











 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
Permalink
Case Presentation
A 12-year-old male patient presented with one-month history of left anterior knee pain that started after a sprint, without history of trauma or surgery. Clinical examination revealed localized tenderness over the lateral patellar border and anterior tibial tuberosity, preserved range of motion, and no signs of dislocation.
Radiography showed mild heterogeneity of the anterior tibial tuberosity with adjacent soft-tissue prominence, consistent with Osgood-Schlatter disease, and a thin calcific fragment adjacent to the lateral patellar margin suspicious for patellar avulsion (Fig.1). MRI (Magnetic Resonance Imaging) demonstrated marked bone marrow edema of the lateral patella, thickening and hyperintensity of the lateral retinacular insertion and periosteal avulsion with a small adjacent bone fragment consistent with an avulsion fracture. Also, ill-defined bone marrow edema in the medial femoral condyle, raising the possibility of a transient medial patellar dislocation, even though clinical history was not suggestive (Fig. 2). Edema of suprapatellar and Hoffa’s fat pads were associated. Additional important findings included patellar tendon thickening with infrapatellar bursitis, and tibial tuberosity edema consistent with Osgood-Schlatter disease (Fig. 2). There was no evidence of trochlear dysplasia.
The final diagnosis was avulsion fracture of the lateral patellar retinacular insertion in the context of a possible medial patellar transient dislocation, coexisting with active Osgood-Schlatter disease. Conservative management was recommended including immobilization with knee brace, rest, cryotherapy and anti-inflammatory drugs initially, followed by progressive activity increase and physical therapy with focus on strengthening the vastus lateralis.
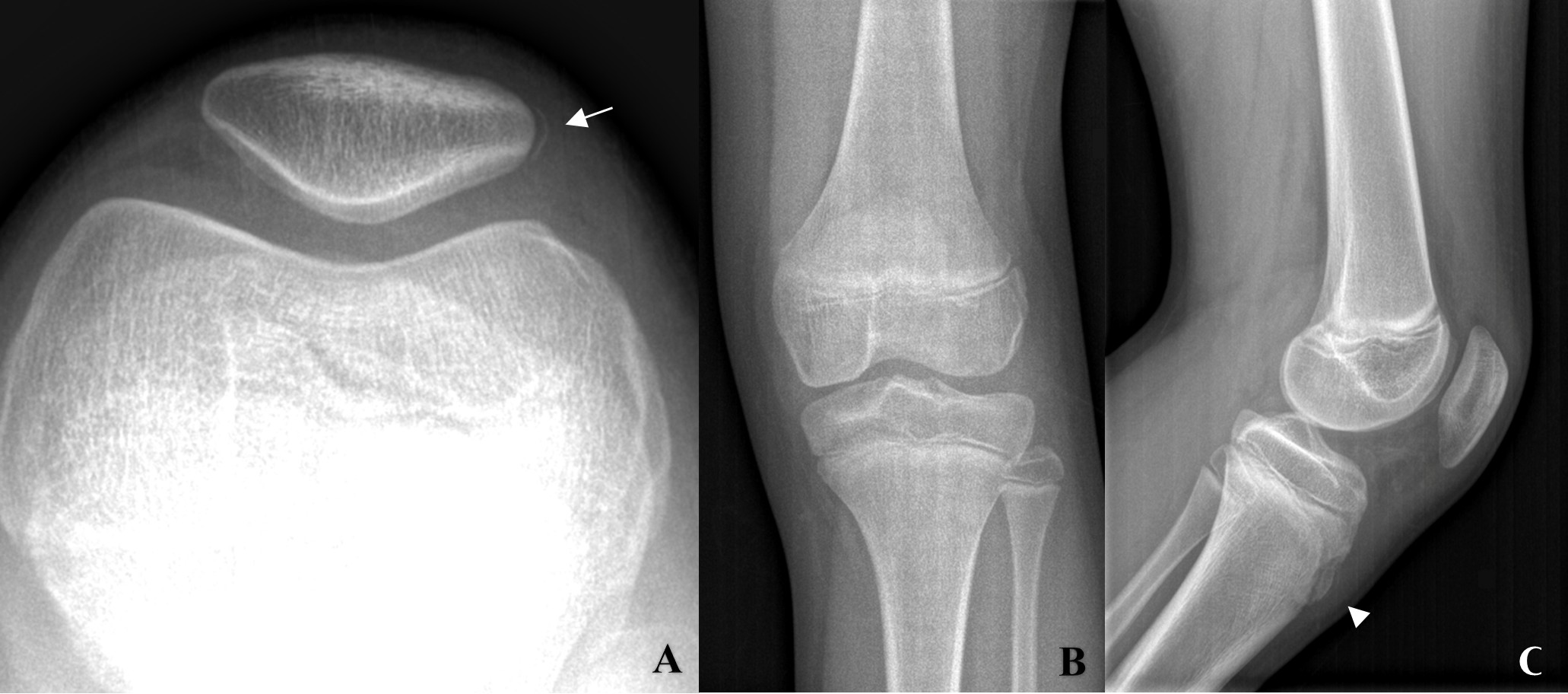
Figure 1: Left knee radiographs. Axial patellar (Merchant) view (A) demonstrates a small curvilinear calcific fragment adjacent to the lateral border of the patella (arrow), compatible with an avulsion fracture at the lateral retinacular insertion. Anteroposterior view (B) shows no significant abnormalities. Lateral projection (C) depicts preserved patellofemoral alignment without evidence of patella alta. Mild heterogeneity of the anterior tibial tuberosity with adjacent soft tissue density is seen (arrowhead), favoring Osgood-Schlatter disease.
