











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
A female patient in her 70s with no other relevant past medical history presented to the emergency department with severe right upper quadrant pain. Laboratory tests revealed markedly elevated C-reactive protein and leucocytosis, with no significant liver function tests abnormalities.
A computed tomography (CT) was obtained. Non-contrast CT showed a linear high-density foreign body in the left lobe of the liver, next to the falciform ligament (Figure 1).
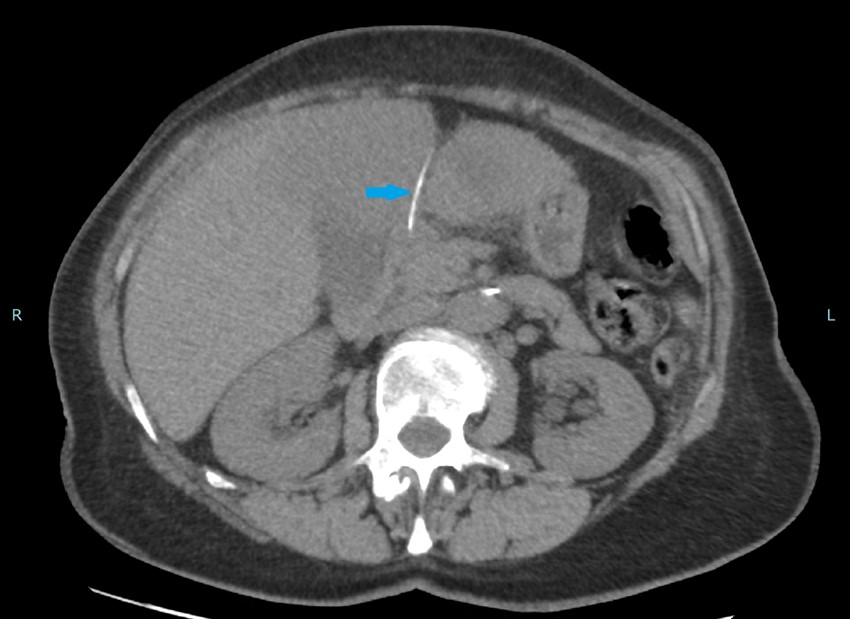
Figure 1: On non-contrast CT, a linear high-density foreign body compatible with a fish bone was identified in the left lobe of the liver, next to the falciform ligament (blue arrow).
This foreign body was compatible with a fish bone and was in close proximity with the pylorus. After intravenous (IV) contrast injection, a large abscess occupying the majority of the left lobe of the liver with 12 cm was seen (Figure 2). There were no signs of pneumoperitoneum.
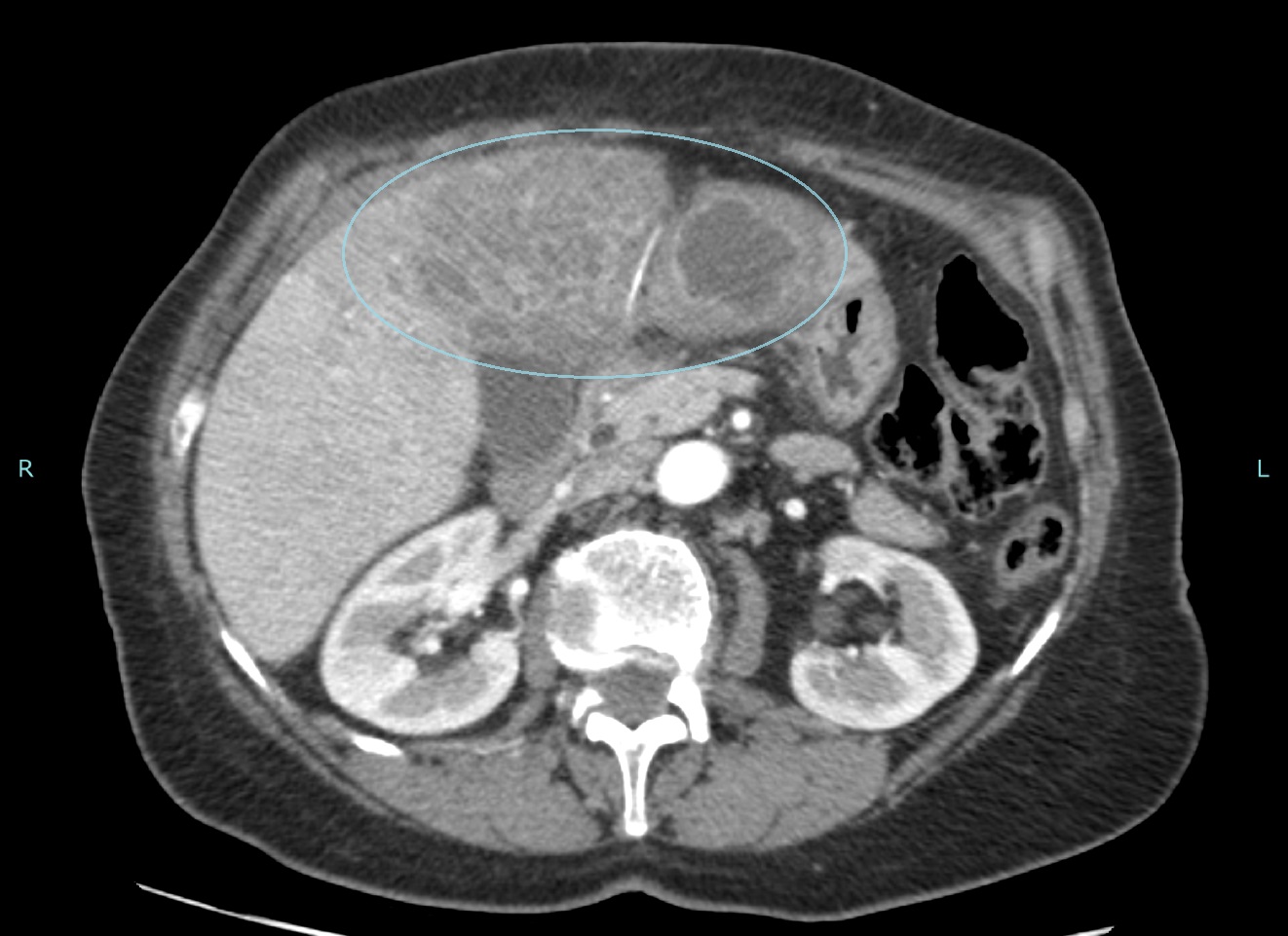
Figure 2: After IV contrast injection, a large abscess occupying the majority of the left lobe of the liver (blue circumference) was identified.
A percutaneous pigtail catheter was placed on the larger fluid collection on segment III of the liver, with drainage of most of the abscess. The drained pus was sent for bacterial culture, and it came positive for Streptococcus anginosus.
The patient received IV antibiotics and was discharged symptom-free after two weeks.
Follow-up CT revealed complete resolution of the abscess, with only mild heterogeneity near the falciform ligament of the liver, which was assumed to be residual (Figure 3). The fish bone remained unchanged.

