











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
The placement of central venous catheters (CVC) is a widely used clinical practice in critical care, anesthesia, and other medical fields for hemodynamic monitoring, drug administration, and nutritional support. Although considered a relatively safe procedure when performed by trained professionals, complications can arise, including improper insertions or mispositioning.1
The atypical placement of a CVC in the pulmonary venous system is an extremely rare complication, often associated with vascular anomalies or technical errors. Congenital malformations may alter the usual configuration of the vascular system, diverting the catheter from its expected trajectory and leading to its insertion into unintended structures, such as the pulmonary veins.2,3,4
This case report describes a rare instance of a central venous catheter malpositioned into the left superior pulmonary vein due to a congenital anomaly - partial anomalous pulmonary venous drainage (PAPVD). This anomaly results in a left-to-right shunt, explaining why arterial blood was aspirated from the catheter. The discussion highlights the importance of recognizing such anomalies, the imaging techniques required for accurate diagnosis, and potential clinical implications of catheter malposition.
Case-Description
A 70-year-old male patient with end-stage renal disease on regular hemodialysis (HD) presented to the hospital due to irrecoverable thrombosis of his vascular access, requiring the placement of a central venous catheter for HD.
An attempt was made to place a long-term catheter in the right internal jugular vein, but the guidewire could not progress beyond 7-8 cm.
A subsequent attempt was made to place a temporary CVC in the left internal jugular vein under ultrasound guidance. The vein was successfully punctured without complications, but guidewire advancement was challenging at 10-15 cm, presumably due to venous stenosis at that site. Nevertheless, the catheter was advanced.
During the procedure, oxygenated blood was aspirated from both lumens, confirmed by arterial blood gas analysis. A chest X-ray revealed the CVC on the left hemithorax. No signs of iatrogenic complications such as pneumothorax, hemothorax, or tracheal deviation were observed (Fig. 1). The patient remained hemodynamically stable throughout the procedure.
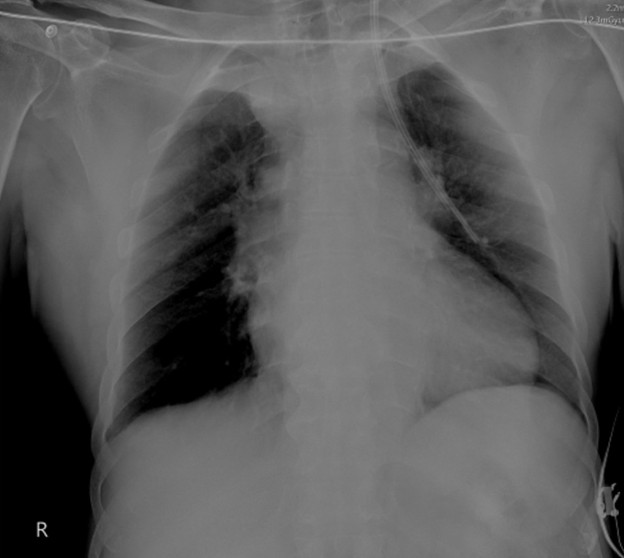
Figure 1: Chest X-ray revealed the CVC on the left hemithorax. No signs of other iatrogenic complications were observed, such as pneumothorax, hemothorax, or tracheal deviation.
Given these findings, the catheter was not used.
A tunneled hemodialysis CVC was placed in the right femoral vein without complications.
Vascular Surgery was contacted and recommended a thoracic and cervical CT. Promptly, a cervical and thoracic CT scan was acquired, which revealed the following:
The left superior pulmonary vein drains into the left brachiocephalic vein, consistent with a congenital anomaly classified as partial anomalous pulmonary venous drainage (PAPVD).
The left-sided CVC was noted entering the left internal jugular vein, descending through the left brachiocephalic vein, and subsequently passing into the left superior pulmonary vein, with its distal tip located in an anterior segmental venous branch of the superior lobe of the left lung. No active contrast extravasation from arterial or venous sources was observed (Fig. 2a, 3, 4).