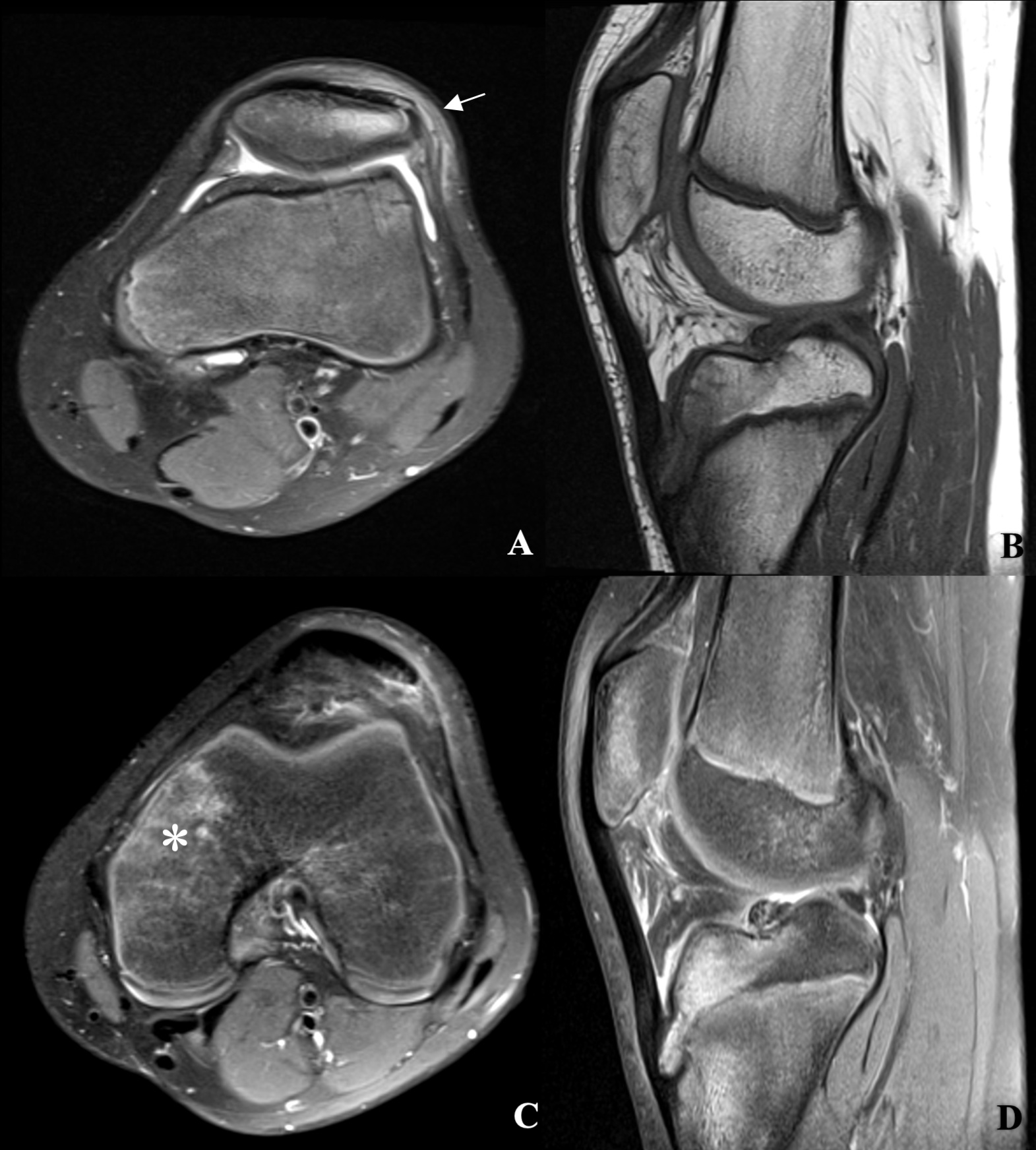
Figure 2: MRI of the left knee. Axial fat-suppressed proton-density-weighted images (A and C) show marked bone marrow edema in the lateral patella with thickened and hyperintense lateral retinaculum at its patellar insertion associated with avulsion the ligamentous insertion (arrow), confirmed to include a small fragment of bone in the previously showed radiography (Fig.1A). No significant chondral involvement was present (A). Edema in the surrounding soft tissue is also seen. The more inferior axial image (C) depicts ill-defined bone marrow edema in the medial aspect of the medial femoral condyle (asterisk), most likely post-traumatic in nature, which, taken together with the other findings, suggests the occurrence of a transient medial patellar dislocation. There were no signs suggestive of trochlear dysplasia (not shown: Wiberg type I patella, with a trochlear depth of 6 mm, lateral trochlear inclination of 15°, trochlear angle of 139° and a normally positioned patella (Insall-Salvati index 1.12 and Caton-Deschamps index of 1.2). Sagittal T1 (B) and fat-suppressed proton-density-weighted (D) images demonstrate thickening and hyperintensity of the distal third and patellar insertion of the patellar tendon, associated with edema of the adjacent subcutaneous fat as well as distension of the deep infrapatellar bursa. There is also mild structural heterogeneity of the anterior tibial tuberosity associated with moderate bone marrow edema, which is consistent with Osgood-Schlatter disease.
