











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Case Report
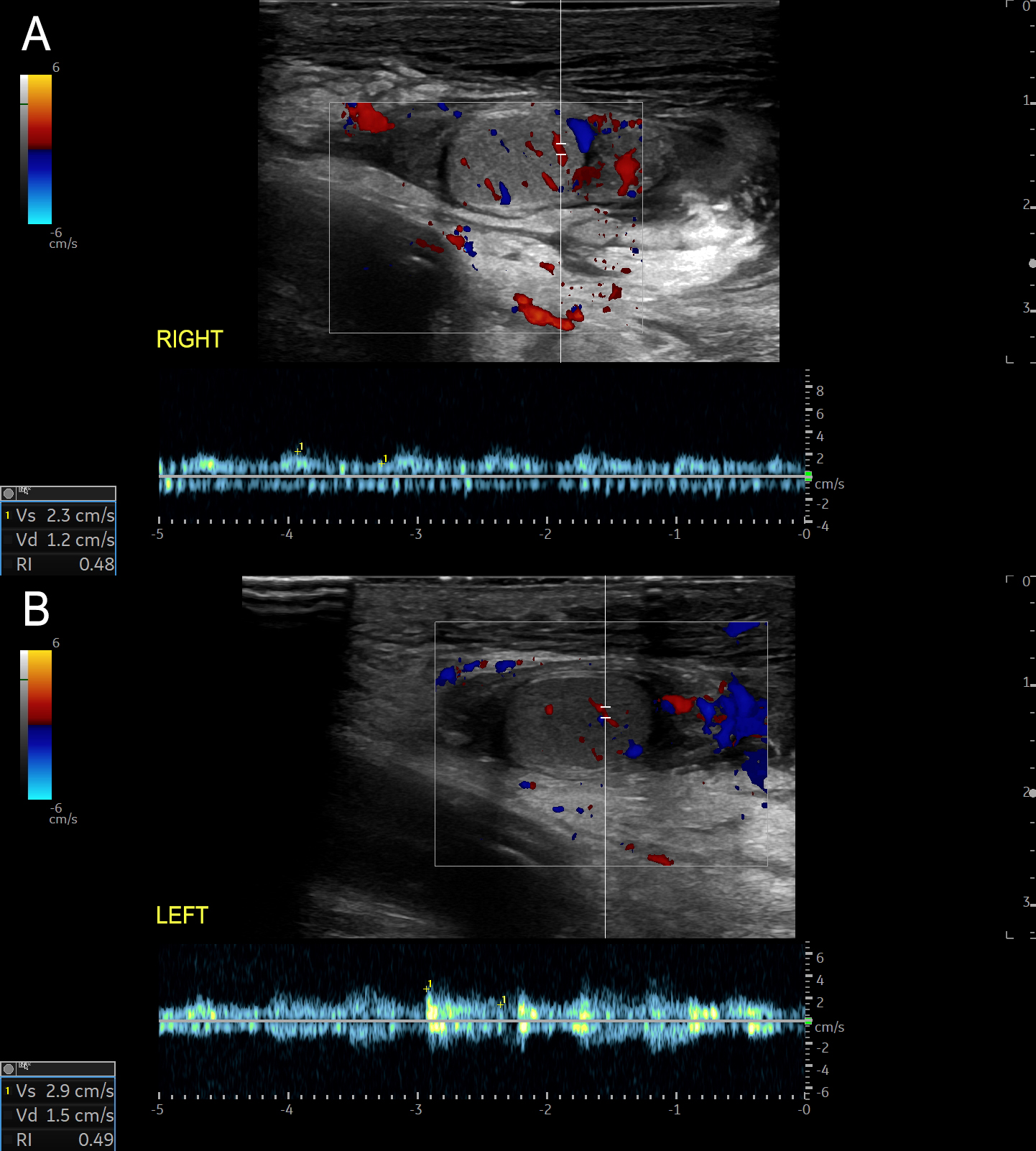
A 7-year-old boy, with no significant medical history, was admitted with complicated acute appendicitis and underwent an appendectomy. Two days after surgery, he developed painless, marked scrotal swelling. Physical examination revealed significant scrotal edema and erythema without tenderness. Ultrasound (US) showed diffuse hypoechoic thickening of the scrotal wall and pronounced subcutaneous edema, while the testes and epididymis appeared normal (Figure 1). Doppler imaging demonstrated marked bilateral hypervascularity in the scrotal wall, including the "fountain sign" (Figure 2), with normal intratesticular blood flow (Figure 3). These findings were consistent with acute idiopathic scrotal edema (AISE). The patient was managed conservatively with anti-inflammatory and antihistamine medication. The edema entirely resolved after four days, and a follow-up US confirmed the resolution of hypervascularity and edema.
