











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Hereditary Hemorrhagic Telangiectasia (HHT), also known as Osler-Weber-Rendu syndrome, is a rare autosomal dominant condition characterized by mucocutaneous telangiectasias and arteriovenous malformations (AVMs).1,2 These malformations can affect various organs, including the skin, lungs, gastrointestinal tract, brain, and liver, potentially leading to significant complications such as spontaneous bleeding, high-output cardiac failure, or portal hypertension.1,2
Hepatic involvement in HHT occurs in 44% to 74% of cases, although only a small proportion of patients develop clinical symptoms.3,4 One of the rare but severe hepatic complications is ischemic cholangiopathy, resulting from hemodynamic alterations induced by AV shunts.5,6 The resulting biliary ischemia can lead to a spectrum of complications ranging from bile duct necrosis and biloma formation to chronic biliary strictures and secondary biliary cirrhosis.5,7
Patients with biliary ischemia often present with fever and acute-phase responses, including elevated gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP), and C-reactive protein. In chronic phases, patients typically present with biochemical markers of cholestasis, and elevated conjugated bilirubin. These changes reflect progressive biliary obstruction and liver dysfunction.5,7 Jaundice normally occurs in cases with extensive liver involvement.3,4 Imaging modalities such as computed tomography (CT), magnetic resonance imaging (MRI), and ultrasound (US), play a critical role in the diagnosis and characterization of ischemic cholangiopathy.7,8
