstract
OHVIRA syndrome is a rare congenital female anomaly, characterized by the triad: uterus didelphys, unilaterally obstructed hemivagina and ipsilateral renal agenesis. The authors present a case of a 12-year-old girl with cyclic abdominal pain, scarce catamenia and intense dysmenorrhea refractory to NSAIDs. An abdominal and pelvic computized tomography was carried out which revealed renal agenesis, duplication of the uterus, cervix, and vagina, and hematocolpos, suggesting vaginal obstruction. The prompt treatment allows a clear improvement in the clinical and reproductive prognosis, so the authors emphasize the importance of the knowledge and suspicion of this condition, allowing the diagnosis, referral, and early approach.
Keywords: Congenital defects; Diagnosis; Female genitourinary diseases; OHVIRA syndrome.
Resumo
A síndrome de OHVIRA é uma rara anomalia congénita feminina, caracterizada pela tríade: útero didelfo, hemivagina unilateral obstruída e agenesia renal unilateral. Os autores apresentam um caso de uma menina de 12 anos com dor abdominal cíclica, cataménio escasso e intensa dismenorreia refratária aos AINEs. Foi realizada uma tomografia computorizada que revelou uma agenesia renal, duplicação do útero, colo uterino e vagina, e hematocolpos a sugerir obstrução vaginal. O tratamento precoce permite uma melhoria significativa do prognóstico clínico e reprodutivo, por isso os autores realçam a importância do conhecimento e suspeita desta condição, permitindo um diagnóstico, referenciação e tratamento precoce.
Palavras-chave: Defeito congénito; Diagnóstico; Doenças genitourinárias femininas; Síndrome de OHVIRA.
Case
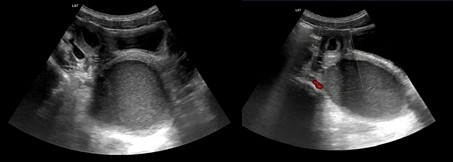
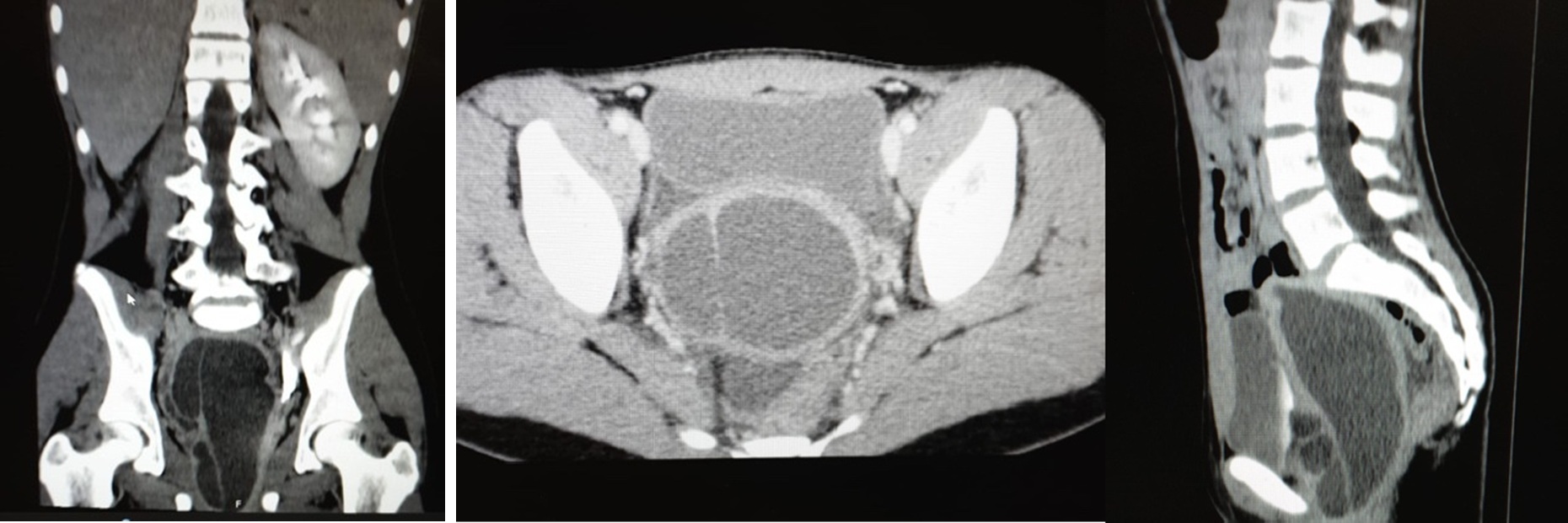
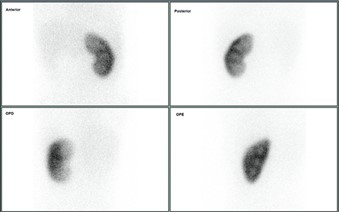
A 12-year-old girl, with an irrelevant medical history, was admitted to the pediatric emergency department with pollakiuria and abdominal and genital pain for two weeks, with worsening in the day before admission. There was a reference to menarche in the six months before, with scarce catamenia and intense dysmenorrhea refractory to NSAIDs. Last catamenia had been two weeks prior to the admission. On physical examination, the lower abdominal quadrants were rigid and painful on palpation and decompression, mainly in the right iliac fossa. An analytical study, urinalysis and pregnancy test were performed, all negative. Therefore, she did an abdominal ultrasound which suggested