











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Introduction
Gadolinium-based contrast agents (GBCAs) are widely used in magnetic resonance imaging (MRI) due to their efficacy and generally favorable safety profile.1 These agents consist of highly toxic gadolinium ion chelated by ligands forming either linear or macrocyclic structures.1 Commonly available GBCAs in Europe include gadobutrol (Gadovist®), gadoteric acid (Dotarem®), disodium gadoxetate (Primovist®), and gadodiamide (Omniscan®.).1
Although adverse reactions to GBCAs are infrequent, immediate hypersensitivity reactions, including anaphylaxis, have been reported with an estimated incidence of 0.01% to 0.1% per administration.2 Recent data estimates indicate an overall incidence of immediate GBCA reactions of <0.1%, with higher risk in patients with a prior reaction. Current recommendations for management and prevention are detailed in the ACR Manual on Contrast Media (2024) and the ESUR Guidelines (2025).3,4,5
Data from pharmacovigilance databases and multiple case reports confirm that all types of GBCAs, including macrocyclic agents such as gadobutrol can elicit severe immediate reactions.6,7,8,9 While the underlying mechanisms remain incompletely understood, evidence from positive skin tests supports the hypothesis of IgE-mediated pathways in some patients.10,11 The aim of this study was to describe a case series of patients with immediate hypersensitivity reactions to gadolinium-based contrast agents, focusing on the clinical presentation, skin test results, and tolerance to alternative agents, to contribute to the understanding and management of GBCAs allergy in clinical practice.
Case Presentation
We present a case series of four patients who experienced immediate reactions to gadobutrol, ranging from cutaneous symptoms to anaphylaxis. All underwent systematic allergological evaluation, which confirmed sensitization and enabled the identification of safe alternative contrast agents for future imaging procedures.
Demographic and clinical characteristics of the patients are described in Table 1. Four patients (2 females, 2 males) were included; mean age was 65.8 years (range: 56-87). Three patients experienced an anaphylactic reaction during contrast-enhanced MRI with gadobutrol.
According to Table 1, one reaction was classified as Grade 2, two as Grade 3 and one as Grade 4, based on the Ring and Messmer severity scale.11 Clinical features observed during the reaction included hypotension (n=3), urticaria (n=2), angioedema (n=1), and cardiorespiratory arrest (n=1). One patient also presented with syncope and desaturation. All patients received intravenous treatment with clemastine and hydrocortisone and intramuscular adrenaline was administered to three patients.
Table 1: Overview of case report presentations
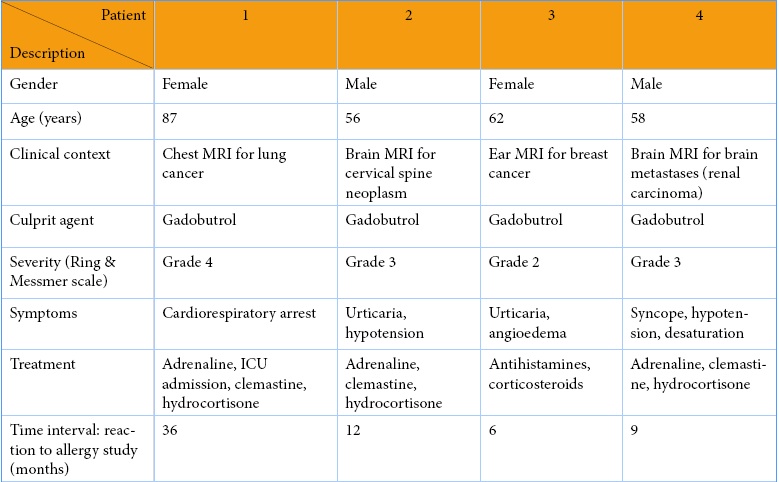
MRI: Magnetic Resonance Imaging; ICU: Intensive Care Unit
One patient required intensive care unit admission. The interval between the hypersensitivity reaction and allergological evaluation ranged from 6 to 36 months (mean 15.75).
Table 2 and Figure 1 detail the individual diagnostic investigation performed in our Immunoallergology Department.