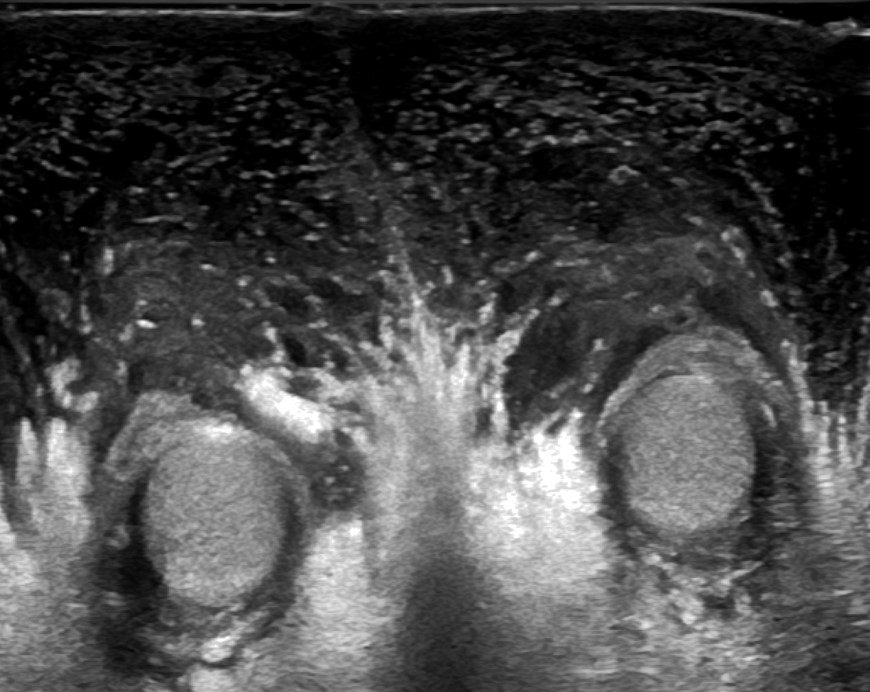
Figure 1: Transverse US scan showing diffuse thickening of the scrotal wall and pronounced subcutaneous edema, with unremarkable testes and epididymis.
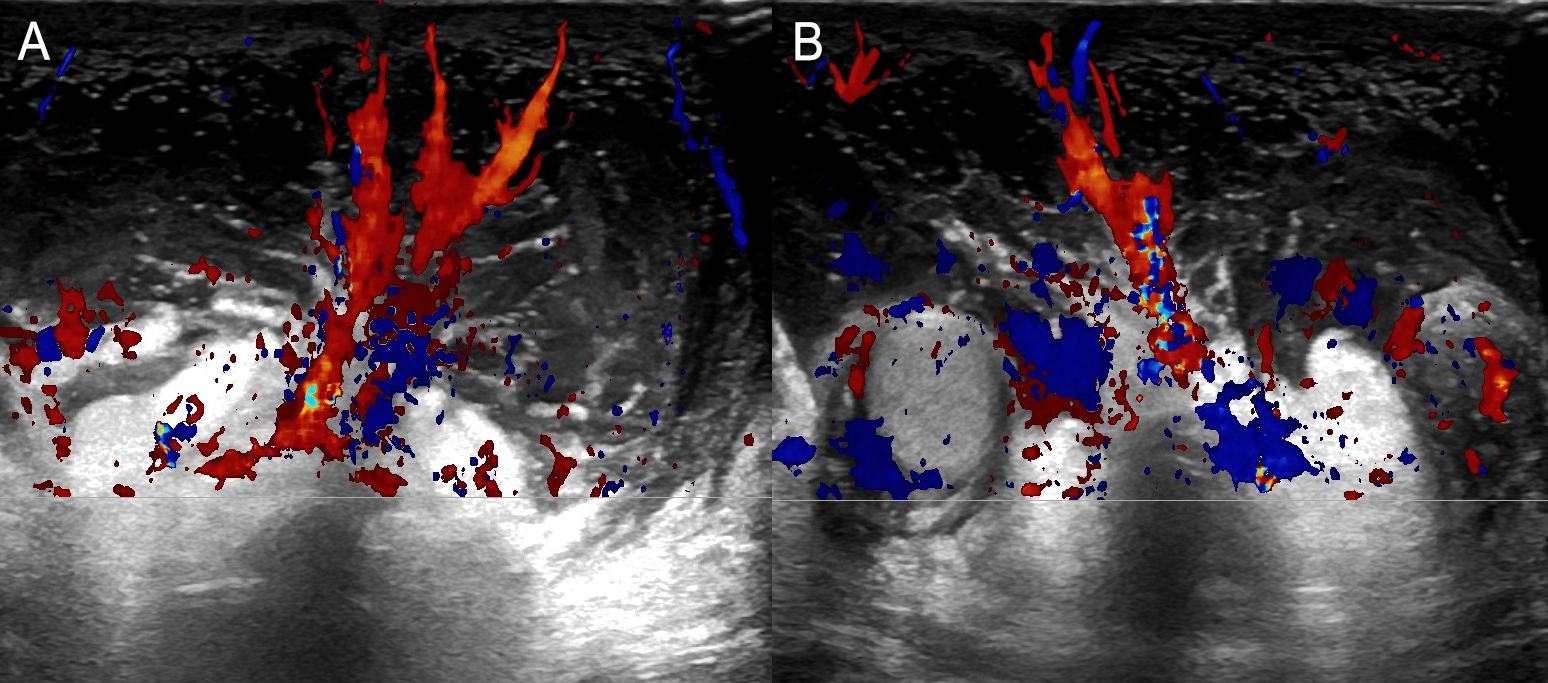
Figure 2: Transverse Color Doppler scans (A and B) showing the "fountain sign" (increased scrotal wall blood flow, resembling a colored fountain).
Discussion
AISE is a self-limiting condition primarily affecting boys under the age of 10 years old, accounting for about 10% of acute scrotum cases in children and adolescents.1 Although its etiology remains unclear, AISE is generally thought to involve an exaggerated inflammatory response, related to a variant of angioneurotic edema, leading to significant edema of the scrotal skin and dartos fascia.1,2 The condition is usually painless and is characterized by sudden-onset scrotal swelling and redness without involvement of the deeper layers, testes, or epididymis.1,2,3 Bilateral involvement is the usual presentation but unilateral AISE is described with variable occurrence rates in the literature.1,3
From a radiological perspective, the diagnosis of AISE is often established using US, which is the modality of choice due to its non-invasive nature and high sensitivity for scrotal pathology.2 US findings typically include diffuse thickening of the scrotal wall and marked subcutaneous edema, with unremarkable testes and epididymis.1,2 Doppler imaging can further confirm the absence of testicular torsion by demonstrating normal intratesticular blood flow.3 A distinctive