Figure 3: Follow-up CT 2 months after showing complete resolution of the abscess, with only residual hypodensities next to the falciform ligament.
Foreign body ingestion is a common problem in clinical practice, affecting mostly the paediatric and elderly population, as well as those with oropharyngeal dysphagia. Most foreign bodies pass through the GI tract without issues, but about 1% can cause perforations, especially sharp ones like fish bones and toothpicks, making liver abscesses rare.1 When present, due to its anatomic location, they are more frequently encountered in the left lobe of the liver, as in this case.2
Pyogenic liver abscesses typically present with fever, upper right abdomen pain, and jaundice. However, these signs don't always occur together as patients often have nonspecific symptoms such as vague abdominal pain, fever, and vomiting. They usually don't remember swallowing anything unusual, requiring a high level of suspicion to make the diagnosis.2
Laboratory analyses are also non-specific, usually showing elevated inflammatory markers as well as elevated liver enzymes and bilirubin. The diagnosis usually relies on CT as the best diagnostic test, with a sensitivity as high as 90%, as it may also demonstrate the location of the foreign body, which typically appears as a hyperdense object within the gastrointestinal tract accompanied by surrounding soft tissue oedema or inflammation.3
The treatment of choice in these cases remains controversial, but usually include antibiotic therapy, percutaneous drainage and/or open surgery. Foreign body removal can be accomplished by endoscopy, percutaneously or by laparotomy, depending on the case and location of the foreign body.