Table 2: Skin prick test (SPT) and intradermal test (IDT) results with gadolinium-based contrast agents
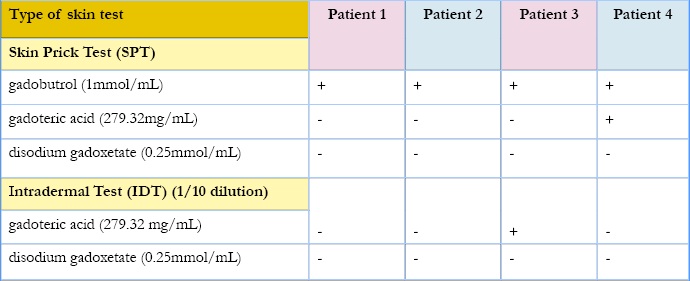
+ positive; - negative
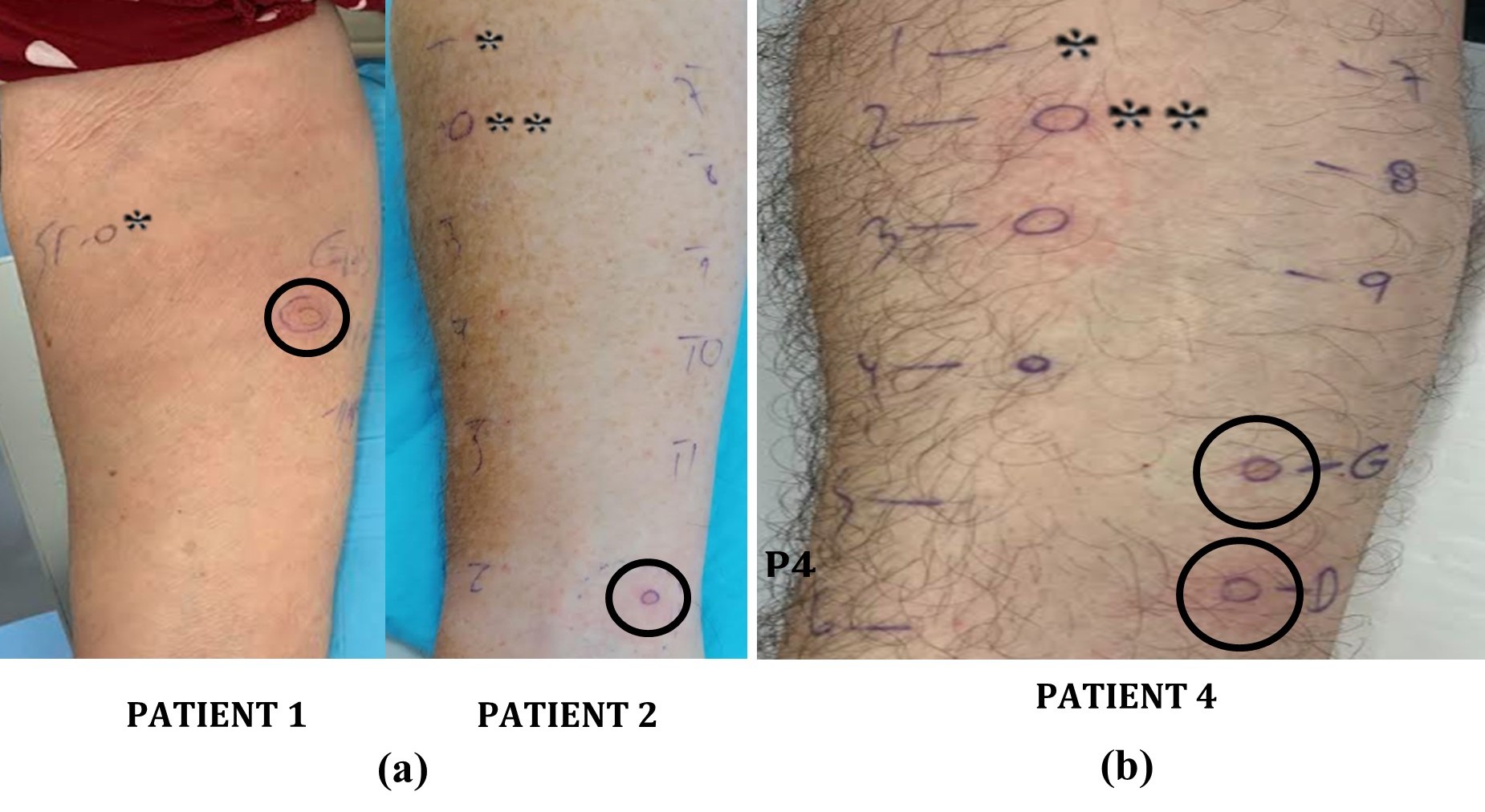
Figure 1: Positivity of skin prick tests. a) to the GBCA gadobutrol (circle) for Patient1 and Patient2; b) to the Gadolinium-Based Contrast Agents (GBCAs) gadobutrol and gadoteric acid (circles) for P4. *: saline;** histamine
Regarding gadobutrol hypersensitivity diagnostic investigation, skin tests were positive in all four patients: skin prick tests with gadobutrol (1 mmol/mL) were positive in 4/4 patients. Intradermal tests with gadobutrol were not performed as skin prick tests with this contrast agent were positive.
Two patients showed positive skin test results to gadoteric acid-one in the skin prick test and another in the intradermal test with a 1:10 dilution (279.32 mg/mL). The remaining two patients had negative skin tests for gadoteric acid. Skin prick and intradermal tests with a 1:10 dilution of disodium gadoxetate (0.25 mmol/mL) were negative in all patients, and disodium gadoxetate was tolerated in all cases during magnetic resonance imaging.