This article presents a clinical case of ischemic cholangiopathy in a patient with HHT, emphasizing the importance of imaging in diagnosing and monitoring this rare condition.
Case Presentation
We report the case of a 60-year-old female with no relevant personal or family history suggestive of HHT, who repeatedly presented with upper right quadrant abdominal pain. Initial laboratory tests were inconclusive, showing nonspecific alterations in hepatocellular and cholestatic patterns, which prompted further diagnostic investigation.
Abdominal ultrasound revealed a dysmorphic liver with left and caudate lobes hypertrophy, lobulated contours, and significantly heterogeneous parenchyma, consistent with chronic liver disease. Multiple rounded hyperechoic areas were identified within the parenchyma. The hepatic artery was notably dilated, measuring 10 mm in diameter, with increased peak systolic velocities (>150 cm/s) and a reduced resistive index (0.48) on Doppler spectral analysis, indicative of hemodynamic alterations caused by arteriovenous shunting (Figure 1).
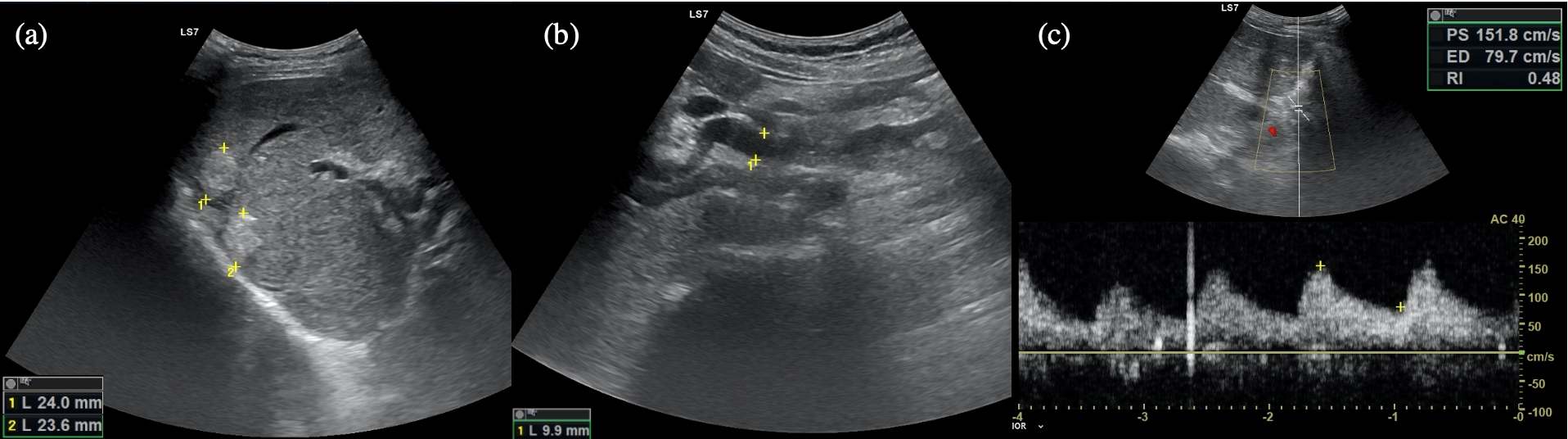
Figure 1: Abdominal ultrasound: (a) Hyperechoic nodular areas, corresponding to biliary lakes/bilomas with echogenic biliary debris. (b) Dilated hepatic artery measuring 10 mm in diameter, (c) demonstrating increased peak systolic velocity (PS > 150 cm/s) and a reduced resistive index (0.48) in Doppler spectral analysis, indicative of hemodynamic alterations caused by arteriovenous shunts.