There was slight soft tissue densification around the left internal jugular vein at the catheter entry site, likely related to puncture attempts.
The right internal jugular vein showed a contrast-filling defect extending approximately 5 cm, involving its most caudal portion but sparing the confluence with the subclavian vein, consistent with thrombosis (Fig. 5).
No pneumothorax (Fig. 2b), pleural effusion, or pericardial effusion was observed (Fig. 3).
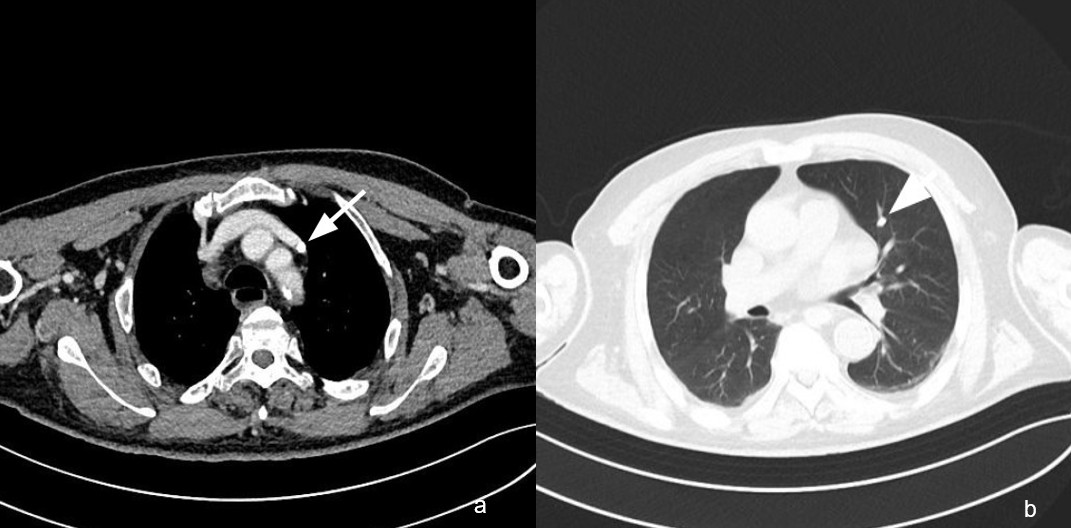
Figure 2: a) - Axial CT scan with soft tissue window showing the catheter entering the left superior pulmonary vein (arrow) that drains into the left brachiocephalic vein. b) - Axial CT scan with lung window showing the catheter in the left superior pulmonary vein (arrow) inside the superior lobe of the left lung. No pneumothorax or lung consolidation is present.

Figure 3: Coronal CT scan with soft tissue window showing the trajectory of the catheter entering the left jugular vein and then the left superior pulmonary vein (straight arrow). An additional anatomical variant is noted, characterized by a common origin of the right brachiocephalic trunk and the left common carotid artery, commonly referred to as a bovine arch (curved arrow).

Figure 4: 3D reconstruction showing the trajectory of the catheter entering the left internal jugular vein (LIJV) and then the left superior pulmonary vein (LSPV).
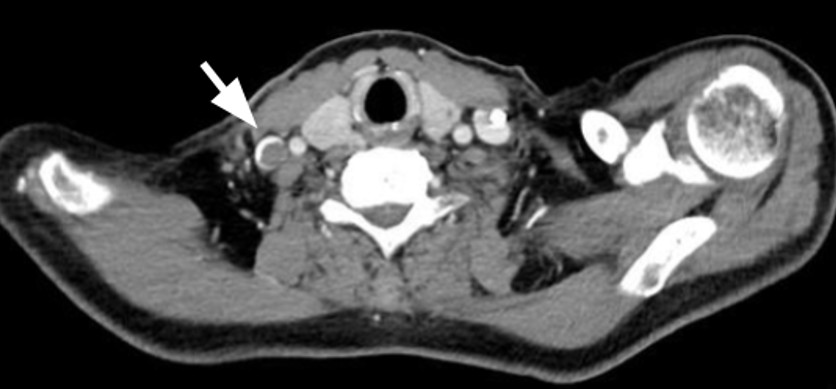
Figure 5: The right internal jugular vein shows a contrast-filling defect consistent with thrombosis (arrow). The catheter can be seen in the lumen of the left internal jugular vein.