Discussion
Patellofemoral stability depends on the integration of osseous morphology, dynamic muscular control, and soft-tissue restraints, including the medial and lateral retinacula.1,2 While the medial patellofemoral ligament (MPFL) has been extensively studied, less attention has been paid to the lateral patellofemoral retinacula that includes the lateral patellofemoral ligament (LPFL), the lateral patellotibial ligament, the lateral patellomeniscal ligament, bands of the vastus lateralis obliquus, the quadriceps aponeurosis, and the iliotibial band.1,2 These structures act as important secondary restraints, contributing to the resistance of medial translation of the patella and maintaining joint balance, particularly in early flexion.3
Most clinical reports of lateral retinacular pathology involve iatrogenic excessive medialization of the tibial tubercle, over constricted MPFL or, more frequently, insufficiency following lateral release procedures, where weakening of the retinaculum predisposes to medial patellar instability.1,3 In contrast, non-iatrogenic avulsion of the lateral retinaculum as in our clinical case is exceedingly rare in the literature, with a small number of cases reported.4,5
Identifying these lesions radiographically can be very helpful because the avulsed fragments are frequently small and may not be visible on MRI. Otherwise, MRI provides the most reliable assessment demonstrating bone marrow edema, signs of lesion of the retinaculum, and evidence of periosteal or chondral avulsion.4,5 Correlation of radiographs and MRI is essential to confirm the diagnosis and avoid misinterpretation. This scenario is a good example of the potential utility of MRI CT-like sequences, that could better depict the bone fragment, mainly when radiographs or CT are not available. Our patient also had bone marrow edema of the medial femoral condyle, a finding that supports the mechanism of a transient medial patellar dislocation.
In our clinical case we could not objectify the etiology of the lateral retinaculum lesion since potential causes referred in the literature were not present in our clinical history, such as iatrogenic, direct trauma, congenital or hypermobility diseases.11 However, one case in the literature also refers that patient´s symptoms started suddenly after a sprint as in our case.5
Osgood-Schlatter disease, a traction-related apophysitis of the tibial tuberosity in adolescents, typically presents with marrow edema, thickening of the patellar tendon, infrapatellar bursal inflammation and ossification center fragmentation.6,7 Its overlap with the rare avulsion fracture can complicate the clinical diagnostic interpretation of anterior knee pain. In our clinical case, imaging and clinical examination were compatible with coexisting active Osgood-Schlatter disease.
Differential diagnoses in this scenario would include Osgood-Schlatter disease, Sinding-Larsen-Johansson syndrome, patellar stress fracture, symptomatic bipartite patella, Iliotibial band friction syndrome, patellar tendon-lateral femoral condyle friction syndrome and meniscal pathology, all of which can overlap clinically but have distinct imaging features.
Given the rarity of this lesion, no standard treatment is established to our knowledge. Considering the same principles used for MPFL acute bony avulsion lesion and LPFL iatrogenic injury, non-operative treatment can be tried for small minimally displaced avulsions without cartilage involvement. Physical therapy to strengthen the vastus lateralis is recommended. Surgical intervention, including ligament reconstruction or repair and medial retinacular release, may be considered for symptomatic patients with persistent instability. Prompt diagnosis and treatment is critical to avoid long-term complications such as instability, abnormal patellar tracking, and premature degenerative changes.8,9,10
This case highlights a rare lateral retinacular avulsion fracture with coexisting active Osgood-Schlatter disease, emphasizing the importance of combined radiographic and MRI evaluation in adolescents with anterior knee pain. Awareness of this entity is crucial to avoid misinterpretation on imaging, allowing a timely and appropriate management.