CT scans also revealed numerous AVMs, early filling of hepatic veins during the arterial phase, and parenchymal perfusion changes, consistent with HHT hepatic involvement. The rounded hyperechoic areas identified on ultrasound corresponded to hypodense nodular regions on CT, lacking enhancement on post-contrast images, consistent with bilomas (Figure 2).
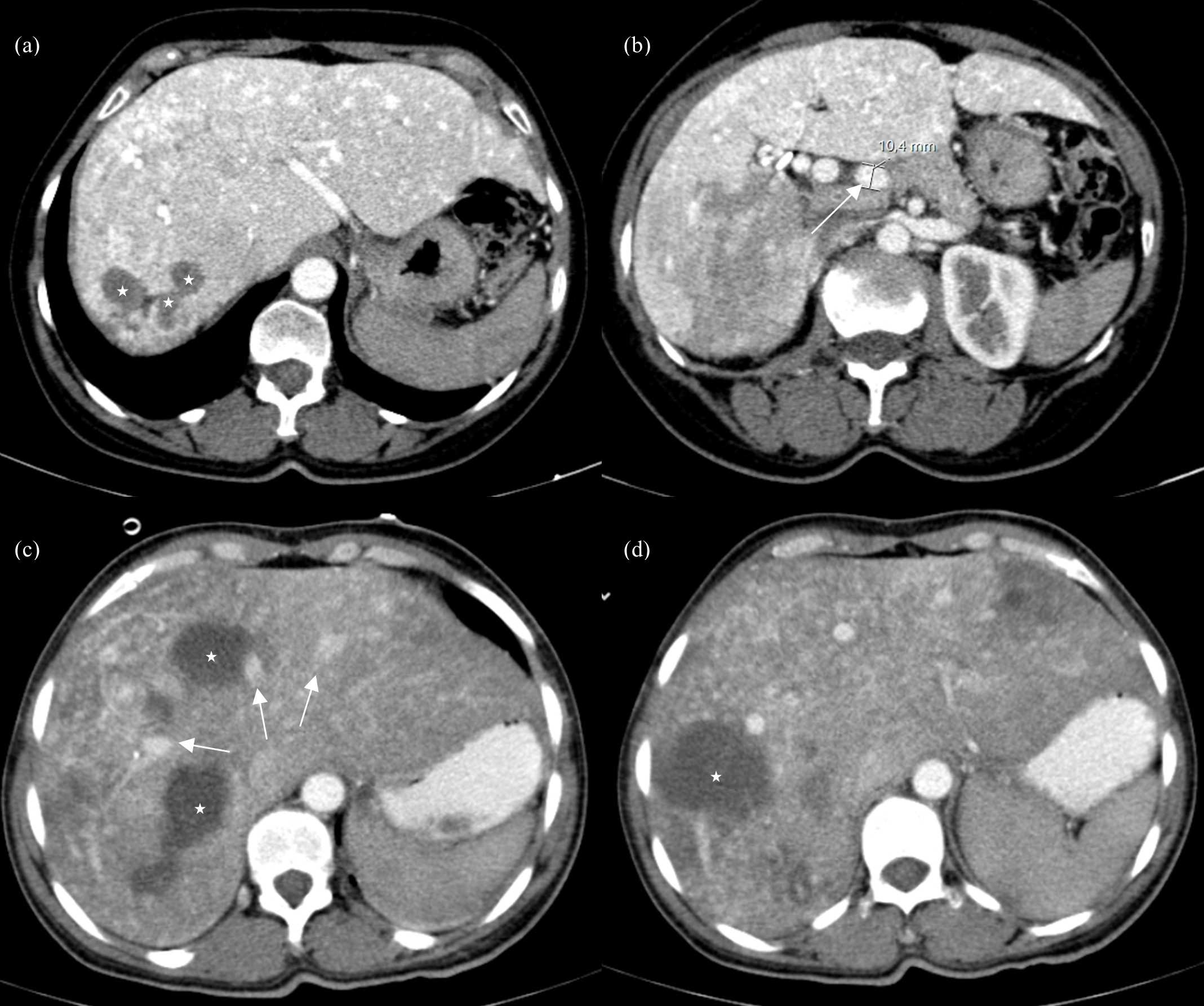
Figure 2: Arterial phase axial CT images showing a liver with features of chronic hepatopathy and multiple AVMs. (a) Hypodense nodular areas consistent with biliary lakes/bilomas (stars). (b) Dilated hepatic artery measuring 10 mm in diameter (arrow) and perfusion changes in the right lobe. (c, d) On a prior examination performed several years earlier, larger bilomas are evident, appearing hypodense with poorly defined margins (stars). Early enhancement of hepatic veins is also observed, consistent with arteriovenous shunting (arrows).
MRI further corroborated these findings, demonstrating peripheric segmental intrahepatic biliary dilatation adjacent to these lesions (Figure 3).
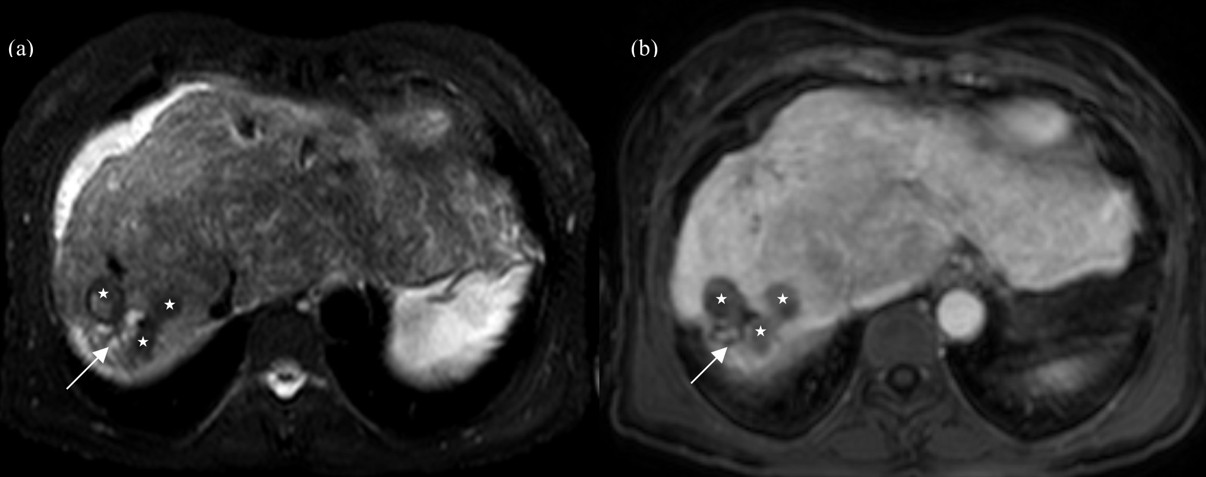
Figure 3: Abdominal MRI. T2-weighted image, with fat saturation (a) and dynamic study in the portal phase (b). The liver shows signs of chronic hepatopathy. The bilomas appear as nodular lesions with heterogeneous signal, predominantly hypointense on T2, with hyperintense areas, without enhancement on post-contrast dynamic study (stars). Mild ectasia of the intrahepatic bile ducts upstream of the bilomas is also observed (arrows).