After the diagnosis was confirmed by CT, the CVC in the left internal jugular vein was removed without complications.
The placement of a long-term dialysis catheter (LDC) in the left internal jugular vein was scheduled for the following week under fluoroscopic guidance and was performed without complications.
Despite the presence of a left-to-right shunt, the patient remained asymptomatic, with no reports of dyspnea, chest pain, or palpitations. Further evaluation by the cardiology team, including standard diagnostic tests such as echocardiography with Doppler and pulmonary artery pressure measurement, revealed no evidence of pulmonary hypertension.
Additionally, the CT scan revealed an anatomical variant with a common origin of the right brachiocephalic arterial trunk and the left common carotid artery (bovine arch).
Discussion
Central venous access is essential in patients with advanced chronic kidney disease; however, anatomical anomalies can hinder proper catheter placement, leading to unexpected complications.3,5,6
The misplacement of a CVC is an uncommon but clinically significant complication. In this case, arterialized blood aspiration was the first indication of an anomalous trajectory. The radiographic evaluation revealed CVC misplacement in the left hemithorax.
The radiographic appearance of the misplaced catheter, initially suggesting intrapulmonary positioning or the presence of a large-caliber vessel lateral to the aortic arch on chest radiography, hypotheses such as intra-arterial placement or extravascular positioning in the mediastinum or pleural space were not primarily considered, given that the procedure was ultrasound-guided and no immediate complications occurred during catheter insertion, which raises four main differential diagnoses:
Persistent left superior vena cava, a true anatomical variant with normal drainage into the right atrium via the coronary sinus.
Superior intercostal vein.
Levo-atrial cardinal vein, a vertical vessel connecting the left brachiocephalic vein to the left atrium.
Partial anomalous pulmonary venous drainage (PAPVD) of the left superior pulmonary vein, as seen in this case.
Imaging studies, particularly CT, are crucial in distinguishing these entities.
Persistent Left Superior Vena Cava (PLSVC)
A persistent left superior vena cava is the most common thoracic venous anomaly, occurring in approximately 0.3-0.5% of the general population and up to 10% in patients with congenital heart disease. It results from the failure of regression of the left anterior cardinal vein during embryonic development. Typically, a PLSVC drains into the right atrium via the coronary sinus, maintaining normal venous return without hemodynamic consequences. However, in rare cases, it may drain directly into the left atrium, leading to a right-to-left shunt and potential cyanosis. Imaging findings on contrast-enhanced CT or MRI include a prominent venous structure coursing along the left mediastinum, descending anterior to the aortic arch, and draining into the coronary sinus. Differentiation from pathological vascular anomalies is crucial, as a PLSVC is usually an incidental finding with minimal clinical significance.1,4
Superior Intercostal Vein
The superior intercostal vein is a normal venous structure that drains the upper intercostal spaces and empties into either the azygos vein (on the right) or the left brachiocephalic vein (on the left). On imaging, it may appear as a prominent vessel lateral to the aortic arch, potentially mimicking a vascular anomaly. However, its anatomical course, small caliber, and typical connection to the azygos-hemiazygos system help differentiate it from congenital anomalies such as PLSVC or partial anomalous pulmonary venous drainage. Recognition of this structure is important to avoid misinterpretation, particularly in cases where atypical vascular findings are present on chest radiography or CT.1,3
Levo-atrial Cardinal Vein
The levo-atrial cardinal vein is a rare congenital anomalous connection between the left atrium and the systemic venous system, classically described in association with severe left heart obstruction, particularly mitral atresia and interrupted aortic arch. In these contexts, it is usually regarded as a collateral pathway that allows pulmonary venous decompression and attenuation of severe pulmonary venous hypertension, especially when the interatrial communication is small, restrictive, or absent. The direction of flow through this vessel is not fixed and depends on the underlying anatomy and pressure gradients. While left-to-right shunting (from the left atrium to the systemic veins) is most commonly observed in neonates with obstructive left heart lesions, right-to-left shunting has also been reported, particularly in isolated cases diagnosed in adulthood, potentially leading to arterial desaturation and paradoxical embolism. Flow orientation should be assessed using advanced imaging techniques such as Doppler echocardiography, CT angiography, or cardiovascular MRI. It is also important to differentiate this anomaly from a persistent left superior vena cava draining into the left atrium, as both may present with systemic-to-pulmonary venous communications but have different embryological origins and clinical implications.1,3,6,7