an hematocolpus (Fig. 1), but could not correctly evaluate the uterus. To better characterization, an abdominal and pelvic computized tomography was carried out which revealed the absence of the right kidney and retroaortic left renal vein, duplication of the uterus, cervix, and vagina, and marked distension of the right hemivagina and endometrial cavity, with hematocolpos, suggesting vaginal obstruction (Fig. 2). Afterwards, she did a renal scintigraphy for a renal morphofunctional assessment, which confirmed a right renal agenesis (Fig. 3). These findings allowed the diagnosis of an OHVIRA syndrome.
Discussion
OHVIRA syndrome is a rare congenital female anomaly, that results from an abnormal embryological development of the Mullerian and Wolffian ducts.1,2,3 It is characterized by the triad: uterus didelphys, unilaterally obstructed hemivagina and ipsilateral renal agenesis.1,2,3 This syndrome should be considered as a differential diagnosis in female adolescents with dysmenorrhea, abdominal pain, pelvic mass and/or inpatient retention, since it is the typical presention.1,2,3 Also, in female patients diagnosed with renal agenesis, these anomalies should be investigated, even in pre-pubertal stages.3 The prompt diagnosis and surgical treatment allow a clear improvement in the clinical and reproductive prognosis, avoiding late complications, such as endometriosis, pelvic adhesions, and infertility.1,2,3 Thus, we emphasize the importance of the knowledge and suspicion of this condition, allowing the diagnosis, referral, and early approach.
Acknowledgments
We thank the parents of the patient for giving us permission to publish the data.
References
1. Aydin R, Ozdemir AZ, Ozturk B, Bilgici MC, Tosun M. A rare cause of acute abdominal pain: herlyn-werner-wunderlich syndrome. Pediatr Emerg Care. 2014;30:40-42. https://doi:10.1097/0000000000000052.
[ Links ]
2. Del Vescovo R, Battisti S, Di Paola V, et al. Herlyn-werner-wunderlich syndrome: MRI findings, radiological guide (two cases and literature review), and differential diagnosis. BMC Med Imaging. 2012; 12:4. https://doi:10.1186/1471-2342-12-4.
[ Links ]
3. González Ruiz Y, Delgado Alvira R, Siles Hinojosa A, Izquierdo Hernández B, Rihuete Heras MÁ. Diagnóstico prepuberal del síndrome de OHVIRA: es posible? An Pediatr (Barc). 2019;90:244-245. https://doi.org/10.1016/j.anpedi.2018.04.010.
[ Links ]












 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink