











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Computed Tomography (CT) is essential in the diagnosis, management, and prognosis of patients in emergency departments (EDs), by providing rapid and high-quality information that supports clinical decision-making. This imaging modality is increasingly available and utilised; for instance, across the three hospital units of Trás-os-Montes e Alto Douro (Lamego, Chaves and Vila Real), a total of 36,610 CT scan exams were performed exclusively in emergency settings in 2023, rising to 38,059 in 2024, as verified through local ByMe bHealth Flow.
However, concerns have been raised regarding the appropriateness of this substantial volume of requests, due to both clinical risks and financial implications, particularly in resource limited EDs. Unjustified imaging exposes patients to unnecessary ionising radiation, increasing the risk of malignancy, particularly in children, and potentially contributing to up to 5% future cancers, as suggested recently by Rebecca Smith-Bindman et al. In addition, the potential use of contrast agents can also pose additional risks, including allergic reactions and acute kidney injury. Furthermore, excessive imaging not only increases healthcare costs but may also reduce the time available for image interpretation, potentially compromising the quality of radiological reports.1,2,3,4,5
To address this issue, several decision-support tools have been developed to guide imaging requests in various clinical scenarios, assisting physicians and reducing overuse. Notable examples include the American College of Radiology (ACR) Appropriateness Criteria and the European Society of Radiology guidelines (ESR iGuide). In Portugal, the Directorate-General of Health (DGS) has also issued some guidelines and normative circulars (NOCs) that provide additional support.6,7,8
This study aims to assess the appropriateness of CT scan requests in the basic emergency department of Lamego Hospital and correlate with imaging findings.
Methods
Study Design: This retrospective cross-sectional study was conducted at the Unidade Local de Saúde de Trás-os-Montes e Alto Douro (ULSTMAD), EPE, Vila Real, Portugal. A total of 360 CT exams were randomly selected for data collection from a total sample of 5500 requested in the basic emergency department of Lamego from January to December 2023. All selected exams had been requested by an attending physician.
This study was reviewed and approved by the Ethics Committee and Data Protection Officer of ULSTMAD and complies with all principles of the Declaration of Helsinki and applicable legislation.
Data collection and variables: Patient and CT Scan data were extracted from ByMe bHealth Flow into an Excel database. The selection process was conducted using a computer-generated randomization algorithm to prevent selection bias. A random seed was obtained by using the set.seed and sample R functions. The seed obtained was 1574 and the sample R function without replacement was used to randomly pick the 360 CT exams to be used for this study. All of them contained relevant and sufficient clinical information for analysis; lack of adequate clinical information would have constituted an exclusion criterion. A total sample of 360 provides at least 10% precision to estimate the rate of inappropriate CT scans which was deemed adequate for this study.
The variables collected comprised: (1) patient demographics (age and sex); (2) clinical data (presenting clinical information and Manchester Emergency Triage level at admission); (3) examination characteristics (CT anatomical region, relative radiation level, ESR iGuide appropriateness rating, and final appropriateness assessment); (4) prescriber characteristics (medical specialty); and (5) imaging findings (as detailed below).
CT scan appropriateness was determined based on ESR guidelines (ESR iGuide), applicable NOCs, and the expertise of two different certified radiologists; a third radiologist was consulted in case of disagreement.
Imaging findings were categorised as: i) ―Relevant findings related with emergency admission if the findings were directly related to the patient's reason for presenting to the emergency department (clinical information provided); ii) ―Relevant findings not related with emergency admission if the imaging findings provided relevant clinical information that required follow-up in an outpatient context but was not associated with an urgent clinical condition or the patient's reason for presenting to the emergency department; and iii) ―No relevant findings for all other cases. This variable followed a similar approach, relying on the consensus of two certified radiologists, with a third consulted in case of disagreement.
Absence of imaging abnormalities was categorised as ―No relevant findings.
Statistical Analysis: All analyses were conducted using base R version 4.4.2. Continuous variables were summarized with mean and standard deviation or median and range as appropriate. Categorical variables were summarized by frequency and percentage in each group. All data were summarized at the CT exam level. Clopper-Pearson method was used for any 95% confidence intervals presented for rates.