Discussion
Gadolinium-based contrast agents are widely used in MRI procedures due to their favorable safety profile; however, immediate hypersensitivity reactions including anaphylaxis, though rare, can be life-threatening.1,3 While macrocyclic agents like gadobutrol are considered less immunogenic compared to linear compounds, growing evidence shows that they can still trigger severe allergic reactions.6,9
In our series, four patients experienced immediate reactions to gadobutrol, ranging from cutaneous manifestations to severe anaphylaxis. We used the Ring and Messmer grading system (grades II-IV), which is standard in allergology. For clarity, we provide the parallel with the ACR classification: Ring and Messmer grade II corresponds to moderate ACR reactions, while grades III-IV correspond to severe ACR reactions. All had positive skin prick tests (SPT) to gadobutrol, consistent with a IgE-mediated mechanism. Although skin testing for GBCAs is not yet standardized, several studies and reviews support its diagnostic value in identifying sensitization and predicting tolerance to alternative agents.10,11
Skin prick tests (SPT) are useful for assessing IgE-mediated hypersensitivity with high specificity, whereas intradermal tests (IDT) are more sensitive but less specific and associated with higher risk of local irritation. In our protocol, SPTs are performed first, with IDTs reserved for negative or equivocal SPTs. Graded intravenous challenges may be considered after negative SPT/IDT results when contrast-enhanced imaging is essential but should only be conducted in a monitored hospital setting. In the present series, all four patients had positive SPTs to gadobutrol; therefore, IDTs with gadobutrol were not performed. For disodium gadoxetate, both SPTs and IDTs (1:10 dilution) were negative in all cases, and this agent was subsequently used during MRI under monitoring without adverse reactions. The mean interval between the reaction and allergological evaluation was 15.75 months (range: 6-36), mainly due to referral and institutional availability. This delay may reduce the sensitivity of diagnostic tests, and we acknowledge it as a limitation. Whenever necessary, alternative imaging strategies or the use of a tested safe agent were prioritized to avoid compromising oncological decision-making. Interestingly, two patients also reacted to gadoteric acid, another macrocyclic GBCA, suggesting potential cross-reactivity. This challenges the assumption that all macrocyclic agents are safe alternatives once sensitization to one is established.14 While the exact chemical determinants of cross-reactivity remain undefined, published cases have documented similar findings, reinforcing the need for individualized testing.9,11,14
Conversely, all patients tolerated disodium gadoxetate, a linear GBCA traditionally associated with a higher risk of nephrogenic systemic fibrosis and possibly of allergic reactions.1 In our cases, skin testing was negative, and no clinical reactions occurred upon exposure, highlighting that linear agents may be used safely in selected patients when macrocyclic cross-reactivity is suspected or confirmed. In Europe, non-hepatobiliary linear GBCAs were suspended in 2017, with exceptions maintained for disodium gadoxetate (for hepatobiliary imaging) and for agents used in MR arthrography.15 In our series, disodium gadoxetate tested negative (SPT/IDT) and was safely administered, supporting its continued practical role as an available and regulated alternative. Our results are consistent with previously published series, where substitution with structurally distinct contrast agents, guided by allergological evaluation, allowed safe completion of subsequent imaging studies. Recent reviews reinforce the importance of a systematic and interdisciplinary approach to prevent recurrence.13
Literature on GBCA-related anaphylaxis has grown, including data from pharmacovigilance systems, individual case reports, and expert guidelines.6,11,13 This underscores the importance of accurate identification of the culprit agent, as well as careful consideration of alternatives. Systematic allergological assessment including detailed clinical history, skin testing with culprit and alternative agents, and, in some cases, graded drug challenges can optimize patient safety and preserve access to necessary imaging.9,10,11 When no safe GBCA can be identified, desensitization protocols may be considered in specialized centers after multidisciplinary evaluation and informed consent. Testing for iodinated contrast agents in patients without prior exposure is not a routine and should only be considered when iodinated contrast administration is clinically indicated and no safe gadolinium-based option is available.12
Clinicians should also be aware of non-IgE-mediated pathways, as some reactions to contrast agents may involve complement activation or direct mast cell triggering. Nonetheless, in the presence of positive skin tests and rapid onset of symptoms, IgE-mediated hypersensitivity is the most probable mechanism.8,11
This study has several important limitations: (i) variable and relatively long interval between reaction and allergological evaluation; (ii) absence of intravenous provocation testing in cases with negative SPT and; (iii) in our series, it was not possible to confirm whether all patients were exposed within the same imaging department, nor to determine the precise time interval between the first and last reaction. Therefore, we cannot exclude the potential contribution of external procedural factors, including batch-related issues, storage conditions, or administration variables (e.g., temperature or injection speed), which may have influenced the occurrence of these clustered cases.
Conclusion
Immediate hypersensitivity reactions to gadobutrol, including severe anaphylaxis, can occur despite its macrocyclic and non-ionic structure. In all four cases presented, skin testing proved valuable in confirming sensitization and identifying safe alternatives. These findings highlight the importance of individualized allergological assessment in patients with suspected GBCA allergy. Clinically, this approach allows safe imaging while reducing the risk of repeated exposure. Cross-reactivity among macrocyclic agents may occur, underscoring the need for testing rather than assumptions based on structure alone. Disodium gadoxetate may be a safe alternative in selected cases, though tolerance should always be verified through testing.