feature observed on Doppler imaging in AISE is the "fountain sign", characterized by hypervascularity in the scrotal skin and dartos fascia, due to increased flow in the anterior and posterior scrotal arteries.3 This sign is considered a hallmark of AISE. It helps to differentiate it from other causes of acute scrotal swelling, such as epididymitis, orchitis, torsion of the appendix testis or testicular torsion, which usually present with more severe clinical symptoms and abnormal testicular findings on imaging.3
The management of AISE is conservative, primarily focusing on observation and symptomatic relief, such as anti-inflammatory medication and scrotal elevation.2 The condition typically resolves spontaneously within a few days to a week, as shown by the complete resolution of symptoms and imaging findings returning to normal, as demonstrated in our case report. Early and accurate diagnosis of AISE is crucial to avoid unnecessary surgical exploration, which may be considered in cases of acute scrotal swelling due to the potential for more serious underlying conditions, and this case underscores the key role of imaging in diagnosis and management.2
Conclusion
AISE should be considered in the differential diagnosis of acute scrotal swelling, particularly in young pediatric patients, when imaging reveals normal testes and epididymis and the characteristic "fountain sign" on Doppler imaging. Radiologists play a key role in diagnosing and managing this condition, ensuring appropriate treatment and avoiding unnecessary surgical interventions.