To assess the relationship between imaging findings and appropriateness of CT Scan request by the attending physician, a logistic regression model was fitted to the data with CT Scan appropriateness as response variable using ‘Inappropriate’ as the reference category and imaging findings as the explanatory variable with ‘Relevant findings related with emergency admission’ as the reference category. P-values and Odds Ratios with associated 95% Confidence Interval were obtained from the model. The Odds Ratio presented provides the odds of a CT exam having a relevant finding related with the emergency admission from an appropriate request vs the odds of a CT exam not having a relevant finding related with the emergency admission from an inappropriate request. Therefore, an Odds Ratio > 1 can be interpreted as a higher chance of having a relevant finding related with the emergency admission from an appropriate CT scan requested. Subgroups with 30 scans or more were explored and reported based on analysis of demographic characteristics for CT scan location and triage level at admission. All statistics presented are crude estimates. No adjustment or confounders were added into the model. P-values are reported for exploratory purposes and therefore no control for multiplicity was applied. A 5% level of significance was considered for comparisons.
Results
Patients‘ and CT exams descriptive data: in total, 360 CT examinations were analysed from 342 patients; the number of exams exceeds the number of patients because some requests included more than one anatomical region (e.g., abdomen and pelvis). The median age was 73 years (range 15-100) and the majority of patients were female (n=176, 51.5%). Most scans were requested for patients triaged as Urgent (n=253, 70.3%) according to the Manchester Emergency Triage System. CT scans were requested for 14 different anatomical regions, being Head (n=198, 55.0%), Abdominal region (superior) (n=45, 12.5%), Pelvic region (n=32, 8.9%) and Thorax (n=30, 8.3%) the most common. General surgery (n=120, 33.3%), General medicine (n=115, 31.9%) and Internal medicine (n=112, 31.1%) accounted for 96.4% of all requests.
CT scan appropriateness: The distribution of demographic and baseline data overall and by CT scan appropriateness is shown below in Table 1.
Table 1: Demographic and baseline overall and by CT scan appropriateness
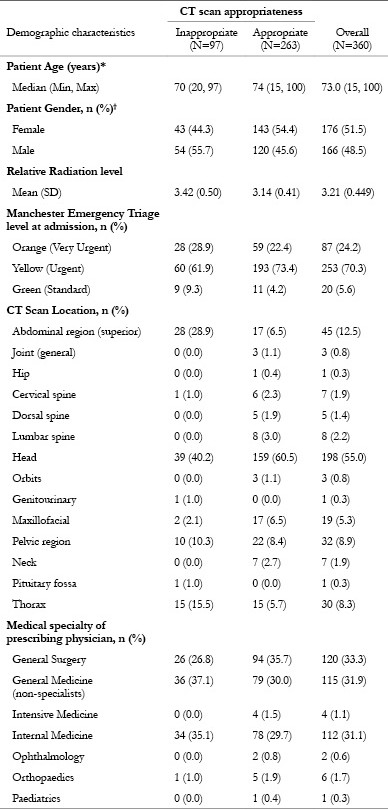
*Age was summarized at patient level
†Gender was summarized at patient level (N=342) for overall and at CT scan level by appropriateness
Ninety-seven of the 360 CT scans (26.9%, 95% CI: 22.4% to 31.8%) were classified as inappropriate. Inappropriate scans were more frequently requested for younger (median age 70 vs 74 years) and male (n=54, 55.7%) patients. Appropriate scans were more frequent among patients with higher triage levels. Of the inappropriate tests, 90.7% were classified as Orange or Yellow, compared with 95.8% of appropriate scans. Specifically, 32.1% of Orange triage scans and 23.7% of Yellow triage scans were inappropriate, while 45% of Green triage scans were deemed inappropriate. Among the most frequently requested regions, the highest proportion of inappropriate requests was observed for the upper abdomen (62.2%) and thorax (50%). Conversely, maxillofacial and head CT scans were most often appropriate, with rates of 89.5% and 80.3%, respectively.
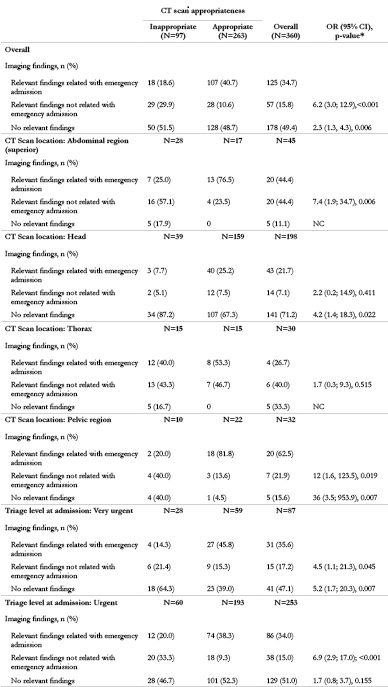
Relation between CT scan appropriateness and imaging findings: overall, a statistically significant association was observed between appropriateness of the CT request and the relevance of imaging findings (p < 0.001). Appropriately requested scans were markedly more likely to yield emergency-related findings compared with both non-emergency findings (OR [95% CI]: 6.2 [3.0-12.9]) and no relevant findings (OR [95% CI]: 2.3 [1.3-4.3]).