Partial Anomalous Pulmonary Venous Drainage
Partial anomalous pulmonary venous drainage is a congenital vascular anomaly in which one or more-but not all-pulmonary veins fail to connect to the left atrium, instead draining into systemic veins, such as the superior vena cava, brachiocephalic vein, or azygos vein. This anomaly results in a left-to-right shunt, which can be asymptomatic or lead to right heart overload, depending on the shunt volume. In this case, the left superior pulmonary vein was found to be draining into the left brachiocephalic vein, leading to an unusual trajectory of the central venous catheter. PAPVD can be associated with atrial septal defects, particularly the sinus venosus type, and may require surgical correction if significant shunting occurs. Imaging with contrast-enhanced CT or MR angiography is crucial for diagnosis and preoperative planning.1,6
In this patient, CT imaging confirmed PAPVD, explaining the catheter misplacement. The CT scan confirmed that the catheter did not contact the pulmonary or systemic arteries and that the catheter remained entirely intraluminal, with no vessel perforation.
Clinically, CVC malposition in a pulmonary vein can lead to complications such as systemic embolization, volume overload, and misinterpretation of hemodynamic readings.
This case describes a rare but clinically significant instance of a central venous catheter being inadvertently placed in the left superior pulmonary vein due to partial anomalous pulmonary venous drainage. Unlike a simple anatomical variant, PAPVD is a congenital anomaly that results in a left-to-right shunt. This explains why the catheter aspirated oxygenated blood, as the pulmonary vein carries arterialized blood from the lungs to the systemic circulation.3,4
Computed tomography (CT) played a crucial role in both the diagnosis and clinical management of this case. While the initial chest X-ray suggested an abnormal catheter position in the left hemithorax, it was not sufficient to determine the exact location of the catheter tip or the underlying anatomical anomaly. The CT scan provided a detailed visualization of the vascular structures, confirming that the catheter had inadvertently entered the left superior pulmonary vein due to an anomalous pulmonary venous drainage pattern. This precise identification allowed for an informed clinical decision to remove the catheter safely, avoiding potential complications such as systemic embolization or inadvertent arterial catheterization. Thus, CT imaging was essential not only for establishing the definitive diagnosis but also for guiding the appropriate management strategy.8
In this case, guidewire advancement difficulties on the right side were explained by confirmed internal jugular vein thrombosis. On the left side, the challenge likely arose from the catheter entering the left superior pulmonary vein instead of following the expected route into the superior vena cava. This highlights the need for careful navigation and awareness of potential anatomical anomalies during CVC placement.
From a clinical perspective, the presence of a misplaced catheter in the pulmonary venous system may have significant implications. Aspiration of arterial blood should prompt immediate reevaluation of catheter positioning, as it may indicate an anomalous venous connection, as observed in this case. The use of CT was essential for the final diagnosis, confirming the atypical placement of the catheter, preventing potential complications, and guiding clinical management.
Although the patient had a left-to-right shunt, he did not exhibit any symptoms related to it, he had no dyspnea, chest pain, or palpitations. He was later evaluated by the cardiology team, and standard tests, echocardiography with Doppler and assessment of pulmonary artery pressure, confirmed the absence of pulmonary hypertension.
Conclusion
This case highlights the importance of recognizing congenital vascular anomalies, such as partial anomalous pulmonary venous drainage, as potential causes of CVC misplacement. Awareness of these anomalies, combined with advanced imaging techniques, is essential for ensuring patient safety and optimizing vascular access procedures.