Notably, the patient did not exhibit typical symptoms of HHT, such as epistaxis or visible telangiectasias, commonly associated with the condition. However, subtle findings such as labial telangiectasias and scattered cutaneous hemangiomas were identified upon closer physical examination and reassessment.
These clinical and imaging findings raised suspicions of HHT, leading to genetic testing. The test confirmed the presence of a heterozygous mutation in the ACVRL1 gene, a known genetic marker for HHT, thus supporting the diagnosis of this complex vascular disorder.
The patient was managed conservatively, with regular follow-ups and imaging studies to monitor progression. Her clinical status remained stable throughout the observation, with no immediate need for interventional procedures.
Discussion
Diagnostic Criteria for HHT
HHT is diagnosed clinically based on the Curaçao criteria, which include: (1) spontaneous and recurrent epistaxis, (2) multiple mucocutaneous telangiectasias at characteristic sites (e.g., lips, oral cavity, fingers, and nose), (3) visceral involvement (e.g., AVMs in the liver, lungs, or brain), and (4) a first-degree relative with HHT.1,2 Diagnosis is definite if three or more criteria are met, possible if two criteria are present, and unlikely with less than two criteria. Genetic testing for mutations in ENG, ACVRL1, or SMAD4 confirms ambiguous cases and elucidates the pathophysiological basis of HHT, which involves disruptions in TGF-signaling, leading to aberrant vascular development.9
Hepatic Manifestations and Pathophysiology of Ischemic Cholangiopathy
Hepatic involvement in HHT manifests as vascular malformations and arteriovenous shunts. These shunts, categorized as arterio-systemic, arterio-portal, and portosystemic, can lead to high-output cardiac failure, portal hypertension, and ischemic complications within the liver.3,4
Ischemic cholangiopathy arises from impaired arterial perfusion to the bile ducts, which rely exclusively on the hepatic artery for oxygenation. The diversion of blood flow through arteriovenous shunts reduces perfusion to the peribiliary plexus, leading to ischemia. This can manifest as bile duct and peribiliary tissue necrosis and fibrosis, focal biliary duct dilatations, and may progress to biliary perforation. In severe cases, biliary necrosis causes significant bile extravasation into the surrounding hepatic parenchyma, forming bilomas. Over time, chronic ischemic injury can result in biliary strictures and secondary biliary cirrhosis, further impairing liver function.5,6,7
Imaging Features of Hepatic Involvement in HHT
Ultrasound with Doppler evaluation is an essential first-line tool for detecting liver AVMs in HHT and assessing hepatic involvement. It allows localization of vascular malformations and evaluation of blood flow dynamics.8
Key ultrasound findings include dilation of the proper hepatic artery (> 5 mm) and increased peak systolic velocity (> 80 cm/s), indicating vascular shunting. A low resistive index (RI < 0.55) in the hepatic artery reflects increased blood flow during diastole due to shunting. Additional features include 'arterialization' of venous waveforms and turbulent flow in the portal vein, which are characteristic of arteriosystemic or arterioportal shunts, respectively.3,8
On ultrasound, bilomas typically appear as anechoic or hypoechoic fluid collections, although in cases of biliary necrosis or debris, they may exhibit internal echoes or heterogeneous echotexture.5,6,7