The same trend was observed across multiple subgroups, including selected CT scan locations and triage levels at admission, with most differences being statistically significant. Results are presented below in Table 2 overall and by selected subgroups.
Discussion
Our study demonstrated that approximately 27% of CT examinations were inappropriately requested, a finding consistent with previous research conducted in emergency settings.9,10,11,12A notably higher rate of 49% was reported by Salman S. Ahmed et al.13 Clara Singer et al. found a 25% inappropriateness rate in a multicentric European study including emergency, inpatient, and outpatient CT requests, while Felix Walther et al. reported a 40% rate in a multi-study review.14,15In our cohort, inappropriate request rates were comparable for suspected stroke (15% in our study vs. 25%) and non-traumatic head CT scans (31% in our study vs. 24%).16,17The mean ESR iGuide score in our study (7.13 ± 2.44) was higher than previously reported values (6.62 ± 2.69 and 5.2 ± 1.07).18,19The mean radiation dose (3.21 ± 0.45 mSv) was similar to that described by Osnat Luxenburg et al.20
Our data also indicated that surgeons requested fewer inappropriate imaging studies than other physicians (22% vs. 30%), aligning with prior findings.19,21Similarly, specialist physicians were less likely to request inappropriate imaging compared to non-specialists (25% vs. 31%).14,21These differences may reflect surgeons‘ more focused clinical reasoning guided by established protocols, and specialists‘ greater adherence to guidelines and experience in estimating pre-test probabilities, both contributing to more appropriate imaging use. Overall, these findings suggest that clinical expertise, diagnostic confidence, and familiarity with decision-support tools such as the ESR iGuide play a key role in optimising imaging requests. Conversely, higher rates of inappropriate requests among non-specialists may be attributed to greater diagnostic uncertainty, time pressure in emergency settings, and defensive medicine practices.
We also found that appropriately requested exams were significantly more likely to yield findings relevant to the emergency admission, with odds ratios of 6.2 and 2.3 compared to relevant non-emergency findings and non-relevant findings, respectively (p < 0.001 and p = 0.006), corroborating previous reports 9,10,11,16. This association can be explained by several factors. First, appropriate requests generally originate from well-founded clinical suspicions, reflecting a higher pre-test probability and focused diagnostic reasoning, which increase the likelihood of relevant findings. Second, guideline-based decision-support tools like the ESR iGuide help exclude low-yield indications, concentrating imaging on patients most likely to benefit. Finally, appropriateness often mirrors the overall quality of clinical decision-making, where imaging is used to confirm or rule out specific diagnoses rather than for broad screening. Together, these factors highlight the importance of promoting appropriate imaging requests to enhance diagnostic accuracy, optimise resource use, and reduce unnecessary patient radiation exposure.
Notably, multiple studies have objectively demonstrated that clinical decision support tools significantly improve the appropriateness of imaging requests. For example, Mark Baker et al. reported a reduction in inappropriate requests from 45% to 22% after implementing guidelines and local support tools. Likewise, Talya Markus et al. observed a decrease from 37% to 11%, while Clara Singer et al. documented an even greater reduction-from 30% to 3.5%-after employing the ESR iGuide.19,21,22
This study has some limitations, including its retrospective design and single-centre setting, which may limit the generalizability of the findings. Furthermore, only positive imaging findings were considered relevant, although negative results can also be clinically significant; including them would have required a more complex analysis beyond this study's scope.
These findings primarily apply to the hospital and region studied and should be generalized to other settings with caution. Nevertheless, they align with international evidence and the only comparable study conducted in Portugal, suggesting broader relevance.
Conclusion
This study highlights that a substantial proportion of CT scans requested in the emergency department are inappropriate (27%), aligning with international data. Appropriately requested imaging studies are up to six times more likely to yield findings relevant to the patient‘s emergency condition, emphasizing the critical role of clinical judgment and strict adherence to established guidelines.
Clinical decision support tools, such as the ESR iGuide, have proven effective in improving the appropriateness of imaging requests and should be more widely integrated into routine clinical practice.
Addressing inappropriate imaging requests is essential not only to enhance diagnostic accuracy and optimise resource utilization but also to reduce unnecessary patient exposure to radiation. Given the high proportion of inappropriate requests in our study, these findings are also highly relevant for hospital management, emphasizing the need to optimise resource allocation while ensuring patient safety and healthcare efficiency. Future initiatives should prioritize targeted education, guideline implementation, and the integration of decision-support systems to foster more rational, evidence-based, and cost-effective imaging use in emergency settings.