CT and MRI offer a more comprehensive evaluation of hepatic involvement. AVMs may be focal or diffuse. These rounded, hypervascular lesions are usually sub-centimetric and appear as focal hyperenhancing lesions during the arterial phase, becoming isoattenuating or isointense on delayed phase acquisitions. Over time, AVMs may enlarge or coalesce, forming more complex vascular malformations or vascular masses. As a result, their hemodynamic impact can become more pronounced, leading to increased arteriovenous shunting.1,2,3,8 This progressive hemodynamic alteration is particularly relevant in HHT, where arteriovenous shunts (hepatic artery to hepatic vein) are the most frequent vascular shunts. These are best visualized during the arterial phase, showing early enhancement of hepatic veins. Arterioportal shunts (hepatic artery to portal vein) result in early enhancement of the portal vein during the arterial phase. Portovenous shunts (portal vein to hepatic vein) are less common and may be identified during the portal venous phase, showing direct communication between a portal vein branch and a hepatic vein.1,3,4,8
Additional hepatic findings may include benign regenerative nodules, often resembling FNH-like lesions on imaging. These nodules can mimic AVMs on contrast-enhanced imaging; however, hepatobiliary phase acquisitions using hepatospecific contrast agents can help differentiate between the two.8
Biliary lakes present as hypodense fluid collections on CT, typically with poorly defined margins and lacking a distinct wall or capsule. These findings represent a combination of dilated ischemic bile ducts and bilomas, often indistinguishable from necrotic peribiliary tissue and debris. In cases complicated by infection, bilomas may evolve into hepatic abscesses with wall enhancement on imaging. In chronic cases of biliary ischemia, the peribiliary fluid collections may become smaller and their margins with liver parenchyma better defined. The peripheral bile ducts can be dilated in the affected segment due to compression by necrotic peribiliary tissue or bile duct strictures.5,6,7
On MRI, bilomas appear as circumscribed T2-weighted hyperintensities that can have fluid-fluid levels or contain debris. Chronic ischemic injury to the biliary tree manifests as a "beaded" appearance of the bile ducts on cholangiography, characterized by alternating strictures and dilatations.5,6,7
The biliary lakes in this case exhibited distinct imaging characteristics. On ultrasound, they appeared as rounded hyperechoic areas, and on MRI, they displayed heterogeneous rather than uniformly hyperintense signal on T2-weighted sequences, likely due to sloughing of the biliary epithelium or solidified debris. CT imaging revealed that, over time, the bilomas became smaller, with increased densities and better-defined margins.
The imaging features, combined with the temporal evolution of bilomas, along with the associated vascular abnormalities, were crucial in confirming the diagnosis of ischemic cholangiopathy in the context of HHT.
Clinical and Therapeutic Implications
Patients with ischemic cholangiopathy often present with right upper quadrant pain, fatigue, and cholestatic biochemical profiles. The biliary phenotype may mimic other conditions, such as sclerosing cholangitis or Caroli’s disease.5,6,7,8 Management includes antibiotics for superimposed infections and interventional procedures such as biliary stenting or drainage for advanced cases. In cases of refractory disease, liver transplantation remains the definitive treatment.3,4,10 Emerging therapies, such as Bevacizumab, an anti-angiogenic agent, have demonstrated efficacy in reducing AV shunting and alleviating symptoms in severe cases of HHT-related complications, including ischemic cholangiopathy.11
Conclusion
This case highlights the essential role of imaging in diagnosing and monitoring Hereditary Hemorrhagic Telangiectasia, as well as in identifying its complications, particularly, ischemic cholangiopathy. The presence of biliary lakes exemplifies the intricate interplay between vascular and biliary abnormalities in this condition. A multimodal imaging approach is not only essential for early diagnosis, but also crucial for detecting systemic involvement beyond the hepatobiliary system, assessing potential complications and guiding therapeutic strategies.

